



The 3rd International Nursing and Health Sciences Students and Health Care Professionals Conference (INHSP)
More infoThis study aimed to analyze the parameters of antenatal care, which becomes a risk factor against the incidence of preeclampsia in primigravidae in Kolaka.
MethodsThe study uses case–control studies (case–control), which use a retrospective approach. The population in this study were all primigravida pregnant women recorded in the medical records at the BLUD Hospital. HM Djafar Harun as many as 5796 women and BLUD Benyamin Guluh Hospital as many as 5065 women. The sample in this case group is the primary mother Gravida, who suffered from preeclampsia from January 2014 to September 2018, and the control group was primigravida mothers who did not suffer from preeclampsia in the same period.
ResultsThe results showed that the age of primigravida mothers 14–28 years had a risk of 1.581 times more significant for having preeclampsia than the age group 29–49 years with CI (1.186–2.108), the incidence of hypertension in trimester 1 in primigravida mothers had a risk of 3.405 times greater for preeclampsia than mothers without a history of hypertension in trimester 1 with CI (2.164–5.358), irregular antenatal visits are 1.095 times more likely to develop preeclampsia than regular antenatal visits with CI (0.799–1.539), weight gain primigravida maternal body 1–10kg 1.540 times greater risk of developing preeclampsia than 10–20kg of weight gain with CI (1.074–2.207), pregnancy checks according to Antenatal Care non-compliant care standards are 1.333 times more likely to develop preeclampsia than primigravida mothers who obediently do the inspection antenatal care with CI (0.970–1.831).
ConclusionVariables that are very risky with preeclampsia in primigravida mothers based on multivariate analysis are the hypertension incidence in the first trimester with an OR: 3.363 with a CI value of 2.126 and a lower value of 5.318.
Preeclampsia is a disease in pregnant women which is characterized by high blood pressure and proteinuria in pregnancy >20 weeks which occurs in 2–8% of pregnancies.1,2 WHO (World Health Organization) estimates the incidence of preeclampsia to be seven times higher in developing countries (2.8% of live births) compared to developed countries (0.4%) and is a leading cause of maternal, fetal, and neonatal death, especially in low- and middle-income countries.3,4
According to WHO preeclampsia affects seven to ten percent of all pregnancies in the United States. In the UK, less than 10 women die from preeclampsia each year, affecting maternal mortality. In the least developed countries, there are 50,000 maternal deaths caused by preeclampsia and eclampsia. On the other hand, the incidence of eclampsia in developing countries is around 1 case per 100 pregnancies to 1 case per 1700 pregnancies. In African countries such as South Africa, Egypt, Tanzania Ethiopia dam varies from 1.8% up to 7.1%. In Nigeria, the prevalence is about 2% up to 16.7%3.
Primiparity, early age of menarche (12 years), preobese, obesity, age >30 years, multiple pregnancies, anemia, previous preeclampsia, Diabetes mellitus, chronic hypertension, acute kidney disease, family history of hypertension are risk factors that increase the incidence of preeclampsia.5–7 Bodnar et al. (2015) suggest the measurement of fat mass to recognize preeclampsia in obese women because the results of their study indicate that an increase in body mass index (BMI) in the normal range is also associated with an increased risk of preeclampsia.8
According to Tigor H. Situmora research, 2016 with the results, there is a relationship between age, knowledge, and the incidence of preeclampsia, and there is no relationship between parity, history of hypertension, antenatal care examination with the incidence of preeclampsia in pregnant women in the MCH clinic (maternal and child health) Anutapura General Hospital Palu.9
This research is important to compare the history of ANC (antenatal care) examination between primigravida mothers who have preeclampsia and those not affected by preeclampsia based on ANC (antenatal care) examination parameters, to see whether ANC (antenatal care) can be a predictor of preeclampsia in primigravida. Based on this, the purpose of this study is to analyze the antenatal care parameters that are predictors of risk factors for the incidence of preeclampsia in primigravida in the Kolaka Regency.
Research methodsTypes and designs were used case-control study and have accepted ethical approval from the ethical committee of medicine faculty, Hasanuddin University.
Population and sample techniquesThe population in this study were all primigravida pregnant women recorded in the medical record data at the BLUD Hospital. HM Djafar Harun as many as 5796 women and BLUD Benyamin Guluh Hospital as many as 5065 women. The sample in this study was a primigravida mother suffering from preeclampsia recorded in the medical record data at the BLUD Hospital. HM Djafar Harun and BLUD Hospital Benyamin Guluh for the period of 2014 to September 2018. The sample in this study were all primigravida mothers recorded in the medical record at the BLUD Hospital. HM Djafar Harun and BLUD Hospital. Benjamin Guluh period 2014 to September 2018. Data obtained from hospitals either of the cases or the control group, then draw the case and control groups through the mother's name were obtained from the sampling frame patient's medical record antenatal care in hospitals Djafar Harun period from 2014 until September 2018 as many samples required in research which is the category of cases as many as 179 people and a control group of 179 people and BLUDs RS Benjamin Guluh period from 2014 until September 2018 as many samples required in research which is the category of cases as many as 248 people and a control group as many as 248 people.
Data analysisData analysis was performed using bivariate and multivariate analysis.
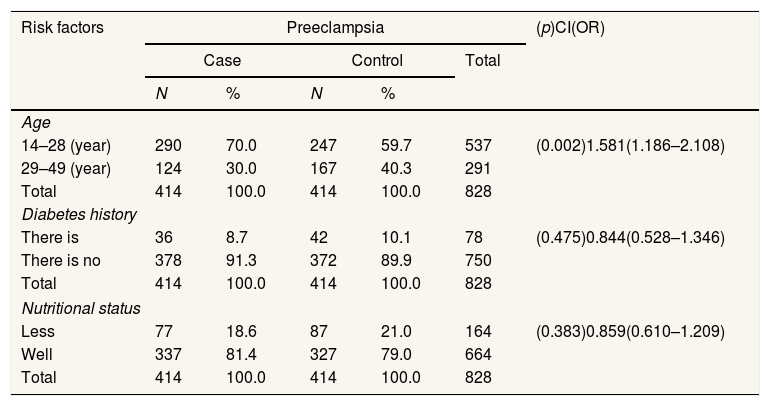
ResultsThe results showed that the age of primiparous mothers 14–28 (year) was at risk 1.581 times, compared with the age of mothers 29–49 (year) with a range 1.186–2.108 times. Thus it can be concluded that there was a mother's age at risk preeclampsia in primigravida mothers, and a p-value (0.002) <0.005 indicates a relationship between maternal age and the incidence of preeclampsia in primigravida mothers (Table 1).
Risk factors for the incidence of preeclampsia in primigravida based on age, history of diabetes, and nutritional status in BLUD RSHHDjafar Harun and BLUD RS. Benjamin Guluh of Kolaka Regency.
| Risk factors | Preeclampsia | (p)CI(OR) | ||||
|---|---|---|---|---|---|---|
| Case | Control | Total | ||||
| N | % | N | % | |||
| Age | ||||||
| 14–28 (year) | 290 | 70.0 | 247 | 59.7 | 537 | (0.002)1.581(1.186–2.108) |
| 29–49 (year) | 124 | 30.0 | 167 | 40.3 | 291 | |
| Total | 414 | 100.0 | 414 | 100.0 | 828 | |
| Diabetes history | ||||||
| There is | 36 | 8.7 | 42 | 10.1 | 78 | (0.475)0.844(0.528–1.346) |
| There is no | 378 | 91.3 | 372 | 89.9 | 750 | |
| Total | 414 | 100.0 | 414 | 100.0 | 828 | |
| Nutritional status | ||||||
| Less | 77 | 18.6 | 87 | 21.0 | 164 | (0.383)0.859(0.610–1.209) |
| Well | 337 | 81.4 | 327 | 79.0 | 664 | |
| Total | 414 | 100.0 | 414 | 100.0 | 828 | |
Secondary data sources 2019.
Mothers with a history of diabetes have a risk of 0.844 times, compared to mothers who do not have a history of diabetes in the range 0.528–1.346. Thus it can be concluded that the history of maternal diabetes is not at risk of preeclampsia in primigravida mothers, and a p-value is obtained (p 0.475)>0.005, which indicates that there is no relationship between maternal diabetes history and the incidence of preeclampsia in primigravida mothers (Table 1).
Nutritional status is less risk 0.859 times, compared to good nutritional status with a range 0.610–1.209, thus it can be concluded that nutritional status is not at risk for preeclampsia in primigravida mothers, and a p-value (0.838)>0.005 indicates that there is no relationship between nutritional status and the incidence of preeclampsia in primigravida mothers (Table 1).
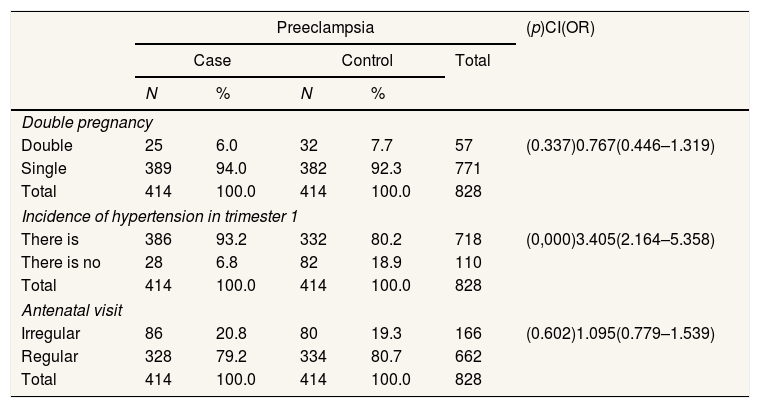
Table 2 shows that Multiple Pregnancy has a risk of 0.767 times, compared to a Single Pregnancy with a range 0.446–1.319. Thus, it can be concluded that Multiple Pregnancy is not at risk for preeclampsia in primigravida mothers. Furthermore, a p-value (0.337)>0.005 shows no relationship between multiple maternal pregnancies and the incidence of preeclampsia in primigravida mothers.
Risk factors for preeclampsia in primigravida based on multiple pregnancies, the incidence of hypertension and antenatal visits in BLUD RS. HMDjafar Harun and BLUD Hospital. Benjamin Guluh of Kolaka Regency.
| Preeclampsia | (p)CI(OR) | |||||
|---|---|---|---|---|---|---|
| Case | Control | Total | ||||
| N | % | N | % | |||
| Double pregnancy | ||||||
| Double | 25 | 6.0 | 32 | 7.7 | 57 | (0.337)0.767(0.446–1.319) |
| Single | 389 | 94.0 | 382 | 92.3 | 771 | |
| Total | 414 | 100.0 | 414 | 100.0 | 828 | |
| Incidence of hypertension in trimester 1 | ||||||
| There is | 386 | 93.2 | 332 | 80.2 | 718 | (0,000)3.405(2.164–5.358) |
| There is no | 28 | 6.8 | 82 | 18.9 | 110 | |
| Total | 414 | 100.0 | 414 | 100.0 | 828 | |
| Antenatal visit | ||||||
| Irregular | 86 | 20.8 | 80 | 19.3 | 166 | (0.602)1.095(0.779–1.539) |
| Regular | 328 | 79.2 | 334 | 80.7 | 662 | |
| Total | 414 | 100.0 | 414 | 100.0 | 828 | |
Secondary data sources 2019.
The incidence of hypertension in trimester 1 has a risk of 3.405 times, compared to not having a history of hypertension in the range 2.164–5.358. Thus, it can be concluded that hypertension events in trimester 1 have a risk of preeclampsia in primigravida mothers, and a p-value (0.000)<0.005 indicates a relationship between the incidence of hypertension in trimester 1 to the incidence of preeclampsia in primigravida mothers.
Irregular antenatal visits risk 1.095 times, compared to regular visits with a range 0.779–1.539. Thus, it can be concluded that antenatal visits are at risk of preeclampsia in primigravida mothers, and a p-value (0.602)>0.005 indicates no relationship between maternal antenatal visits and the incidence of incidence preeclampsia in primigravida mothers.
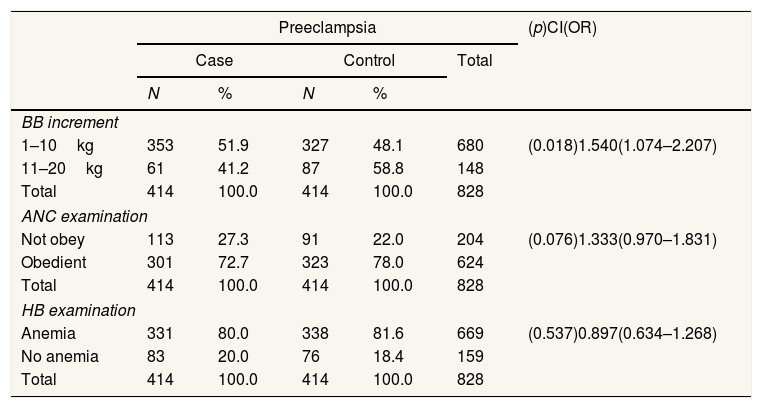
Table 3 shows that weight gain of 1–10kg has a risk of 1.540 times, compared to a weight gain of 10–20kg with a range of 1.074–2.207. Thus it can be concluded that weight gain is at risk of preeclampsia in primigravida mothers and is obtained p (0.000)<0.005. This indicates a relationship between BB increase and the incidence of preeclampsia in primigravida mothers.
Risk factors for preeclampsia in primigravida based on weight gain in BLUD Hospital. HMDjafar Harun and BLUD Hospital. Benjamin Guluh of Kolaka Regency.
| Preeclampsia | (p)CI(OR) | |||||
|---|---|---|---|---|---|---|
| Case | Control | Total | ||||
| N | % | N | % | |||
| BB increment | ||||||
| 1–10kg | 353 | 51.9 | 327 | 48.1 | 680 | (0.018)1.540(1.074–2.207) |
| 11–20kg | 61 | 41.2 | 87 | 58.8 | 148 | |
| Total | 414 | 100.0 | 414 | 100.0 | 828 | |
| ANC examination | ||||||
| Not obey | 113 | 27.3 | 91 | 22.0 | 204 | (0.076)1.333(0.970–1.831) |
| Obedient | 301 | 72.7 | 323 | 78.0 | 624 | |
| Total | 414 | 100.0 | 414 | 100.0 | 828 | |
| HB examination | ||||||
| Anemia | 331 | 80.0 | 338 | 81.6 | 669 | (0.537)0.897(0.634–1.268) |
| No anemia | 83 | 20.0 | 76 | 18.4 | 159 | |
| Total | 414 | 100.0 | 414 | 100.0 | 828 | |
Secondary data sources 2019.
Non-compliant ANC examination has a risk of 1.333 times, compared to compliant ANC examination with a range 0.970–1.831. Thus it can be concluded that the ANC examination is at risk of preeclampsia in primigravida mothers, and obtained p values (0.076)>0.005 things this shows that there is no relationship between ANC examination and the incidence of preeclampsia in primigravida mothers.
Non-anemia HB examination has a risk of 0.879 times, compared to hemoglobin examination with a range 0.634–1.268. Thus it can be concluded that HB examination is not at risk of preeclampsia in primigravida mothers, and obtained p values (0.537)>0.005. This shows that there is no relationship between HB examination and the incidence of preeclampsia in primigravida mothers.
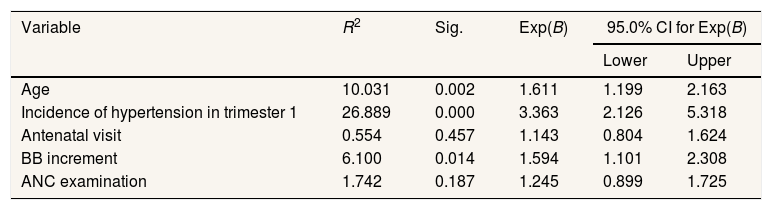
Table 4 shows the results of multivariate analysis using logistic regression for the five variables it appears that the variables that most influence the incidence of preeclampsia in primigravida at the BLUD Hospital. HM Djafar Harun and BLUD Hospital. Benjamin Guluh, Kolaka, namely the variable hypertension in trimester 1 with an OR: 3.363 with a CI value of 2.126 and an upper value of 5.318.
Parameters of the become predictor antenatal care risk factor against genesis preeclampsia in primigravidae in BLUDs RS. HMDjafar Harun and BLUD Hospital. Benjamin Guluh of Kolaka Regency.
| Variable | R2 | Sig. | Exp(B) | 95.0% CI for Exp(B) | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Age | 10.031 | 0.002 | 1.611 | 1.199 | 2.163 |
| Incidence of hypertension in trimester 1 | 26.889 | 0.000 | 3.363 | 2.126 | 5.318 |
| Antenatal visit | 0.554 | 0.457 | 1.143 | 0.804 | 1.624 |
| BB increment | 6.100 | 0.014 | 1.594 | 1.101 | 2.308 |
| ANC examination | 1.742 | 0.187 | 1.245 | 0.899 | 1.725 |
The results showed that the age of primiparous mothers 14–28 years had a risk of 1.581 times, compared to the age of mothers 29–49 (year) with a range 1.186–2.108 times. These results concur with his research finding that preeclampsia is more common at age >35 years.10 Age is one of the factors that can determine the health of pregnant women. Nevertheless, in preeclampsia, age is not the only risk factor for the emergence of preeclampsia, but there are other factors such as nullipara, multiple pregnancies, obesity, history of the disease, genetic and preeclampsia in previous pregnancies.5,11
Mothers with a history of diabetes have a risk of 0.844 times, compared to mothers who do not have a history of diabetes in the range 0.528–1.346. Thus it can be concluded that the history of maternal diabetes is not at risk for preeclampsia in primigravida mothers.
Nutritional status is less risky 0.859 times, compared to good nutritional status with a range 0.610–1.209. Other studies have shown that assessing the nutritional status of pregnant women includes evaluating risk factors, diet, anthropometric measurements, and biochemistry.12 For example, a cohort study found that mothers with a body mass index >35 had a doubled risk of developing preeclampsia. Another study comparing mothers with low and normal body mass index found that the risk of preeclampsia decreased dramatically in mothers with a body mass index <20.13
Multiple pregnancies have a risk of 0.767 times, compared to single pregnancies with a range 0.446–1.319. Thus it can be concluded that multiple pregnancies are not at risk for preeclampsia in primigravida mothers. However, when a mother contains more than one fetus in her womb, the mother's risk of experiencing preeclampsia increases almost threefold. For example, one study showed that pregnant women with three fetuses had a threefold greater risk of developing preeclampsia than those with two fetuses.14
The incidence of hypertension in trimester 1 has a risk of 3.405 times, compared to not having a history of hypertension in the range 2.164–5.358. Thus it can be concluded that the incidence of hypertension in trimester 1 is at risk of preeclampsia in primigravida mothers. Furthermore, a history of chronic hypertension experienced during pregnancy can increase the risk of hypertension in pregnancy, where complications can result in superimposed preeclampsia and chronic hypertension in pregnancy.15
Irregular antenatal visits have 1.095 times more risk than regular visits with ha range 0.779–1.539. Thus it can be concluded that antenatal visits are at risk of preeclampsia in primigravida mothers. Pregnancy examination or ANC (antenatal care) is an examination of pregnant women both physically and mentally. It saves mothers and children in pregnancy, childbirth, and puerperium to be healthy and normal postpartum, both physically and emotionally.16
Weight increase in 1–10kg has a risk of 1.540 times, compared with an increase in body weight of 10–20kg with a range 1.074–2.207. Thus it can be concluded that the increase in body weight risk for preeclampsia in primigravida mothers, and the value of p (0.000)<0.005 indicates that there is a relationship between BB increase and the incidence of preeclampsia in primigravida mothers.
Non- compliant ANC examination has a risk of 1.333 times, compared to compliant ANC examination with a range 0.970–1.831. Thus it can be concluded that the ANC examination is at risk of preeclampsia in primigravida mothers. ANC services affect preeclampsia incidence because ANC services are still not maximized provided to pregnant women. Routine ANC services include at least four visits in each trimester (at least once in the first trimester, once in the second trimester, and twice in the third trimester of gestational age).17
Non-anemia has a risk of 0.879 times, compared to anemia with a range 0.634–1.268. Thus it can be concluded that HB examination is not at risk of preeclampsia in primigravida mothers. The average HB level of pregnant women is 10.72%. This level is lower than the average non-pregnant mother (11.47g/%). Pregnant women with low HB levels will cause some complications that will occur. Normal pregnancy results in a slight decrease in hemoglobin concentration due to hemodilution, a physiological adaptation in pregnancy. Therefore, hemoglobin concentration alone cannot be used to diagnose iron deficiency.18 However, the hemoglobin concentration should be measured, even though not all anemia is caused by iron deficiency.19
ConclusionBased on the results and the discussion, it can be concluded that the variables maternal age, the incidence of hypertension in the first trimester, antenatal visits, added weight, and examination of pregnancy according to the standard of service antenatal care risky with the incidence of preeclampsia in primigravida in BLUDs RS. HM Djafar Harun and BLUD Benyamin Guluh Hospital in Kolaka Regency. Variables history of diabetes, multiple pregnancies, nutritional status, pregnancy examination, hemoglobin examination are not at risk with the incidence of preeclampsia in primigravida mothers at BLUD RS. HM Djafar Harun and BLUD Benyamin Guluh Hospital in Kolaka Regency. Variables that are significantly at risk with preeclampsia incidence in primigravida mothers based on multivariate analysis are the hypertension history variable with OR value: 3.363 with a CI value of 2.126 and an upper value of 5.318.
Conflict of interestThe authors declare no conflict of interest.
Peer-review under responsibility of the scientific committee of the 3rd International Nursing, Health Science Students & Health Care Professionals Conference. Full-text and the content of it is under responsibility of authors of the article.











