



To describe the association between consumption of different alcoholic beverages and adherence to the Mediterranean diet.
MethodsA cross-sectional analysis was conducted of the baseline data of the DiSA-UMH study, an ongoing cohort study with Spanish health science students (n=1098) aged 17-35 years. Dietary information was collected by a validated 84-item food frequency questionnaire. Participants were grouped into non-drinkers, exclusive beer and/or wine drinkers and drinkers of all types of alcoholic beverages. Mediterranean diet adherence was determined by using a modification of the relative Mediterranean Diet Score (rMED; score range: 0-16) according to consumption of 8 dietary components. We performed multiple linear and multinomial regression analyses.
ResultsThe mean alcohol consumption was 4.3g/day (SD: 6.1). A total of 19.5%, 18.9% and 61.6% of the participants were non-drinkers, exclusive beer and/or wine drinkers and drinkers of all types of alcoholic beverages, respectively. Participants who consumed beer and/or wine exclusively had higher rMED scores than non-drinkers (β: 0.76, 95%CI: 0.25-1.27). Drinkers of all types of alcoholic beverages had similar rMED scores to non-drinkers. Non-drinkers consumed less fish and more meat, whereas drinkers of all types of alcoholic beverages consumed fewer fruits, vegetables and more meat than exclusive beer and/or wine drinkers.
ConclusionsThe overall alcohol consumption among the students in our study was low-to-moderate. Exclusive beer and/or wine drinkers differed regarding the Mediterranean diet pattern from non-drinkers and drinkers of all types of alcohol. These results show the need to properly adjust for diet in studies of the effects of alcohol consumption.
Explorar la asociación entre el consumo de diferentes bebidas alcohólicas y la adherencia a la dieta Mediterránea.
MétodosSe analizaron transversalmente los datos basales del estudio DiSA-UMH (n=1098) de 17-35 años. Para recoger información dietética se utilizó un cuestionario de frecuencia de alimentos de 84 ítems validado previamente. Se agrupó a los participantes en no bebedores, bebedores exclusivos de cerveza o vino (o ambos), y bebedores de todo tipo de bebidas. La adherencia a la dieta mediterránea se determinó usando una modificación de la relative Mediterranean Diet Score (rMED). Se utilizó regresión lineal múltiple y multinomial.
ResultadosLa media de alcohol fue de 4,3 (6,1) g/día. El 19,5%, el 18,9% y el 61,6% de los participantes fueron clasificados en no bebedores, bebedores exclusivos de cerveza o vino, y bebedores de todo tipo de bebida, respectivamente. Los participantes clasificados en bebedores exclusivos de cerveza o vino tuvieron una mayor rMED que los no bebedores (β: 0,76; intervalo de confianza del 95%: 0,25-1,27). Los participantes clasificados en bebedores de todo tipo de bebidas tuvieron una rMED similar a los no bebedores. En comparación con los bebedores exclusivos de cerveza o vino, los no bebedores consumían menos pescado y más carne, mientras que los bebedores de todo tipo consumían menos frutas, vegetales y más carne.
ConclusionesLa ingesta de alcohol entre los estudiantes de nuestro estudio fue en general baja-moderada. Los bebedores exclusivos de cerveza o vino presentaron un patrón dietético mediterráneo diferenciado del de los no bebedores y los bebedores de todo tipo de bebidas, lo que justificaría ajustar correctamente por la dieta en estudios sobre los efectos del consumo de alcohol.
Alcohol consumption is a serious worldwide public health problem because of its high prevalence and the substantial physical and psychosocial health burden caused by its harmful use.1 Alcohol drinking is a risk factor associated to more than 200 pathologies.1 In many cases exists a dose-response relationship, especially for the alcohol attributable cancers.2 For example, it has been demonstrated that yet one alcoholic drink per day increases the risk for female breast cáncer.3 Young people are a vulnerable collective and the negative effects of alcohol consumption may be more pronounced among them.4 Consequences include an elevated risk of other drug abuse, suffering car accidents as a result of driving under the influence of alcohol and higher long term risks of developing chronic alcohol consumption or alcohol addiction.4 Additionally, alcohol consumption at younger ages interferes with the complex process of brain development.5 Some U.S. studies have shown higher rates of alcohol abuse and alcoholism in university students than in non-students.6 Interestingly, despite their training in health issues, medical students also show alarming rates of alcohol intake although recent studies in health science students are scarce.7
In contrast, the benefits of moderate alcohol consumption have been demonstrated in relation to cardiovascular diseases.8 However, the balance between potential harms and benefits of moderate alcohol consumption is a complex matter and internationally consistent recommendations still do not exist.9 The Mediterranean diet includes daily moderate alcohol consumption, especially of red wine.10 This dietary pattern plays an important role in the reduction of cardiovascular risk which was recently confirmed by a large randomized intervention trial.11 An important question in this aspect is whether the beneficial effects of moderate alcohol consumption are caused by the alcohol itself, by non-alcoholic drink components or by associated dietary or lifestyle factors. Many studies observed that the preferences for certain alcoholic beverages, which is usually defined as more than 50% of the total alcohol intake coming from a particular beverage, are associated with certain dietary or lifestyle habits.12,13 For example, it has been reported that wine consumption is associated with healthier dietary and lifestyle habits.13–15 This observation could partially explain the described health benefits of moderate alcohol or red wine consumption or it may even introduce confounding.14–16 On the other hand, a prospective Spanish study did not identify relevant differences between alcoholic beverage preference and the adherence to the Mediterranean dietary pattern and concluded that the positive cardiovascular effects should not be attributed to an overall healthier dietary pattern.17 Hence, more research is needed to explore the association between the intake of specific alcoholic beverages and specific dietary patterns.
In the present study, we aimed to describe the alcohol consumption among university health science students using the baseline data of a Spanish prospective epidemiological cohort (DiSA-UMH Project) and to explore the association between the consumption of alcoholic beverages and Mediterranean Diet adherence.
MethodsStudy populationThe DiSA-UMH Project (Dieta, Salud y Antropometría - Universidad Miguel Hernandez) is a prospective cohort study of health science university students from the Miguel Hernandez University in Alicante, Spain. Baseline information was collected for 1204 subjects (868 female and 336 male) aged 17 to 35 years during the enrolment period from 2006 to 2012. The study rationale and design has been previously described in detail.18,19 Briefly, the recruitment took place during the lecture period from different health science degrees at the San Joan d’Alacant Campus of Miguel Hernández University such as Medicine (72%), Physiotherapy (10%), Master of Public Health program (9%), Occupational Therapy (5%) and Pharmacy (4%). After we excluded the subjects with missing data for relevant variables and extreme values for mean daily energy intake (<500 and >3500kcal/day for women, <800 and >4000kcal/day for men) which indicate misreporting,20 1098 students (91.2%) between 17 and 35 years (791 female and 307 male) were included in the present analysis. All subjects gave informed consent and responded to a self-administered questionnaire at baseline. The study was approved by the ethics committee of the Miguel Hernandez University.
Dietary assessmentThe alcohol consumption and dietary intake were evaluated using a self-administered semi-quantitative food-frequency-questionnaire (FFQ) completed at baseline. The FFQ was an adapted version of the questionnaire by Willett et al.21 and validated for Spanish populations.22,23 Nutrient values for each food in the questionnaire were mainly obtained from the food composition tables of the US Department of Agriculture and other Spanish sources.24,25
Assessment of alcohol intakeThe FFQ included the following types of alcoholic drinks in order to measure total alcohol intake: red wine (one drink=125ml), other wines (one drink=125ml), beer (one drink=200ml), medium alcoholic drinks such as sherry, dry wines or vermouth (one drink=50ml) and spirits such as brandy, gin, rum, whisky or vodka (one drink=50ml). The validity and reproducibility of the FFQ used in the present study was satisfactory when comparing the FFQ with 3 to 9 repeated 24-hours recall. The correlation coefficients for the 1-year reproducibility and validity of mean alcohol intake in grams per day were 0.78 and 0.58, respectively. Subjects were categorized into 3 groups by alcohol consumption: non-drinkers (alcohol intake=0g/day), exclusive beer and/or wine drinkers (only beer, only wine or only beer and wine consumption) and drinkers of all types of alcoholic beverages (only high graduation drinks or only medium graduation drinks or drinks of various categories). For an additional analysis, we categorized the subjects according to their alcoholic beverage preference which we defined as >50% of the total alcohol intake coming from the specific beverages, as done in other epidemiological studies.14,17 The alcohol intake was categorized according to the criteria of the relative Mediterranean Diet score (rMED)26 after excluding the non-drinkers: low (<5g/day for women, <10g/day for men), moderate (5-25g/day for women, 10-50g/day for men) and high (>25g/day for women, >50g/day for men).
Mediterranean Diet assessmentThe Mediterranean Diet adherence was determined by the rMED score26 which was adapted by excluding the item alcohol as it was considered as the independent variable (consumed drink type). The rMED is based on the ingestion of typical components of the Mediterranean Diet. In order to calculate the score, the intake of eight components was expressed in grams per 1000kcal/day to express them in terms of energy density. Afterwards, tertiles were calculated and assigned with 0, 1 or 2 points. Out of the 8 items of the rMED, six are considered to be healthy and therefore positively scored: fruits (including nuts), vegetables (not including potatoes), legumes, cereals (including whole grain), fresh fish and olive oil. Two components were negatively scored (2 points for less consumption): total meat consumption (including processed meat) and dairy products. To obtain the score of each participant we added the points of each component. Hence, the possible score range was from 0 points (minimum adherence) to 16 points (maximum adherence). Furthermore, we calculated the tertiles of the score to determine the relative adherence of the subjects: first, 0-7 (42.8%); second, 8-9 (27.9%); and third, 10-16 (29.3%).
CovariatesThe following information was also collected at baseline: age in years, sex (male, female), smoking status (smoker, non-smoker), physical activity (no, low, moderate, medium and high activity) and television viewing in hours per day (≤1hour, >1-2hour and >2hours).27 The body mass index (BMI) was calculated by dividing the self-reported weight in kilograms by the squared self-reported height in meters. The self-reported weight and height were validated by comparing them to direct weight and height measurements in a subgroup of the study (n=628): the Pearson correlation coefficients were 0.97 for the weight, 0.96 for the height and 0.95 for the BMI.28
Statistical analysisThe statistical analysis was conducted with the statistical software R, version 3.0.2. The applied statistical tests were bilateral and signification was established at 0.05.
To compare the sample characteristics between each group we applied analysis of variance (ANOVA) for continuous variables and Chi-squared tests for categorical variables. The association between Mediterranean Diet adherence and the type of alcoholic beverage consumed was analyzed by multiple lineal regression to explore the continuous relation. Furthermore, a multinomial regression model was computed to explore the association between the tertiles of the rMED score and the type of alcoholic beverage consumed, considering the non-drinkers as the reference category. Relative risk ratios (RRR) were calculated for each rMED tertile for exclusive beer and/or wine drinkers and for drinkers of all types of alcoholic beverages in order to compare their Mediterranean Diet adherence to that of the non-drinkers. Moreover, a multinomial regression model was used to study the association between each component of the rMED score and drinkers of all types of alcoholic beverages as well as non-drinkers compared to exclusive beer and/or wine drinkers.
Models were adjusted for potential confounders based on those factors published in literature and those variables with p values <0.20 in the bivariate analysis. When adjusting for not living with the family the results did not appreciably change in the association and therefore this variable was not included in the final models. Finally, all models were adjusted for sex, age, BMI, hours of TV viewing per day, smoking status, soft drink intake and total energy intake (kcals).
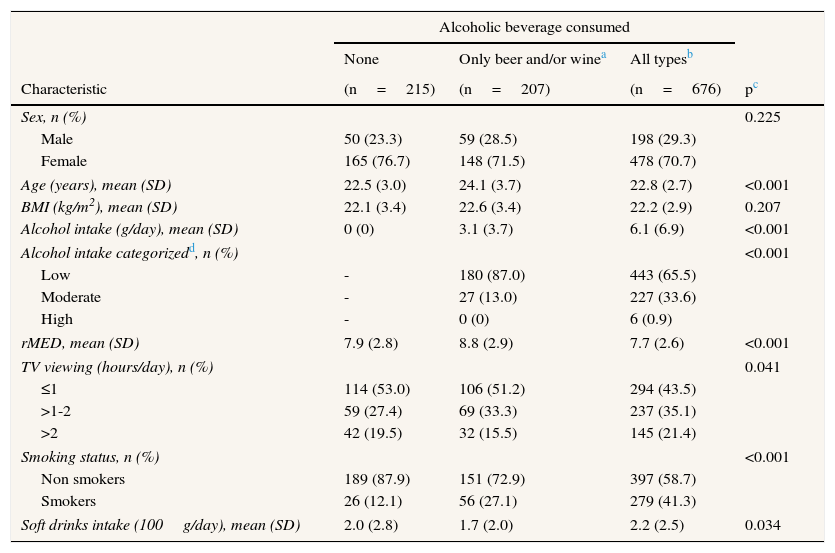
ResultsTable 1 shows the characteristics of the study population according to the type of alcoholic beverage consumed. Of the total number of subjects (n=1098), 19.6% were non-drinkers and 80.4% drinkers (18.9% consumed exclusively beer and/or wine and 61.6% consumed other alcoholic drinks as middle or high graduation drinks or combinations). Of the exclusive beer and/or wine drinkers, 51.7% consumed only beer, 16.9% only wine and 34.3% both. The mean overall alcohol consumption was 4.3g/day (SD: 6.1). When categorized by the rMED score criteria, 87.0% of the exclusive beer and/or wine drinkers had a low daily alcohol intake and 13.0% a moderate daily alcohol intake. Of the drinkers of other alcoholic drinks or combinations 65.5% had a low daily alcohol intake, 33.6% a moderate and 0.9% a high daily alcohol intake.
Characteristics of the subjects of the DiSA-UMH study (n=1098) according to the type of alcoholic beverage consumed.
| Alcoholic beverage consumed | ||||
|---|---|---|---|---|
| None | Only beer and/or winea | All typesb | ||
| Characteristic | (n=215) | (n=207) | (n=676) | pc |
| Sex, n (%) | 0.225 | |||
| Male | 50 (23.3) | 59 (28.5) | 198 (29.3) | |
| Female | 165 (76.7) | 148 (71.5) | 478 (70.7) | |
| Age (years), mean (SD) | 22.5 (3.0) | 24.1 (3.7) | 22.8 (2.7) | <0.001 |
| BMI (kg/m2), mean (SD) | 22.1 (3.4) | 22.6 (3.4) | 22.2 (2.9) | 0.207 |
| Alcohol intake (g/day), mean (SD) | 0 (0) | 3.1 (3.7) | 6.1 (6.9) | <0.001 |
| Alcohol intake categorizedd, n (%) | <0.001 | |||
| Low | - | 180 (87.0) | 443 (65.5) | |
| Moderate | - | 27 (13.0) | 227 (33.6) | |
| High | - | 0 (0) | 6 (0.9) | |
| rMED, mean (SD) | 7.9 (2.8) | 8.8 (2.9) | 7.7 (2.6) | <0.001 |
| TV viewing (hours/day), n (%) | 0.041 | |||
| ≤1 | 114 (53.0) | 106 (51.2) | 294 (43.5) | |
| >1-2 | 59 (27.4) | 69 (33.3) | 237 (35.1) | |
| >2 | 42 (19.5) | 32 (15.5) | 145 (21.4) | |
| Smoking status, n (%) | <0.001 | |||
| Non smokers | 189 (87.9) | 151 (72.9) | 397 (58.7) | |
| Smokers | 26 (12.1) | 56 (27.1) | 279 (41.3) | |
| Soft drinks intake (100g/day), mean (SD) | 2.0 (2.8) | 1.7 (2.0) | 2.2 (2.5) | 0.034 |
BMI, body mass index; rMED: relative Mediterranean Diet score; SD: standard deviation.
Includes all subjects who consumed only beer, only wine (including red and other wines) or only beer and wine.
Includes all subjects who consumed drinks of various categories or only medium graduation drinks or only high graduation drinks.
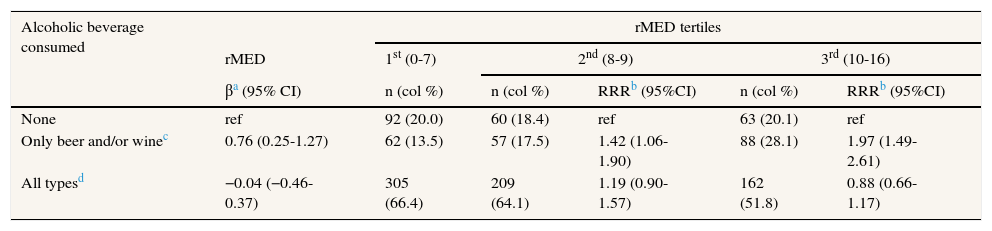
The mean rMED score for exclusive beer and/or wine drinkers was about one unit higher than the observed for non-drinkers and drinkers of all types of alcoholic beverages (8.8 vs. 7.9 and 7.7 respectively). Table 2 shows the association between the type of alcoholic beverage consumed and Mediterranean Diet adherence adjusting for sex, age, BMI, hours of TV viewing per day, smoking status, soft drink intake and total energy intake. In the lineal regression analysis, subjects who consumed exclusively beer and/or wine had a significantly higher Mediterranean Diet adherence than non-drinkers, β for 1 rMED score=0.76 (95%CI: 0.25-1.27). No association was observed for subjects who consumed all types of alcoholic beverages. In the multinomial logistic regression model, subjects who consumed exclusively beer and/or wine showed statistically significant higher Mediterranean Diet adherence than non-drinkers: RRR=1.42 (95%CI: 1.06-1.90) and RRR=1.97 (95%CI: 1.49-2.61) for the second and third tertiles of rMED, respectively. No association was observed for subjects who consumed all types of alcoholic beverages.
Association between Mediterranean Diet adherence measured by the rMED score and type of alcoholic beverage consumed in subjects of the DiSA-UMH study (n=1098).
| Alcoholic beverage consumed | rMED tertiles | |||||
|---|---|---|---|---|---|---|
| rMED | 1st (0-7) | 2nd (8-9) | 3rd (10-16) | |||
| βa (95% CI) | n (col %) | n (col %) | RRRb (95%CI) | n (col %) | RRRb (95%CI) | |
| None | ref | 92 (20.0) | 60 (18.4) | ref | 63 (20.1) | ref |
| Only beer and/or winec | 0.76 (0.25-1.27) | 62 (13.5) | 57 (17.5) | 1.42 (1.06-1.90) | 88 (28.1) | 1.97 (1.49-2.61) |
| All typesd | −0.04 (−0.46-0.37) | 305 (66.4) | 209 (64.1) | 1.19 (0.90-1.57) | 162 (51.8) | 0.88 (0.66-1.17) |
95%CI, 95% confidence interval; col: column; ref: reference; rMED: modified relative Mediterranean Diet score; RRR: relative risk ratio.
β regression coefficient; obtained from a lineal regression model adjusted for sex, age, BMI, hours of TV viewing per day, smoking status, soft drink intake and total energy intake.
RRR obtained from multinomial logistic regression models comparing the categories only beer and/or wine and all types to none; adjusted for sex, age, BMI, hours of TV viewing per day, smoking status, soft drink intake and total energy intake.
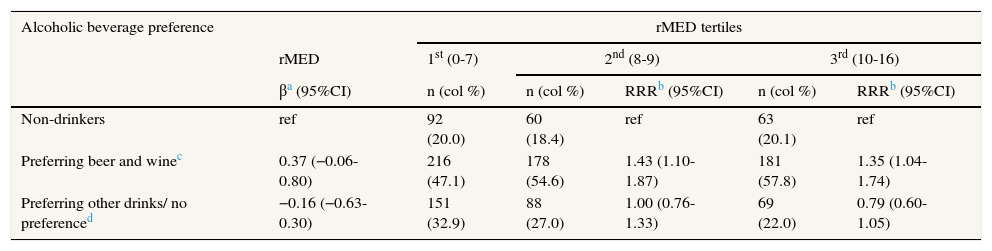
When the analyses were based on alcoholic beverage preference (defined as >50% of total alcohol ingestion coming from the specific beverages) instead of exclusive beverage consumption (all alcohol ingested coming from the specific beverages) the association between Mediterranean diet adherence and beer and/or wine preference diminished (see Table 3). In the multinomial logistic regression analysis the association remained statistically significant: RRR=1.43 (95%CI: 1.10-1.87) and RRR=1.35 (95%CI: 1.04-1.74) for the second and third tertiles of rMED, respectively, but no association was observed for subjects who consumed all types of alcoholic beverages. In contrast, in the linear regression analysis no statistically significant associations were observed.
Association between Mediterranean Diet adherence measured by the rMED score and preferred alcoholic beverage in subjects of the DiSA-UMH study (n=1098).
| Alcoholic beverage preference | rMED tertiles | |||||
|---|---|---|---|---|---|---|
| rMED | 1st (0-7) | 2nd (8-9) | 3rd (10-16) | |||
| βa (95%CI) | n (col %) | n (col %) | RRRb (95%CI) | n (col %) | RRRb (95%CI) | |
| Non-drinkers | ref | 92 (20.0) | 60 (18.4) | ref | 63 (20.1) | ref |
| Preferring beer and winec | 0.37 (−0.06-0.80) | 216 (47.1) | 178 (54.6) | 1.43 (1.10-1.87) | 181 (57.8) | 1.35 (1.04-1.74) |
| Preferring other drinks/ no preferenced | −0.16 (−0.63-0.30) | 151 (32.9) | 88 (27.0) | 1.00 (0.76-1.33) | 69 (22.0) | 0.79 (0.60-1.05) |
95%CI: 95% confidence interval; col: column; ref: reference; rMED: modified relative Mediterranean Diet score; RRR: relative risk ratio.
β regression coefficient; obtained from a lineal regression model adjusted for sex, age, BMI, hours of TV viewing per day, smoking status, soft drink intake and total energy intake.
RRR obtained from multinomial logistic regression models comparing the categories preferring beer and wine and preferring other drinks/no preference to non-drinkers; adjusted for sex, age, BMI, hours of TV viewing per day, smoking status, soft drink intake and total energy intake.
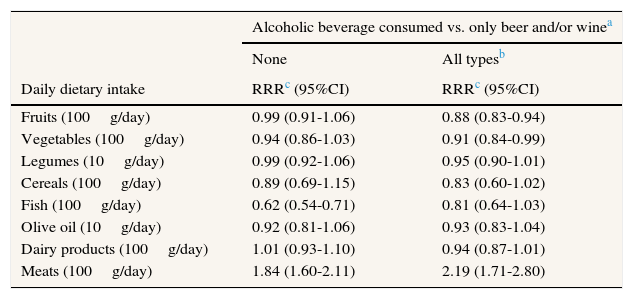
Table 4 shows the results of the multinomial logistic regression analysis according to components of the rMED by comparing exclusive beer and/or wine drinkers to non-drinkers and drinkers of all types of alcoholic beverages.
Association between the intake of Mediterranean Diet components and exclusive beer and/or wine consumption in comparison with no alcohol consumption and the consumption of all types of alcoholic beverages in subjects of the DiSA-UMH study (n=1098).
| Alcoholic beverage consumed vs. only beer and/or winea | ||
|---|---|---|
| None | All typesb | |
| Daily dietary intake | RRRc (95%CI) | RRRc (95%CI) |
| Fruits (100g/day) | 0.99 (0.91-1.06) | 0.88 (0.83-0.94) |
| Vegetables (100g/day) | 0.94 (0.86-1.03) | 0.91 (0.84-0.99) |
| Legumes (10g/day) | 0.99 (0.92-1.06) | 0.95 (0.90-1.01) |
| Cereals (100g/day) | 0.89 (0.69-1.15) | 0.83 (0.60-1.02) |
| Fish (100g/day) | 0.62 (0.54-0.71) | 0.81 (0.64-1.03) |
| Olive oil (10g/day) | 0.92 (0.81-1.06) | 0.93 (0.83-1.04) |
| Dairy products (100g/day) | 1.01 (0.93-1.10) | 0.94 (0.87-1.01) |
| Meats (100g/day) | 1.84 (1.60-2.11) | 2.19 (1.71-2.80) |
95%CI: 95% confidence interval; RRR: relative risk ratio.
Compared with exclusive beer and/or wine drinkers, non-drinkers had a significantly lower daily fish intake (RRR for 100g/day=0.62; 95%CI: 0,54-0.71) and a significantly higher daily meat intake (RRR for 100g/day=1.84; 95%CI: 1.60-2.11). The drinkers of all types of alcoholic beverages showed a significantly lower daily intake of fruits (RRR for 100g/day=0.88; 95%CI: 0.83-0.94) and vegetables (RRR for 100g/day=0.91; 95%CI: 0.84-0.99) as well as a higher daily meat intake (RRR for 100g/day=2.19; 95%CI: 1.71-2.80) in comparison with exclusive beer and/or wine drinkers.
DiscussionThe overall alcohol consumption in this population of university health science students in Spain was low to moderate. Furthermore, our findings suggest that those university students who consumed exclusively beer and/or wine had a higher Mediterranean Diet adherence than non-drinkers and drinkers of all alcoholic beverages.
The mean daily alcohol intake in the present study (4.3g/day) was much lower than the mean alcohol intake for the same age range observed in the Spanish national health survey carried out in 2011-12 (11.8g/day).29 The high alcohol consumption of students/medical students that some studies have reported7,30–32 has not been confirmed in this collective of Spanish health science students.
The higher adherence to Mediterranean Diet observed among those students who exclusively consumed or preferred beer and/or wine in our study are comparable to the results of one study from the U.S. where subjects who preferred wine reported eating more fruits and vegetables and fewer servings of red or fried meats.14 These associations are important because it is possible that the diet quality may contribute to the described beneficial effects of low to moderate alcohol consumption.14 However, a Spanish study with 10,526 university graduates did not observe differences in the adherence to the Mediterranean food pattern according to alcoholic beverage preference.17 Nevertheless, we must be cautious in comparing results from different studies based on beverage preferences because determining beverage preference instead of exclusive beverage consumption could explain the identification of fewer differences between the different study groups. As alcoholic beverage preference in many studies is defined as at least 50% of the total alcohol ingestion coming from a specific alcoholic beverage, theoretically an important amount (up to 50%) could come from another specific alcoholic beverage which leads to overlapping alcoholic ingestion patterns between the different study groups. Consequently, when analysing beverage preference instead of exclusive beverage consumption, weaker and non-statistically significant associations may be observed. This observation highlights a limitation of the use of less specific definitions of beverage preference to determine the alcohol consumption pattern and could in part explain some inconsistencies in published results.
Interestingly, the higher mean rMED score among exclusive beer and/or wine drinkers with respect to the non-drinkers and drinkers of all types of alcoholic beverages had a different basis. Non-drinkers reported a lower fish and a higher meat intake, whereas drinkers of all types of alcoholic beverages had a lower intake of fruits and vegetables as well as a higher intake of meat. These findings are consistent with the described associations between both higher alcohol intake and lower diet quality33 and low to moderate wine consumption and higher diet quality13,14. To explore possible differences regarding the Mediterranean diet adherence between wine and beer drinkers, we excluded the drinkers of only wine or combinations of beer and wine from the analysis but the results remained very similar, which suggested that beer and wine drinkers may have similar patterns of Mediterranean diet adherence (data not shown).
This study may have some limitations. First, the cross-sectional analysis of the baseline data does not allow causal inferences. Therefore, it is not possible to separate the relationship between exclusive beer and/or wine consumption from higher Mediterranean Diet adherence. Moreover, we did not address the maximum alcohol intake on a single occasion or whether the alcohol was consumed with meals, as this is typical for the Mediterranean Diet. These are relevant limitations as a recent study pointed out the importance of the specific Mediterranean alcohol-drinking pattern because it was associated with a relative risk reduction in mortality.34 Additionally, we could not determine binge drinking in the present study because the maximum alcohol intake on a single occasion was not measured by the questionnaire. Binge drinking is a highly relevant and current health issue in relation with alcohol drinking, especially in young people.35 It should be taken into account in future studies on the association between dietary and drinking habits. Furthermore, the fact that the subjects were health science students who voluntarily participated in the study might have caused some response bias. In order to minimize bias, we used a validated food frequency questionnaire22 and carried out the validation of self-reported weight and height in a subgroup of the study population.28
The results of our study confirm the importance to adjust for dietary habits or patterns when studies on the effect of low to moderate beer and/or wine consumption are performed. Not adjusting for these factors could lead to confounding and an overestimation of benefits from low to moderate alcohol consumption might result. However, our findings should be confirmed in studies with other samples as well as less selected populations than health science students. The long term goal should be to describe and understand the complex interplay between eating and drinking habits considering also the specific social, educational and environmental backgrounds and to use this information for the planning of effective and specific health promotion strategies.
ConclusionsIn a population of health science students with a low to moderate overall alcohol consumption, exclusive beer and/or wine consumption was associated with a higher Mediterranean Diet adherence than non-drinking and drinking all types of alcoholic beverages. The stricter determination of exclusive beverage consumption instead of the less specific determination of beverage preferences led to different results which could explain some inconsistencies in published literature. Moreover, the results of our study confirm the importance to adjust for dietary habits or patterns when studies on the effect of alcohol consumption are performed. These findings should be considered in further studies on alcohol drinking and dietary patterns.
Editor in chargeAlberto Ruano-Ravina.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Ethical standards disclosureThis study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the ethics committee of the Miguel Hernandez University. Written informed consent was obtained from all subjects.
Alcohol consumption at younger ages interferes with the complex process of brain development. Prevalence of alcohol consumption in students is high. The preferences of certain alcoholic beverages are associated with certain dietary or lifestyle habits.
What does this study add to the literature?Our health science students have a low to moderate overall alcohol consumption. The stricter determination of exclusive beverage consumption instead of the less specific determination of beverage preferences led to different results. The exclusive beer and/or wine drinkers showed a different Mediterranean diet pattern from non-alcohol and all types of alcohol drinkers, which could warrant adjusting for diet in studies on the effects of alcohol consumption.
J. Vioque, M. García de la Hera and E.M. Navarrete-Muñoz designed and concept the study. D. Gimenez-Monzo, D. Valera-Gran, S. Gonzalez-Palacios and L. Torres-Collado collected the data. A. Scholz and E.M. Navarrete-Muñoz performed the analysis of the data. A. Scholz drafted the manuscript. All authors contributed to the interpretation of the result, critically revised the work and approved the final version to be published.
FundingThe DiSA-UMH study has received funding from the Consellería de Sanitat-Generalitat Valenciana (grant number CTGCA/2002/06, G03/136, ACOMP/2010/115, 087/2008, 084/2010); CIBER de Epidemiología y Salud Pública; A.S. is supported by an “Ayuda de iniciación a la investigación” scholarship from the Miguel Hernandez University; D.G.M. is supported by a Vali+d fellowship from the Generalitat Valenciana; S.G.P. is supported by a PFIS fellowship from the Spanish Government and L.T. is supported by a Geronimo Forteza fellowship from the Generalitat Valenciana. Funding sources had no role in the design, analysis or writing of this article.
Conflicts of interestNone.
The authors thank the subjects of the DiSA-UMH cohort for their enthusiastic participation and collaboration. We also thank the other members of the DiSA-UMH study who participate in the collection of information: Sergio Hernández-Sánchez, José Vicente Toledo-Maruhenda, José Francisco Checa-Sevilla, Fernando Cano, María Martinez-Moya, Fatoumata Rosita Savane, Ricardo Barrios, Laura Compañ and Amaia Beti. Jonathan Whitehead provided assistance with the English revision of the manuscript.











