



Sleep quality has a significant impact on health and quality of life and is affected, among other factors, by age and sex. However, the prevalence of problems in this area in the general population is not well known. Therefore, our objective was to study the prevalence and main characteristics of sleep quality in an adult population sample.
Methods2,144 subjects aged between 43 and 71 years belonging to the Murcia (Spain) Twin Registry. Sleep quality was measured by self-report through the Pittsburgh Sleep Quality Index (PSQI). Logistic regression models were used to analyse the results.
ResultsThe prevalence of poor sleep quality stands at 38.2%. Univariate logistic regression analyses showed that women were almost twice as likely as men (OR: 1.88; 95% confidence interval [95%CI]: 1.54 to 2.28) to have poor quality of sleep. Age was directly and significantly associated with a low quality of sleep (OR: 1.05; 95%CI: 1.03 to 1.06).
ConclusionsThe prevalence of poor sleep quality is high among adults, especially women. There is a direct relationship between age and deterioration in the quality of sleep. This relationship also appears to be more consistent in women.
La calidad del sueño tiene una incidencia notable en la salud y en la calidad de vida, y a su vez se ve afectada, entre otros factores, por la edad y el sexo. Sin embargo, la prevalencia de problemas en este ámbito en la población general no es bien conocida. Por ello, nuestro objetivo fue estudiar la prevalencia y las características de la calidad del sueño en una muestra de población adulta.
Métodos2144 personas de edades comprendidas entre 43 y 71 años pertenecientes al Registro de Gemelos de Murcia. La calidad del sueño se determinó por autoinforme mediante el índice de calidad del sueño de Pittsburgh. Se utilizaron modelos de regresión logística para el análisis de los resultados.
ResultadosLa prevalencia de una pobre calidad del sueño se sitúa en el 38,2%. Los análisis de regresión logística univariados mostraron que las mujeres prácticamente doblaban (odds ratio [OR]: 1,88; intervalo de confianza del 95% [IC95%]: 1,54-2,28) la probabilidad de tener una pobre calidad del sueño con respecto a los hombres. La edad se asocia de manera directa y significativa con una baja calidad del sueño (OR: 1,05; IC95%: 1,03-1,06).
ConclusionesLa prevalencia de una pobre calidad del sueño es alta en la población adulta, en especial en las mujeres. Existe una relación directa entre la edad y el deterioro de la calidad del sueño. Esta relación también parece ser más consistente en las mujeres.
Sleep quality is directly related to the overall health and quality of life. Sleep-related problems are associated with poorer health, increased risk of mortality, hormonal and biochemical changes, higher health care costs, increased use of health resources, absenteeism and increased risk of psychological disorders, especially depression.1–4
Note that the term “sleep quality” entails certain difficulties in definition and in differentiation from insomnia. The term covers a number of aspects such as latency and total sleep time, number of awakenings and sleep efficiency, among others.5
The relationship between sleep quality and mental health is well established, but it is usually analyzed from a negative perspective. In fact, sleep problems are part of the expected symptoms in mood disorder.6 Thus, the prevalence of poor sleep quality in patients suffering from anxiety or depression is much higher compared to the overall population.6 This is a two-way relationship and it has been demonstrated by longitudinal studies and meta-analysis, finding that it is twice as likely to develop a depressive disorder if suffering from insomnia.7 Some authors have also found a strong relationship between sleep duration and severity of symptoms associated with bipolar disorder.8 In general, the quality of sleep decreases when the number of comorbidities increased. Using the Pittsburgh scale, it has been estimated that for every comorbidity, the score increased 0.37 on this scale.9
Prevalence of problems related to sleep qualityThe prevalence of poor sleep quality and sleep problems varies greatly depending on the population. For example, in a study in 8 different countries, the prevalence of poor sleep quality ranged from 3.9% to over 40%.10 In a study of Norwegians using DSM-V, a prevalence of 7.1% (8.6% for women, 5.5% for men)11 was found. Higher prevalence has been reported in Canadians (13.4%).12 Given this variability, the accuracy, the precision, and the criteria used to define sleep problems are fundamental.
The reported prevalence of insomnia in Spain varies depending on the used methodology. For example, the type of questions is responsible for variations between 11.3% and 22.9%.13,14 Other data show insomnia according to DSM-IV at 6.4%, and complaints related with insomnia at 20.8%, with higher incidence in women (23.9%) than men (17.6%).15 Finally, as expected, in a clinical population, the prevalence of poor sleep quality is higher, as was found in over 90% of anxious and depressive patients.6
Influence of sex on the prevalence of problems related to sleep qualityThe higher incidence of problems and shorter sleep duration in women is constant in the literature,11,16 and has been also found in the Spanish population.17 The National Health Survey 2011-2012 found an average sleep duration that ranged from 7.03 to 7.11hours in women between 45-74 years. In men, these same averages range from 7.19 to 7.61hours.18 In a meta-analysis of sex differences in prevalence of insomnia, Zhang and Wing16 found that women are 1.41 times more likely to suffer from insomnia.
These differences could be due to hormonal changes related to menopause symptoms and associated with physical, physiological and psychological changes that may increase the incidence of problems related to sleep.19 Insomnia increases in the perimenopausal state, and slightly decreases in the postmenopausal, but remains above the premenopausal levels. Moreover, insomnia contributes to psychopathology, mainly anxiety and depression, which increase during menopause and decrease later.20,21
Influence of age on the prevalence of problems related to sleep qualityAging contributes progressively to lower sleep quality in men and women.22,23 Throughout adulthood an attenuation of motivational pressure (tendency to fall asleep based on the elapsed wakefulness) is observed, leading to a lower recovery of lost sleep that affects its subjective quality. Similarly, after 40 years old people tend to go to bed earlier and wake up earlier.24
Due to the significant impact of the problems related to quality of sleep, and the influence of factors such as age and sex, it is particularly important to analyze what the actual prevalence of these problems in the population is, especially in the age groups where this impact is greater. There is also a lack of studies for Spain. Up to date data are needed in order to reveal the current situation accurately and establish the variations due to age and gender. Therefore, our objective is to study the prevalence of poor sleep quality and the characteristics of sleep quality components in a population based sample of adult subjects living in the Region of Murcia.
MethodsParticipantsThe sample comprised 2144 subjects born between 1939 and 1966, participants in the Murcia Twin Registry (MTR).25 The MTR is a population based registry of adult multiples in the Region of Murcia (Spain). The registry was born in 2006 based on an agreement between the University of Murcia and the Murcia Health Council. The general goal of this initiative was to constitute a basic research tool for the analysis of the relative contribution of genetic and environmental factors to the development of complex phenotypes, focusing on health and health-related behaviors. Participation in the MTR is voluntary, subjected to informed consent, and not remunerated. Information about the individuals comes from the databases available at the regional health system. People who were born on the same day and share their surnames are selected from these databases and contacted as potential twins. They are included in the MTR if they meet the inclusion criteria: pairs with both members alive at the time of incorporation, residence in the Region of Murcia, and no conditions or disability that may limit their voluntary participation. The MTR development strategy has followed a step-by-step process and data collection has been done in different sub-samples (female-female, male-male, opposite-sex pairs) and moments, and using alternative methods (face-to-face or telephone interview) depending on the availability of resources. Global cooperation rate across data collection waves and sub-samples is 72.5%. More detailed information about recruitment procedures and data collection is provided elsewhere.25,26 The MTR sample has been shown to be comparable regarding main health conditions to reference representative samples of the general population in the region and Spain, accounting for the generalizability of results.27
The MTR data collection and analytical procedures have been approved by the Committee of Research Ethics of the University of Murcia and meet the legal requirements of confidentiality and personal data protection. Since the objective of this work is not the analysis of the relative contribution of genetic and environmental factors on the studied phenotypes, it does not impact on the zygosity data of twins and no genetic analyses are carried out.
The study data were collected from the three sub-cohorts (female pairs, male and opposite-sex) providing data at different times between 2009 and 2011 through face-to-face or telephone interviews. Mean age of the subjects with available data for this study was 53.7 years (SD: 7.4; range: 43-71) at the time of data collection and 54.7% of the sample were women. Data collection and administration of the questionnaires was carried out at all times by trained personnel.
InstrumentsSubjects answered to an inventory developed specifically for the MTR that incorporates socio-demographic health-related information, together with several standard scales (e.g., zygosity questionnaire and Pittsburgh Sleep Quality Questionnaire). This inventory is based on the National Health Survey questionnaire,18 and questions are the same regardless of administration method. For this study we have selected from the demographic datasets (age and sex), menopausal status, and sleep quality information. Menopausal status was assessed through self-report on whether it had already begun or had passed, and in case of a hit, if it had started naturally or by other causes (disease/drug therapy/surgery) and the age of onset.
The subjective quality of sleep was assessed by a self-report questionnaire through the Pittsburgh Sleep Quality Index,28,29 which provides seven partial scores and an overall score on sleep characteristics referring to the previous month. The overall score is known as the Pittsburgh Sleep Quality Index in (PSQI). The questionnaire has proven reliable and valid30 and it is validated in its Spanish version.29 The seven partial scores are: 1) sleep quality, 2) sleep latency, 3) sleep duration, 4) habitual sleep efficiency (percentage of time that the patient believes to be asleep of the total time lying down), 5) sleep disturbance (frequency of disturbances such as snoring or toileting), 6) use of sleeping medication, and 7) daytime dysfunction (such as daytime sleepiness or fatigue). Subjects with a score >5 on a general scale can be classified as having poor sleep quality.28,29
Data analysisDependent variables were the overall score in the PSQI scores and the different subscales that compose it. The dependent variables were categorized in a binary fashion. The global PSQI Index was dichotomized as good (PSQI ≤5) or poor (PSQI >5) sleep quality according to the standard criteria for this scale.28,29 All subscales were also dichotomized. For quantitative scales the cut-off points were defined, according to the scoring system of the PSQI, depending on whether the score on the sub-scale added 0 or ≥1 points to the global index (1 or 2 points in the case of disturbances) (duration: ≥7hours vs. <7hours; disturbances: 0-9 vs. 10 or more; latency ≤15minutes vs. >15minutes; efficiency ≥85% vs. <85%). Discrete variables were categorized as yes/no or good/bad answers [daytime dysfunction (yes/no); subjective quality (good or fairly good/bad or very bad; use of sleeping medication (yes/no)].
To assess the association between age (quantitative) and gender with respect to PSQI and its various subscales logistic regression analyses were performed. Bivariate analyses were also performed to analyze the effect of age and sex together. The analysis of subjects from the same family produces dependence on data, which is why regression analyses were performed by adjusting the estimates of standard error. This method provides robust statistical estimates for the characteristics of the model. Analyses were performed using the statistical package STATA12. The level of statistical significance was set at α=0.05 with a confidence interval (CI) of 95%.
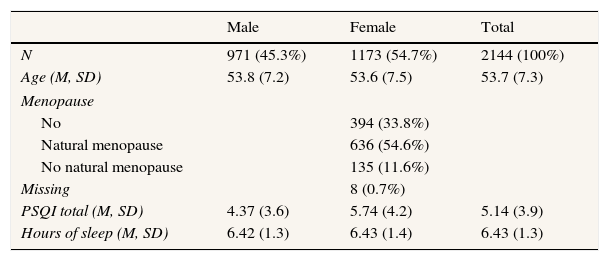
ResultsTables 1 and 2 summarize the main demographic characteristics of the sample and the results of the measures of sleep quality. The mean total sleep was 6.43hours (SD: 1.3). We found no differences in sex, with a similar average for men and women (6.42 and 6.43hours, respectively).
Sample characteristics and global measures of sleep quality.
| Male | Female | Total | |
|---|---|---|---|
| N | 971 (45.3%) | 1173 (54.7%) | 2144 (100%) |
| Age (M, SD) | 53.8 (7.2) | 53.6 (7.5) | 53.7 (7.3) |
| Menopause | |||
| No | 394 (33.8%) | ||
| Natural menopause | 636 (54.6%) | ||
| No natural menopause | 135 (11.6%) | ||
| Missing | 8 (0.7%) | ||
| PSQI total (M, SD) | 4.37 (3.6) | 5.74 (4.2) | 5.14 (3.9) |
| Hours of sleep (M, SD) | 6.42 (1.3) | 6.43 (1.4) | 6.43 (1.3) |
M: mean; PSQI: Pittsburgh Sleep Quality Index; SD: standard deviation.
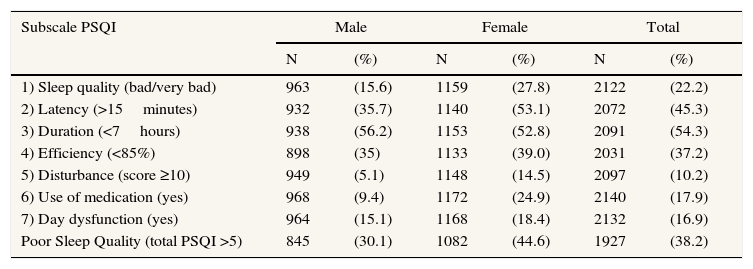
Proportion of subjects by gender with sleep quality problems. Subscales of PSQI.
| Subscale PSQI | Male | Female | Total | |||
|---|---|---|---|---|---|---|
| N | (%) | N | (%) | N | (%) | |
| 1) Sleep quality (bad/very bad) | 963 | (15.6) | 1159 | (27.8) | 2122 | (22.2) |
| 2) Latency (>15minutes) | 932 | (35.7) | 1140 | (53.1) | 2072 | (45.3) |
| 3) Duration (<7hours) | 938 | (56.2) | 1153 | (52.8) | 2091 | (54.3) |
| 4) Efficiency (<85%) | 898 | (35) | 1133 | (39.0) | 2031 | (37.2) |
| 5) Disturbance (score ≥10) | 949 | (5.1) | 1148 | (14.5) | 2097 | (10.2) |
| 6) Use of medication (yes) | 968 | (9.4) | 1172 | (24.9) | 2140 | (17.9) |
| 7) Day dysfunction (yes) | 964 | (15.1) | 1168 | (18.4) | 2132 | (16.9) |
| Poor Sleep Quality (total PSQI >5) | 845 | (30.1) | 1082 | (44.6) | 1927 | (38.2) |
PSQI: Pittsburgh Sleep Quality Index.
There are notable differences between men and women, with an overall average in the PSQI of 5.74 (SD: 4.2) for the first and 4.37 (SD: 3.6) for the second. On a dichotomized scale, poor quality of sleep occurs for 44.6% of women versus 30.1% of men. Overall, 38.2% of the sample had poor sleep quality. For the different subscales, the same differences are observed, obtaining scores that correspond to a poorer sleep quality in women (Table 2).
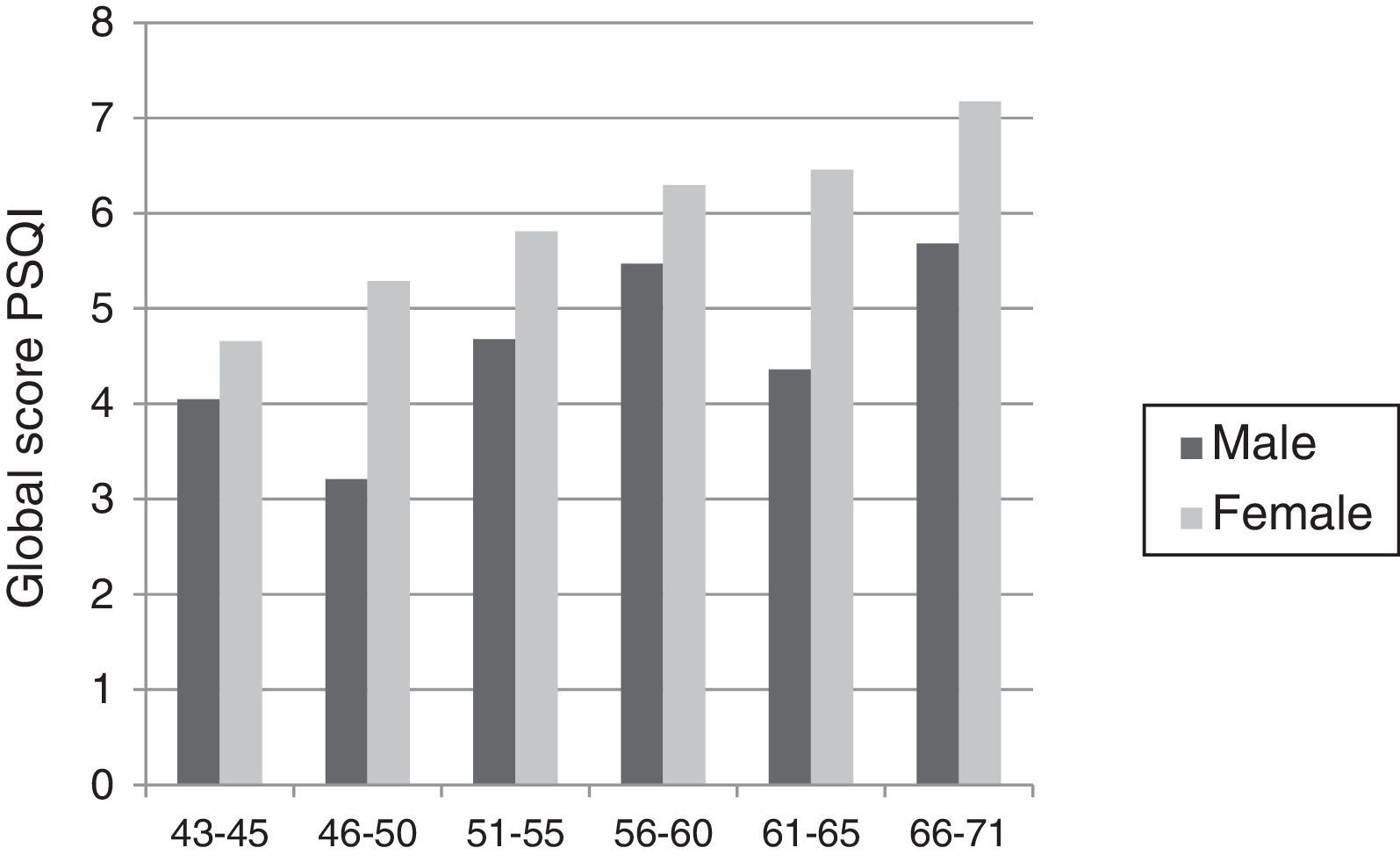
Age has an inverse relationship to the quality of sleep but varies by sex. While for women there is a steady worsening of sleep quality, in the case of men this deterioration is seen with a less stable and marked pattern (Fig. 1).

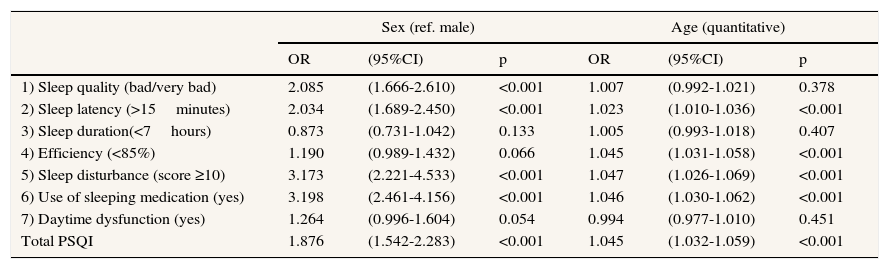
The univariate logistic analyses showed that both age and sex had a significant effect on the overall score of the PSQI. Women are significantly more likely to have poor sleep quality (OR: 1.88; 95%CI: 1.54 to 2.28) than men; age similarly affects significantly poor sleep quality (OR: 1.05; 95%CI: 1.03 to 1.06) (Table 3).
Logistic regression analyses. Influence of age and sex on sleep quality. Univariate results.
| Sex (ref. male) | Age (quantitative) | |||||
|---|---|---|---|---|---|---|
| OR | (95%CI) | p | OR | (95%CI) | p | |
| 1) Sleep quality (bad/very bad) | 2.085 | (1.666-2.610) | <0.001 | 1.007 | (0.992-1.021) | 0.378 |
| 2) Sleep latency (>15minutes) | 2.034 | (1.689-2.450) | <0.001 | 1.023 | (1.010-1.036) | <0.001 |
| 3) Sleep duration(<7hours) | 0.873 | (0.731-1.042) | 0.133 | 1.005 | (0.993-1.018) | 0.407 |
| 4) Efficiency (<85%) | 1.190 | (0.989-1.432) | 0.066 | 1.045 | (1.031-1.058) | <0.001 |
| 5) Sleep disturbance (score ≥10) | 3.173 | (2.221-4.533) | <0.001 | 1.047 | (1.026-1.069) | <0.001 |
| 6) Use of sleeping medication (yes) | 3.198 | (2.461-4.156) | <0.001 | 1.046 | (1.030-1.062) | <0.001 |
| 7) Daytime dysfunction (yes) | 1.264 | (0.996-1.604) | 0.054 | 0.994 | (0.977-1.010) | 0.451 |
| Total PSQI | 1.876 | (1.542-2.283) | <0.001 | 1.045 | (1.032-1.059) | <0.001 |
OR: odds ratio; 95%CI: confidence interval of 95%; PSQI: Pittsburgh Sleep Quality Index.
Regarding the components of the questionnaire, the influence of sex was significant in all subscales, except duration, daytime dysfunction and efficiency. Age significantly influenced all components except duration, daytime dysfunction, and sleep quality. None of the significant relationships lost significance in the bivariate analysis (age and sex) for all the variables, and the effect sizes remained of virtually the same magnitude.
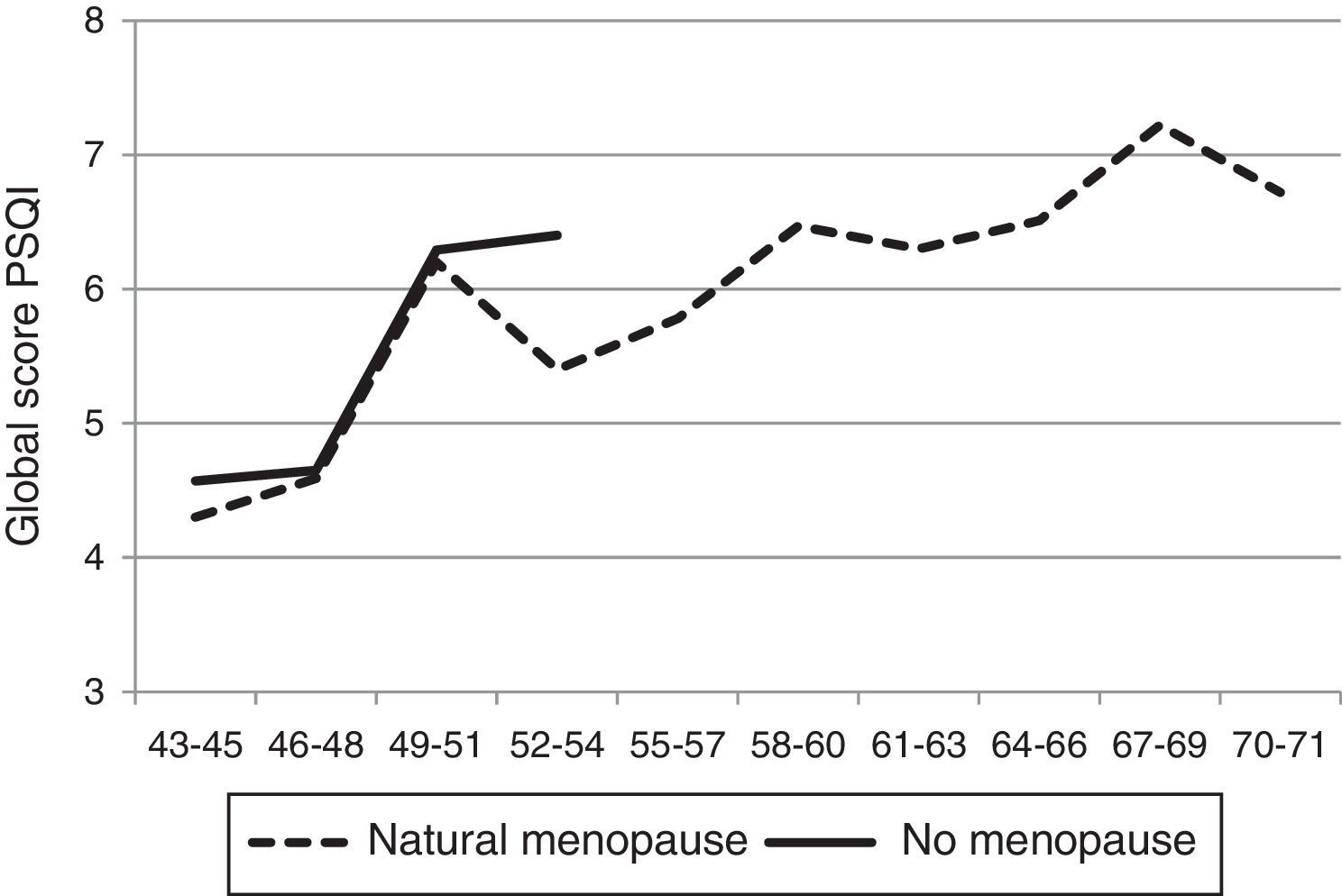
Given the possible relevance of menopausal status for the results, a comparative analysis was carried out among women who reported having begun or had had their menopause and the rest. Menopausal women due to unnatural causes were excluded from this analysis. Figure 2 shows how the evolution is parallel in both cases with no clear effect of the classification. While there is a notable increase in sleep difficulties between 45 and 50 years, this increase occurs for the two groups of women, regardless of them being in one group or another. Menopausal status, individually, had a significant effect on the quality of sleep (OR: 1.86; 95%CI: 1.40 to 2.47; p <0.001) but, as expected, in the logistic regression bivariate (age and menopause) the second lost significance (OR: 1.11; 95%CI: 0.75 to 1.65; p=0.60), being the effect attributable to age (OR: 1.04; 95%CI; 1.02 to 1.08; p <0.001).
Discussion
This study sought to analyze both the distribution of the quality of sleep in a sample of Spanish adult population and the variations in terms of age and sex. The results show a high prevalence of poor sleep quality, reaching 38.2% of the participants. This prevalence is higher in women and increases gradually with age. Comparison with other studies is difficult because of their scarcity in the Spanish general population and the studied age range. In a younger sample (X¯=41.9 years) of primary care physicians, it was found that 35.4% had poor sleep quality.31 Outside of Spain, other studies obtained results consistent with ours, with an average score for the PSQI ranging from 4.79 to 5.28 in the studied age ranges.32 At older ages (X¯=74 years), somewhat higher scores have been reported (men: 5.95; women: 6.59), consistent with those obtained at this age range in our sample.33 And in younger subjects (38-50 years) an average of 5.7.34
The worse sleep quality found in women is consistent with the literature.11,17 Zhang and Wing16 established that women are 1.41 times more predisposed to suffer from insomnia than men at all ages but especially at advanced ages. Menopause may be related to this. Xu et al.19 found that menopausal women had a poorer sleep quality than non-menopausal. However, in our case, this potential effect is completely overshadowed by age, and menopausal status loses significance when controlling for the effect of this.
Women generally have a higher score (corresponding to a lower quality of sleep) in all subscales. So, they are twice as likely to assess their subjective sleep quality as very bad/bad or latency of more than 15minutes and are three times more likely to use medication to sleep or have disturbances during sleep. These results agree partially with studies that found differences for sleep disturbances and daytime dysfunction, but not for the other subscales.31 The much higher frequency of use of sleeping medication in women, as compared to men, is also consistent with other studies in Spanish population18,35 and would be mainly the result of the greater prevalence of sleep problems.
Age, as expected, is significantly and inversely related to sleep quality. Our data are consistent with previous literature. For example, Uhlig et al.11 reported a higher prevalence of suffering from insomnia for subjects over 50. There are also several studies that suggest a strong association between quality of sleep and age.19,22 Such association appears to depend on evolutive changes occurring throughout adult life, which involve increasing vulnerability of the regulatory system of the sleep-wake rhythm,24 affecting sleep quality. However, it is not clear if or when the age-related changes (i.e., sleep disruption or phase changes) that affect quality of sleep may be considered a sleep disorder.17
The interpretation of the results has some limitations. First, the measure of sleep quality is subjective and self-reported. Obviously objective measures (e.g., polysomnography) would offer more valid results, but its implementation is not feasible in a sample of this size. Additionally, the number of independent variables is limited and does not allow a thorough analysis of the ways in which age and gender influence sleep quality. Finally, we cannot rule out that using different methods for data collection in different sub-samples could have biased the responses.
Despite these limitations, we believe the study meets the stated objective of analyzing the prevalence of poor sleep quality in the adult Spanish population and the evolution of this problem depending on the age and sex of the subject. It also provides data, that constituting a reference for future studies to analyze the causes of this problem.
Editor in chargeClara Bermúdez-Tamayo.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Sleep quality is linked to many fundamental variables for health and disease. Sleep problems also have increased in the population however, there are no reliable and updated data on Spanish population about the prevalence of sleep quality.
What does this study add to the literature?In this study the prevalence of poor sleep quality in Spanish adult population is explored, taking into account gender differences and age effects in a representative sample. This study is a point of reference when considering the distribution of sleep quality in adult Spanish population, providing representative and updated information which allows for comparisons with other samples.
The Murcia Twin Registry has been funded by the Seneca Foundation, Regional Agency for Science and Technology of Region de Murcia (Project 03082-PHCS-05; 08633/PHCS/08; 15302/PHCS/10; and 19479/PI/14) and the Ministry of Economy and Competitiveness (PSI2009-11560 and PSI2014-56680-R).
Authorship contributionsJ.R. Ordoñana Martín and J.M. Martínez-Selva conceived and designed the study. J.J. Madrid-Valero, J.F. Sánchez-Romera and B. Ribeiro do Couto have participated at different times in the fieldwork and data analysis. J.J. Madrid-Valero, J.R. Ordoñana Martín and J.M. Martínez-Selva developed the first version of this manuscript. All signatories have made critical contributions and approved the final text.
Conflicts of interestNone.
The authors wish to thank the participants in the Murcia Twin Registry, their selfless contribution, and willingness to participate; and the Seneca Foundation for the support and confidence shown by funding both the Murcia Twin Registry and predoctoral scholarship of J.J. Madrid Valero.











