



The objective of this study was to assess the validity of two questions about the perception of intensity of exposure to secondhand smoke (SHS) at home using as a reference environmental markers (airborne nicotine and benzene) and biomarkers of exposure (cotinine in saliva and urine). This was a cross-sectional study in a convenience sample of 49 non-smoking volunteers. We found a high correlation between self-reported SHS exposure and airborne nicotine (rsp=0.806, p<0.05), salivary cotinine (rsp=0.752, p<0.05), and urinary cotinine (rsp=0.626, p<0.05). We did not find differences between the score question and the conventional ones (p >0.05). In conclusion, the significant correlation of the two questions proposed with environmental markers and personal markers indicates their potential validity to assess exposure to SHS at home.
El objetivo de este trabajo es evaluar la validez de dos preguntas sobre la exposición al humo ambiental de tabaco (HAT) en el hogar utilizando como referencia marcadores ambientales (nicotina y bencenos en el aire) y biomarcadores específicos (cotinina en saliva y orina) de la exposición pasiva al tabaco. Para ello se realizó un estudio transversal de una muestra de conveniencia de 49 voluntarios no fumadores mayores de edad de la ciudad de Barcelona. Se encontró una alta correlación entre la pregunta de intensidad de la exposición pasiva autodeclarada en casa y la nicotina en el aire (rsp=0,806, p <0,05), la cotinina en saliva (rsp=0,752, p <0,05) y la cotinina en orina (rsp=0,626, p <0,05). No encontramos diferencias entre las preguntas puntuables y las convencionales (p>0,05). En conclusión, la alta correlación de las preguntas propuestas con los marcadores ambientales y los biomarcadores indica su validez para evaluar la intensidad de la exposición pasiva al tabaco en el hogar.
World Health Organization proposed the MPOWER package in order to achieve a world where no child and adult will be exposed to second hand smoke (SHS).1 Among the measures of MPOWER, WHO encourages the monitoring (the M of MPOWER acronym) of the tobacco epidemic.
Monitoring and measurement of SHS exposure can be performed by direct and indirect methods. Among the direct methods, environmental markers (e.g., airborne nicotine and benzene) and/or personal biomarkers such as cotinine in biological matrices can be measured. Although direct methods are the most reliable to measure the SHS exposure, indirect methods –such as questionnaires– are the most commonly used in the scientific literature2,3 because they are low cost and simple to implement.4
In a previous study,5 two new questions were included to self-report the perception of intensity of exposure to SHS in hospitality venues. The main objective of this study was to assess the validity of these two questions to measure the intensity of exposure to SHS at home using environmental markers (nicotine and benzene) and personal biomarkers (salivary and urinary cotinine) as reference.
MethodsWe conducted a cross-sectional study in a convenience sample of 49 non-smoking volunteers from different houses: 25 non-smokers who lived with at least one smoker and 24 non-smokers who lived in totally smoke-free homes. The fieldwork was conducted between November 2011 and February 2012.
After an initial telephone or direct approach, a member of the research team went to the volunteer's home to explain the objective and procedures of the study. In that visit, the researcher installed two devices to passively collect nicotine and benzene in the main room of the house (usually the living room). In the second visit, one week later, the researcher returned to the volunteer's home to remove both devices from the room, to obtain saliva and urine samples from the volunteer, and to administrate a face-to-face questionnaire on SHS exposure at home. The research and ethics committee of the Bellvitge University Hospital provided ethical approval for the study protocol.
The two questions validated were: 1) “How would you describe, during the last week, secondhand smoke exposure in the room of your home where the devices were installed?” (Likert scale-based question with four possible answers: high, medium, low, and very low intensity); and 2) “What score from 0 to 10 would you give the room where devices were installed regarding the amount of secondhand smoke exposure during the last week, bearing in mind that 0 would be minimum contamination and 10 maximum contamination?”. The questionnaire also included three conventional questions to measure the intensity and duration of SHS exposure at home:3 1) “During the past week, how many persons per day usually smoked inside your home?”; 2) “During the past week, how many cigarettes (per day) have been smoked in your presence in the room where devices were installed?”; and 3) “During the past week, how many hours (per day) have you been exposed in the room where the devices were installed?”.
The sampling devices were installed in the main room following a standard protocol.6 Nicotine and benzene were extracted and analyzed by gas chromatography with detection by mass spectrometry (GC/MS) at the Laboratory of the Public Health Agency of Barcelona (Spain). The analysis of the samples of saliva and urine were performed at IMIM Hospital del Mar Medical Research Institute in Barcelona. Salivary and urinary cotinine were measured by liquid chromatography coupled to tandem mass spectrometry with multiple reactions monitoring (LC/MS/MS).
Medians and interquartile ranges (IQR) were calculated. We performed a Kruskal-Wallis test and a linear trend test to compare the concentrations of the environmental markers and personal biomarkers with the answers to the Likert scale question proposed.
Spearman correlation coefficients (rsp) were computed to assess the relationship between the intensity of exposure elicited by the score question and the markers of exposure. We compared the correlations between the scores of perceived SHS exposure proposed and the concentrations of airborne markers and biomarkers were statistically compared with those correlations between the conventional questions and the concentrations of airborne markers and biomarkers using the Meng's test.7
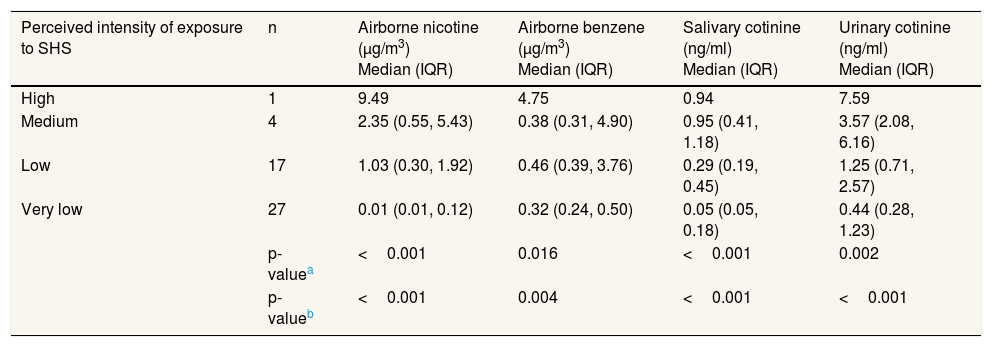
ResultsTable 1 presents the median concentrations and IQR of environmental and personal markers categorized according to the Likert scale-based question (p <0.05). We observed a positive linear relationship between the perception of SHS exposure and each of the direct measures (p <0.05).
Median concentrations and IQR of airborne markers and personal markers according to the perception of exposure to secondhand smoke at home through a Likert scale question.
| Perceived intensity of exposure to SHS | n | Airborne nicotine (μg/m3) Median (IQR) | Airborne benzene (μg/m3) Median (IQR) | Salivary cotinine (ng/ml) Median (IQR) | Urinary cotinine (ng/ml) Median (IQR) |
|---|---|---|---|---|---|
| High | 1 | 9.49 | 4.75 | 0.94 | 7.59 |
| Medium | 4 | 2.35 (0.55, 5.43) | 0.38 (0.31, 4.90) | 0.95 (0.41, 1.18) | 3.57 (2.08, 6.16) |
| Low | 17 | 1.03 (0.30, 1.92) | 0.46 (0.39, 3.76) | 0.29 (0.19, 0.45) | 1.25 (0.71, 2.57) |
| Very low | 27 | 0.01 (0.01, 0.12) | 0.32 (0.24, 0.50) | 0.05 (0.05, 0.18) | 0.44 (0.28, 1.23) |
| p-valuea | <0.001 | 0.016 | <0.001 | 0.002 | |
| p-valueb | <0.001 | 0.004 | <0.001 | <0.001 |
IQR: interquartile range.
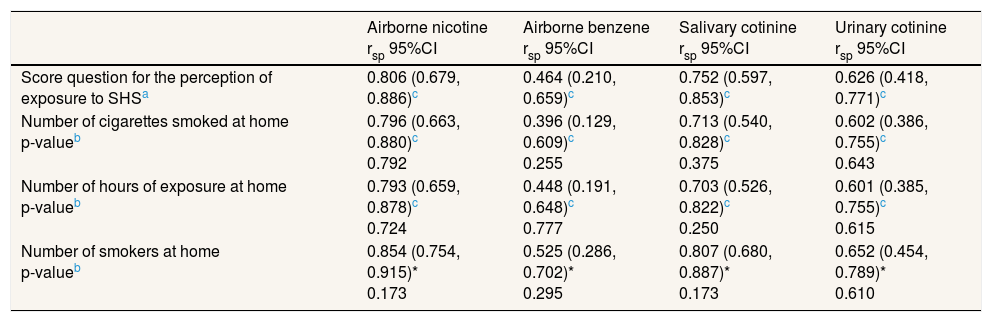
We found a high correlation of the score question with airborne nicotine (rsp=0.806, p <0.05) and moderate with benzene (rsp=0.464, p <0.05). We also found a high correlation of the score question with salivary cotinine (rsp=0.752, p <0.05) and urinary cotinine (rsp=0.626, p <0.05). We did not find statistically significant differences between the correlations of the score question proposed and the conventional ones (Table 2). When we stratified the data according to sex, age (<30 and ≥30 years), and size of the room where the devices were installed (<20 and ≥20 m2) all the correlations were similar (data not shown).
Spearman correlations (rsp) and 95%CI between airborne markers, personal markers and the score question for the perception of exposure to secondhand smoke (SHS) at home and two conventional questions for SHS assessment.
| Airborne nicotine rsp 95%CI | Airborne benzene rsp 95%CI | Salivary cotinine rsp 95%CI | Urinary cotinine rsp 95%CI | |
|---|---|---|---|---|
| Score question for the perception of exposure to SHSa | 0.806 (0.679, 0.886)c | 0.464 (0.210, 0.659)c | 0.752 (0.597, 0.853)c | 0.626 (0.418, 0.771)c |
| Number of cigarettes smoked at home p-valueb | 0.796 (0.663, 0.880)c 0.792 | 0.396 (0.129, 0.609)c 0.255 | 0.713 (0.540, 0.828)c 0.375 | 0.602 (0.386, 0.755)c 0.643 |
| Number of hours of exposure at home p-valueb | 0.793 (0.659, 0.878)c 0.724 | 0.448 (0.191, 0.648)c 0.777 | 0.703 (0.526, 0.822)c 0.250 | 0.601 (0.385, 0.755)c 0.615 |
| Number of smokers at home p-valueb | 0.854 (0.754, 0.915)* 0.173 | 0.525 (0.286, 0.702)* 0.295 | 0.807 (0.680, 0.887)* 0.173 | 0.652 (0.454, 0.789)* 0.610 |
CI: confidence interval; SHS: secondhand smoke.
Our results show that the questions proposed to self-report the intensity of SHS exposure at home were valid when assessed against concentrations of selected markers of SHS exposure (airborne nicotine and cotinine in body fluids). Moreover, the correlations between the score question and all objective markers were statistically similar to those between the conventional questions and the objective markers. In this sense, the proposed question was at least as good as the conventional quantitative questions at assessing the exposure to SHS at home. The poorest discrimination was obtained for benzene concentrations for both the conventional questions and the new questions to validate. This may be because benzene is a less specific airborne marker of SHS exposure.
Previous studies showed similar results in the assessment of self-reported SHS exposure against biomarkers8 and against airborne markers in other settings such as workplaces.9 However, many of the studies reported lower correlations to the ones obtained in ours. These differences may be explained by the fact that our questionnaire was applied immediately after the week the markers were collected, avoiding a recall bias.
The main limitation of our study is related to the use of an opportunistic limited-sized sample of volunteers. In this sense, external validity could be hampered by the non-random sample selection and the power of the experiment could be relatively low. Nevertheless, the use of an opportunistic sample allowed us to include those participants who confirmed no other potential sources of tobacco exposure in other settings. Other potential limitation is the lack of assessment of other potential sources of nicotine and benzene, such as those cumulated in the dust of homes (thirdhand smoke) from previous tobacco consumption in the homes of smokers.10 Finally, as a strength, whereas many of the previous studies measured either biomarkers or environmental markers, we were able to compare our questions to both types of markers and other conventional questions of SHS exposure.
In conclusion, the questions proposed to evaluate the perceived intensity of SHS exposure at home distinguished between different concentrations of nicotine in air and cotinine in saliva and urine. Moreover, we observed a similar discrimination with conventional questions of SHS exposure. These questions may be valid for use in future investigations to characterize SHS exposure at home, although further research in larger and more diverse samples should be conducted.
Authorship contributionsJ.M. Martínez-Sánchez, E. Fernández and I. Galán conceived the study and questions proposed to measure second hand smoke exposure. X. Sureda, M. Fu, E. Fernández and J.M. Martínez-Sánchez conducted the fieldwork. R. Pérez-Ortuño and J.A. Pascual developed the analytical method to quantify the cotinine in saliva and urine and also performed the analyses of biological samples. J.C. Martín-Sánchez and C. Lidón-Moyano prepared and analyzed the database. J.M. Martínez-Sánchez and A. González-Marrón drafted the first draft of the manuscript. All authors contributed substantially to the conception, design, and interpretation of data. All authors contributed to the manuscript and approved its final version. J.M. Martínez-Sánchez is the guarantor.
FundingThis work was supported by the Instituto de Salud Carlos III, Subdirección General de Evaluación, Government of Spain (PI081436, PI081339 and RTICC RD12/0036/0053), the Ministry of Universities and Research, Government of Catalonia (grant 2009SGR192 and 2014SGR689), the Directorate of Public Health, Ministry of Health (GFH 20051) from the Government of Catalonia, ISCIII-Subdirección General de Evaluación and by FEDER funds/European Regional Development Fund (ERDF)−a way to build Europe−. This project has received funding from the European Union's Horizon 2020 research and innovation programme under grant agreement No 681040.
Conflicts of interestNone.











