




Women who experience intimate partner violence (IPV) often do not perceive themselves as abused. This study sought to estimate the health effects of unperceived IPV (uIPV), taking violence-free women as the reference, and to compare the effects of uIPV with those of perceived IPV (pIPV).
MethodWe performed a cross-sectional population study through telephone interviews of 2835 women aged 18 to 70 years living in the region of Madrid and having an ongoing intimate partner relationship or contact with a former partner in the preceding year. Based on 26 questions from the Conflict Tactics Scale-1 and the Enquête Nacional sur les Violences envers les Femmes en France and the question “Do you feel abused by your partner?” a variable was constructed in three categories, namely, the absence of IPV, uIPV and pIPV. Using logistic regression, we analyzed the association between health problems, medication use, health-service utilization and IPV (perceived and unperceived) vis-à-vis the absence of IPV.
ResultsThere were 247 cases of uIPV and 96 of pIPV (prevalences of 8.8% and 3.4%, respectively). The multivariate analysis showed that a substantial number of the outcomes explored were associated with uIPV, pIPV, or both. The highest odds ratios (ORs) were obtained for depression (Patient Health Questionnaire-9≥10) (uIPV: OR 3.4, 95% CI 2.4-3.8; and pIPV: 4.1, 95%CI 2.5-6.8). In most problems, the ORs did not significantly differ between the two types of IPV.
ConclusionsuIPV is 2.6 times more frequent than pIPV and is associated with at least as many health problems as pIPV.
Las mujeres que sufren violencia de pareja (VPM) a menudo no se perciben a sí mismas como maltratadas. Se pretende estimar los efectos en salud de la violencia no percibida (VPMnp), tomando a las mujeres libres de violencia como referencia, y comparar con los efectos de la violencia percibida (VPMp).
MétodoEstudio transversal poblacional mediante encuesta telefónica a 2835 mujeres de 18 a 70 años de edad residentes en la Comunidad de Madrid, con relación de pareja o contacto con la ex pareja en el último año. Basándonos en 26 preguntas de la Conflict Tactic Scale-1 y de la Enquête Nacional sur les Violences envers les Femmes en France, y en la pregunta «¿se siente usted maltratada?», se construyó una variable en tres categorías: ausencia de VPM, VPMnp y VPMp. Se estudió la asociación de problemas de salud, consumo de medicamentos y frecuentación de servicios con la VPM (bien percibida o no) respecto a la ausencia de VPM, mediante regresión logística.
ResultadosSe encontraron 247 casos de VPMnp y 96 de VPMp (prevalencia del 8,8% y el 3,4%, respectivamente). En el análisis multivariado, un gran número de problemas resultaron asociados con la VPMnp, con la VPMp o con ambas. Las odds ratio (OR) más altas se obtuvieron para la depresión (PHQ9≥10) (VPMnp: OR 3,4, intervalo de confianza del 95% [IC95%] 2,4-3,8; VPMp: OR 4,1, IC95% 2,5-6,8). En la mayoría de los problemas, las OR no mostraron diferencias significativas entre los dos tipos de VPM.
ConclusionesLa VPMnp es 2,6 veces más frecuente que la VPMp y se asocia al menos a tantos problemas de salud como la VPMp.
In recent decades, intimate partner violence against women (IPV) has been clearly shown to be associated with health problems,1,2 both physical3–5 and mental.3,4,6 Early studies centred on analysis of the consequences of physical or sexual IPV;7 it soon became apparent, however, that psychological violence also caused health problems, and nowadays studies that analyse the associations between IPV and health include psychological IPV and stalking.3,6
In addition to the type of violence, other aspects, such as the duration and severity of violence, have been analysed: such research has shown more serious mental health problems in cases of prolonged abuse8 and an increase in physical and psychological symptoms when the abuse is more severe1 or different types of violence are combined.5,6
In spite of the abundance of literature on the health-related effects of different types of severity of IPV, there are no quantitative studies in Spain that examine the association between IPV and health according to whether or not the abuse is perceived as such by the victim herself.
Most abused women pass through a stage in which they do not perceive the abuse as such.9,10 In the 2006 Macrosurvey on gender violence in Spain, about three quarters of the abused women did not consider themselves as abused.11 Qualitative research reveals that women at this stage often complain of depression, anxiety and other physical and psychological symptoms.10,12
Despite its limitations, the transtheoretical model of behaviour change (TTM), initially proposed by Prochaska et al13 to describe the process of smoking cessation, is considered useful to illustrate the different stages through which women go before freeing themselves of abuse.14 In the first or so-called “pre-contemplation” stage —one that may last for years—, the woman fails to recognise the problem. In the second stage, denominated the “contemplation” stage, the woman has become aware of the problem, but does not feel ready to act. In the following stages, she begins to seek help, then implements plans to leave the relationship and finally maintains the changes already attained. The progression through these stages is not always linear: there may be jumps to later stages in response to triggers, as a sense of danger for life, or, conversely, relapses due to inappropriate responses from the environment.15
Our main research question sought to establish whether, even at the stage when women do not consider themselves as abused, IPV might have effects on their health; hence, this study aimed to assess the association between unperceived IPV (uIPV) and various health problems, medication use and health-service utilisation. The second research question sought to study the differences between uIPV and perceived IPV (pIPV) in terms of the magnitude of association with the various health outcomes.
MethodsStudy population and data-collectionIn the context of the Madrid Regional Health Authority strategy for combating gender related violence, a population-based survey is undertaken every 5 years to monitor the prevalence of IPV. This study was based on data drawn from the second population survey, undertaken from December 2009 to January 2010.
The women interviewed were aged 18 to 70 years, had been residing for a minimum of one year in the Madrid Region, and were in an ongoing intimate partner relationship and/or had been in contact with an ex-partner in the preceding year.
The women were selected by random sampling, stratified by geographical area (Madrid City; Greater Madrid; and rural) and four age groups (18/24, 25/39, 40/54 and 55/70 years), using the Health Identification Card (Tarjeta de Identificación Sanitaria) database which, at 31 December 2009, covered 99% of the catchment population.16
Information was obtained by telephone interview conducted by trained interviewers, using the Computer Assisted Telephone Interviewing system and following the safety rules and ethical recommendations for research into domestic violence.17 All interviewees could choose the most convenient time for holding their interview and of having the questionnaire administered in Spanish, Romanian or Arabic. On termination of the interview, all women were offered addresses and telephone numbers of IPV information points.
Study variables1) IPV status (principal independent variable)
The interview included 26 questions targeting: psychological, and sexual violence, based on the questionnaire of the Enquête Nacional sur les Violences envers les Femmes en France (ENVEFF);18 and physical violence, based on the Conflict Tactics Scale-119 (see Table I in Appendix online). The Spanish version was previously validated in a cross sectional study evaluating the questionnaire's violence component against an in depth personal interview with two trained psychologists.20
Based on the ENVEFF and CTS-1 definition, physical or sexual violence was defined as a positive response to any item addressing physical and sexual violence respectively, whereas psychological violence was defined as a response of “often” or “always” to an item addressing psychological violence, or as a response of “sometimes” to four or more items. IPV was defined as the presence of at least one of these three types of violence -physical, sexual or psychological- committed by the partner or ex-partner.
After the 26 violence-related questions, the interviewees were asked “Do you feel abused by your partner/ex-partner?”. On the basis of the answer to this question and the definition of IPV, the variable “IPV status”, was constructed in three categories:
- •
Absence of IPV.
- •
pIPV, where the subject met the definition of IPV and answered positively to the question.
- •
uIPV, where the subject met the definition of IPV and answered negatively to the question.
The questionnaire contained a comprehensive section covering different aspects of participants’ health, medication use and health-service utilisation.
For study purposes, the following interviewee health-related variables were considered: self-perceived suboptimal health (fair, poor or very poor); presence of limitation on usual activities due to health problems; having suffered an accident in the preceding year; current smoker status. To assess the presence of chronic problems, interviewees were asked if their physicians had told them that they were suffering from hypertension, high cholesterol, diabetes, asthma or chronic bronchitis, fibromyalgia, any type of locomotor disease, heart disease, stomach ulcer or allergy.
They were also asked if the physician or any other health professional had diagnosed a depressive disorder (major depression, dysthymia or minor depression) or anxiety disorder (acute stress disorder, panic disorder, phobia, post-traumatic stress disorder, or social anxiety disorder). Moreover, presence of depression was assessed using the nine-item Patient Health Questionnaire (PHQ9), a depression measure for population-based studies, with a score ≥10 being deemed to indicate depression.21 Its use in telephone interviews was validated by Pinto-Meza et al.22
As for medication use, the women were asked whether they had taken medical drugs belonging to the main pharmaceutical classes in the preceding two months, and whether they had received counselling support or psychotherapy.
Health-service utilisation was assessed by asking interviewees whether, at any time in the preceding year, they had made use of emergency services, had been hospitalised or had, at least once, consulted a general practitioner, nurse or midwife, social worker or any of the principal medical or surgical specialist departments.3) Variables of adjustment
As adjustment variables, we considered factors which the literature had shown to be related to both health and IPV,23 namely: age, taken as a continuous variable; country of origin; type of partner relationship (current or terminated); history of violence in the family, defined as physical abuse by a family member prior to age 15 years and/or having been witness to IPV before this age; and socio-economic deprivation, constructed on the basis of the variables of educational level, social class and monthly income,24 and defined as the presence of at least one of the following situations: primary education level or lower, monthly income of less than 1200 euros, or manual worker.
Consideration was also given to “number of types of violence”, classified as follows:
- •
One isolated type of violence (psychological, physical or sexual).
- •
Two types of violence combined (psychological + physical; psychological + sexual; physical + sexual).
- •
All three types of violence combined.
In the analysis of the consultation to the social worker, the model was also adjusted for the variable “elderly dependents”.
Statistical analysisAfter estimating the prevalence of uIPV and pIPV, we compared the characteristics of the study population by the “IPV status”, using the chi-squared test and T-test for age.
A chi-squared test was used to compare the prevalence of each health problem, medication use and health-service utilisation in women with uIPV and pIPV versus women reporting no IPV.
Multivariate logistic regression was applied to calculate the odds ratios (OR) of association and 95% confidence interval (95%CI) between each health problem, medication use and health-service utilisation (dependent variables) that showed an association at p<0.1 in the bivariate analysis, and IPV status (independent variable). Age, socio-economic deprivation, type of relationship, country of origin and history of violence before age 15 years were introduced as adjustment variables.
Focusing on abused women, we then assessed whether the ORs of association between health outcomes and pIPV were different with respect to uIPV.
All analyses were performed using the STATA v.11 statistical software package.
ResultsOf the 4862 women initially contacted, 567 did not fulfill the inclusion criteria. Of the remaining 4295, 1460 (34%) refused to participate (1231 initial refusal and 229 withdrawal from the interview). The percentage of refusals to participate was significantly higher among women aged 55 to 70 years than among those aged under 55 years (42.8% vs. 31.1%, p<0.001). Of the 2835 completed interviews, 14 were excluded due to missing data in the violence-related questions, giving a final sample of 2821 valid interviews.
A total of 247 cases of uIPV (prevalence 8.8%) and 96 cases of pIPV (prevalence 3.4%) were detected, with uIPV thus being 2.6 times more frequent than pIPV.
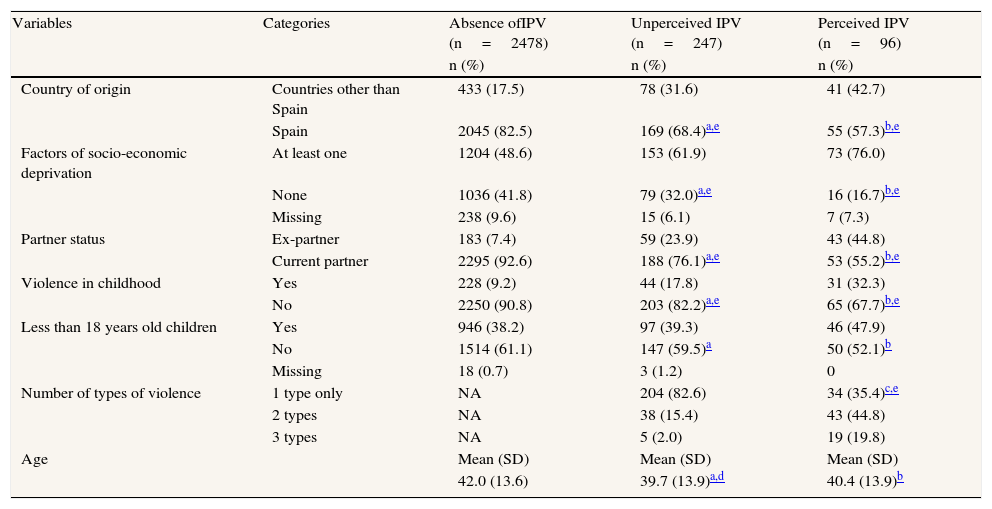
Among women in an IPV situation, whether or not perceived, there was a higher percentage of foreigners and women with socio-economic deprivation, terminated domestic partner relationships, and experience of violence before the age of 15, compared to IPV-free women (Table 1).
Characteristics of the study population according to presence and recognition of IPV (N=2821).
| Variables | Categories | Absence ofIPV (n=2478) | Unperceived IPV (n=247) | Perceived IPV (n=96) |
| n (%) | n (%) | n (%) | ||
| Country of origin | Countries other than Spain | 433 (17.5) | 78 (31.6) | 41 (42.7) |
| Spain | 2045 (82.5) | 169 (68.4)a,e | 55 (57.3)b,e | |
| Factors of socio-economic deprivation | At least one | 1204 (48.6) | 153 (61.9) | 73 (76.0) |
| None | 1036 (41.8) | 79 (32.0)a,e | 16 (16.7)b,e | |
| Missing | 238 (9.6) | 15 (6.1) | 7 (7.3) | |
| Partner status | Ex-partner | 183 (7.4) | 59 (23.9) | 43 (44.8) |
| Current partner | 2295 (92.6) | 188 (76.1)a,e | 53 (55.2)b,e | |
| Violence in childhood | Yes | 228 (9.2) | 44 (17.8) | 31 (32.3) |
| No | 2250 (90.8) | 203 (82.2)a,e | 65 (67.7)b,e | |
| Less than 18 years old children | Yes | 946 (38.2) | 97 (39.3) | 46 (47.9) |
| No | 1514 (61.1) | 147 (59.5)a | 50 (52.1)b | |
| Missing | 18 (0.7) | 3 (1.2) | 0 | |
| Number of types of violence | 1 type only | NA | 204 (82.6) | 34 (35.4)c,e |
| 2 types | NA | 38 (15.4) | 43 (44.8) | |
| 3 types | NA | 5 (2.0) | 19 (19.8) | |
| Age | Mean (SD) | Mean (SD) | Mean (SD) | |
| 42.0 (13.6) | 39.7 (13.9)a,d | 40.4 (13.9)b |
NA: not applicable; SD: standard deviation.
Most abused women who did not perceive the abuse as such were subjected to a single type of IPV, which was psychological in 90.7% of cases, physical in 5.4% and sexual in 3.9% (data not shown in the table). In contrast, women who did perceive the abuse, tended to be faced with two to three types of IPV (Table 1).
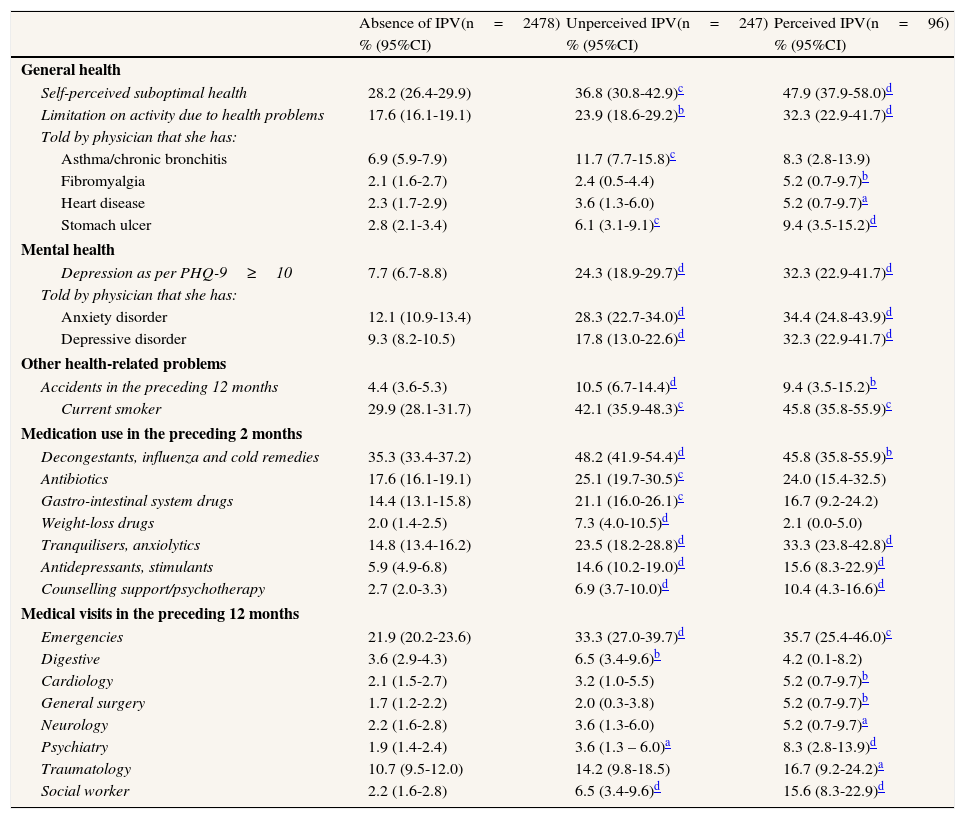
Table 2 lists all the outcomes that were associated at a value of p<0.1 with uIPV and/or pIPV, taking the violence-free population as a reference. In most of these outcomes, prevalence was higher for pIPV than for uIPV.
Prevalence of health problems, medication use and medical visits among women with no IPV, unperceived IPV and perceived IPV (N=2821).
| Absence of IPV(n=2478) | Unperceived IPV(n=247) | Perceived IPV(n=96) | |
| % (95%CI) | % (95%CI) | % (95%CI) | |
| General health | |||
| Self-perceived suboptimal health | 28.2 (26.4-29.9) | 36.8 (30.8-42.9)c | 47.9 (37.9-58.0)d |
| Limitation on activity due to health problems | 17.6 (16.1-19.1) | 23.9 (18.6-29.2)b | 32.3 (22.9-41.7)d |
| Told by physician that she has: | |||
| Asthma/chronic bronchitis | 6.9 (5.9-7.9) | 11.7 (7.7-15.8)c | 8.3 (2.8-13.9) |
| Fibromyalgia | 2.1 (1.6-2.7) | 2.4 (0.5-4.4) | 5.2 (0.7-9.7)b |
| Heart disease | 2.3 (1.7-2.9) | 3.6 (1.3-6.0) | 5.2 (0.7-9.7)a |
| Stomach ulcer | 2.8 (2.1-3.4) | 6.1 (3.1-9.1)c | 9.4 (3.5-15.2)d |
| Mental health | |||
| Depression as per PHQ-9≥10 | 7.7 (6.7-8.8) | 24.3 (18.9-29.7)d | 32.3 (22.9-41.7)d |
| Told by physician that she has: | |||
| Anxiety disorder | 12.1 (10.9-13.4) | 28.3 (22.7-34.0)d | 34.4 (24.8-43.9)d |
| Depressive disorder | 9.3 (8.2-10.5) | 17.8 (13.0-22.6)d | 32.3 (22.9-41.7)d |
| Other health-related problems | |||
| Accidents in the preceding 12 months | 4.4 (3.6-5.3) | 10.5 (6.7-14.4)d | 9.4 (3.5-15.2)b |
| Current smoker | 29.9 (28.1-31.7) | 42.1 (35.9-48.3)c | 45.8 (35.8-55.9)c |
| Medication use in the preceding 2 months | |||
| Decongestants, influenza and cold remedies | 35.3 (33.4-37.2) | 48.2 (41.9-54.4)d | 45.8 (35.8-55.9)b |
| Antibiotics | 17.6 (16.1-19.1) | 25.1 (19.7-30.5)c | 24.0 (15.4-32.5) |
| Gastro-intestinal system drugs | 14.4 (13.1-15.8) | 21.1 (16.0-26.1)c | 16.7 (9.2-24.2) |
| Weight-loss drugs | 2.0 (1.4-2.5) | 7.3 (4.0-10.5)d | 2.1 (0.0-5.0) |
| Tranquilisers, anxiolytics | 14.8 (13.4-16.2) | 23.5 (18.2-28.8)d | 33.3 (23.8-42.8)d |
| Antidepressants, stimulants | 5.9 (4.9-6.8) | 14.6 (10.2-19.0)d | 15.6 (8.3-22.9)d |
| Counselling support/psychotherapy | 2.7 (2.0-3.3) | 6.9 (3.7-10.0)d | 10.4 (4.3-16.6)d |
| Medical visits in the preceding 12 months | |||
| Emergencies | 21.9 (20.2-23.6) | 33.3 (27.0-39.7)d | 35.7 (25.4-46.0)c |
| Digestive | 3.6 (2.9-4.3) | 6.5 (3.4-9.6)b | 4.2 (0.1-8.2) |
| Cardiology | 2.1 (1.5-2.7) | 3.2 (1.0-5.5) | 5.2 (0.7-9.7)b |
| General surgery | 1.7 (1.2-2.2) | 2.0 (0.3-3.8) | 5.2 (0.7-9.7)b |
| Neurology | 2.2 (1.6-2.8) | 3.6 (1.3-6.0) | 5.2 (0.7-9.7)a |
| Psychiatry | 1.9 (1.4-2.4) | 3.6 (1.3 – 6.0)a | 8.3 (2.8-13.9)d |
| Traumatology | 10.7 (9.5-12.0) | 14.2 (9.8-18.5) | 16.7 (9.2-24.2)a |
| Social worker | 2.2 (1.6-2.8) | 6.5 (3.4-9.6)d | 15.6 (8.3-22.9)d |
95%CI: confidence interval of 95%.
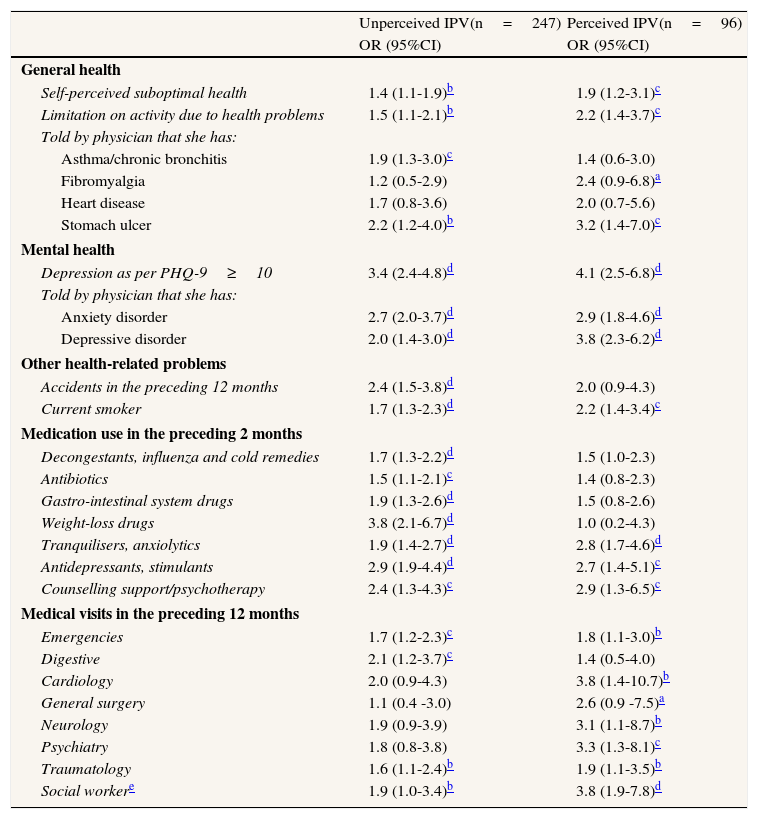
For each outcome shown in Table 2, a logistic regression model was constructed adjusting for the covariates: the association with uIPV and/or pIPV at a value of p<0.05 was confirmed for 23 of the 26 problems. The highest OR was observed for PHQ9-assessed depression, which was linked to uIPV with an OR of 3.4 (95%CI: 2.4-4.8) and to pIPV with an OR of 4.1 (95%CI: 2.5-6.8) (Table 3).
Association between health problems, medication use and diagnostic tests, and unperceived and perceived IPV, with respect to absence of IPV (N=2821).
| Unperceived IPV(n=247) | Perceived IPV(n=96) | |
| OR (95%CI) | OR (95%CI) | |
| General health | ||
| Self-perceived suboptimal health | 1.4 (1.1-1.9)b | 1.9 (1.2-3.1)c |
| Limitation on activity due to health problems | 1.5 (1.1-2.1)b | 2.2 (1.4-3.7)c |
| Told by physician that she has: | ||
| Asthma/chronic bronchitis | 1.9 (1.3-3.0)c | 1.4 (0.6-3.0) |
| Fibromyalgia | 1.2 (0.5-2.9) | 2.4 (0.9-6.8)a |
| Heart disease | 1.7 (0.8-3.6) | 2.0 (0.7-5.6) |
| Stomach ulcer | 2.2 (1.2-4.0)b | 3.2 (1.4-7.0)c |
| Mental health | ||
| Depression as per PHQ-9≥10 | 3.4 (2.4-4.8)d | 4.1 (2.5-6.8)d |
| Told by physician that she has: | ||
| Anxiety disorder | 2.7 (2.0-3.7)d | 2.9 (1.8-4.6)d |
| Depressive disorder | 2.0 (1.4-3.0)d | 3.8 (2.3-6.2)d |
| Other health-related problems | ||
| Accidents in the preceding 12 months | 2.4 (1.5-3.8)d | 2.0 (0.9-4.3) |
| Current smoker | 1.7 (1.3-2.3)d | 2.2 (1.4-3.4)c |
| Medication use in the preceding 2 months | ||
| Decongestants, influenza and cold remedies | 1.7 (1.3-2.2)d | 1.5 (1.0-2.3) |
| Antibiotics | 1.5 (1.1-2.1)c | 1.4 (0.8-2.3) |
| Gastro-intestinal system drugs | 1.9 (1.3-2.6)d | 1.5 (0.8-2.6) |
| Weight-loss drugs | 3.8 (2.1-6.7)d | 1.0 (0.2-4.3) |
| Tranquilisers, anxiolytics | 1.9 (1.4-2.7)d | 2.8 (1.7-4.6)d |
| Antidepressants, stimulants | 2.9 (1.9-4.4)d | 2.7 (1.4-5.1)c |
| Counselling support/psychotherapy | 2.4 (1.3-4.3)c | 2.9 (1.3-6.5)c |
| Medical visits in the preceding 12 months | ||
| Emergencies | 1.7 (1.2-2.3)c | 1.8 (1.1-3.0)b |
| Digestive | 2.1 (1.2-3.7)c | 1.4 (0.5-4.0) |
| Cardiology | 2.0 (0.9-4.3) | 3.8 (1.4-10.7)b |
| General surgery | 1.1 (0.4 -3.0) | 2.6 (0.9 -7.5)a |
| Neurology | 1.9 (0.9-3.9) | 3.1 (1.1-8.7)b |
| Psychiatry | 1.8 (0.8-3.8) | 3.3 (1.3-8.1)c |
| Traumatology | 1.6 (1.1-2.4)b | 1.9 (1.1-3.5)b |
| Social workere | 1.9 (1.0-3.4)b | 3.8 (1.9-7.8)d |
OR: odds ratio; 95%CI: confidence interval of 95%.
Variables of adjustment: age, history of violence in childhood, country of origin, socio-economic deprivation and type of partner relationship.
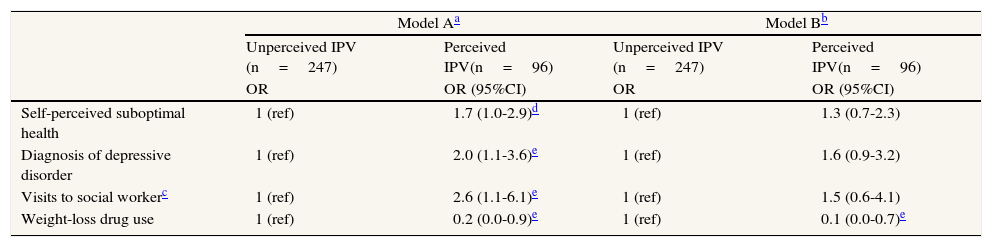
In 18 of the 26 problems analysed, the OR of association with respect to absence of IPV proved higher for pIPV than for uIPV (Table 3). Nevertheless, when we focused on the group of abused women and compared pIPV with uIPV with regard to health outcomes, only diagnosis of depressive disorder and visits to the social worker proved significantly associated with perception of the abuse; self-perceived suboptimal health was associated with a p value at the limit of statistical significance. All these associations became non-significant, however, when the variable “number of types of violence” was introduced into the models (Table 4).
Association between self-perceived health, diagnosis of depressive disorder, visits to social worker and weight-loss drug use and perceived IPV with respect to unperceived IPV, in abused women (N=343).
| Model Aa | Model Bb | |||
| Unperceived IPV (n=247) | Perceived IPV(n=96) | Unperceived IPV (n=247) | Perceived IPV(n=96) | |
| OR | OR (95%CI) | OR | OR (95%CI) | |
| Self-perceived suboptimal health | 1 (ref) | 1.7 (1.0-2.9)d | 1 (ref) | 1.3 (0.7-2.3) |
| Diagnosis of depressive disorder | 1 (ref) | 2.0 (1.1-3.6)e | 1 (ref) | 1.6 (0.9-3.2) |
| Visits to social workerc | 1 (ref) | 2.6 (1.1-6.1)e | 1 (ref) | 1.5 (0.6-4.1) |
| Weight-loss drug use | 1 (ref) | 0.2 (0.0-0.9)e | 1 (ref) | 0.1 (0.0-0.7)e |
OR: odds ratio; 95%CI: confidence interval of 95%.
Use of weight-loss drugs, in contrast, showed a stronger association with uIPV, and the association remained in evidence even after the variable “number of types of violence” had been introduced into the model.
DiscussionThe results indicate that the situation of uIPV is 2.6 times more frequent than that of pIPV, in line with the 2006 Macrosurvey.11 Edwards et al25 reported a very similar ratio of 2.3 between women in the pre-contemplation stage and those at later stages.
Among our interviewees, uIPV was characterised, in the majority of cases, by a single type of violence, which was almost invariably psychological. According to the qualitative literature, abuse often begins as isolated psychological violence that is not perceived as such,26 with initial episodes being regarded as “normal” domestic rows27 or obsessive control interpreted as love.10
The study's principal results show that uIPV is far from being harmless. The greatest magnitude of association is seen in items relating to mental health, as is widely confirmed by the literature6: when women with uIPV were compared to abuse-free women, they displayed a higher prevalence of PHQ-rated depression, diagnosis of depressive disorder and anxiety disorder, use of anxiolytics and antidepressants, counselling support/psychotherapy, and visits to the psychiatrist.
The deterioration of these women's health, however, affects areas that go beyond the purely mental: perception of suboptimal health, presence of limitation on activity due to health problems, presence of asthma, stomach ulcer, accidents in the preceding 12 months and smoking habit were all more prevalent in women with uIPV than among abuse-free women. The intake of commonly used medications, cold and influenza remedies, antibiotics and drugs for the gastro-intestinal system was likewise more frequent.
The second research question sought to ascertain whether there were differences between uIPV and pIPV in terms of the magnitude of association with the various health outcomes. Diagnosis of depression proved significantly more frequent in pIPV than in uIPV, in line with the findings of Edwards et al,25 who observed more severe mental health symptoms in the later stages. Self-perceived suboptimal health was also associated with perception of abuse, though without attaining statistical significance.
Qualitative research has shown that, when other types of violence -and physical violence in particular- are added to psychological violence, women become aware of the abuse and give the correct name to their partner's abusive behavior.10,23 When the variable “number of types of IPV” was taken into account in the analysis, the differences between uIPV and pIPV disappeared, indicating that the greater frequency of depressive disorder and self-perceived suboptimal health in pIPV is due to the accumulation of psychological, physical and sexual violence. These results agree with those published in the literature.1,5,6
With regard to the greater intake of weight-loss drugs among women who do not feel abused, our data are insufficient to advance any interpretations. While the known association between eating disorders and post-traumatic stress disorder related to sexual trauma28 may help one understand the relationship between the desire to lose weight and IPV, it does not explain why this should only be found in uIPV. The starting point for any subsequent research into this aspect should perhaps be the qualitative literature on the topic, which describes the effort made by women to maintain an ideal body image in attempt to please their abusive partners.10
Our study has the limitations specific to cross-sectional designs, with the ensuing impossibility of establishing temporal and causal relationships. Longitudinal studies have shown that IPV influences depression,29 just as depression can precede and facilitate IPV.30 This latter relationship is plausible in some cases of mental disease, since a depressed woman may well be more vulnerable and more exposed to IPV. However, it is inapplicable to other aspects of health, with it being very difficult to explain why asthma or smoking would increase IPV. The high number and the types of items positively associated with IPV leads us to surmise that, in general, IPV precedes and has a causal role in health problems, a conclusion supported by the literature, which documents the deterioration in overall health when IPV persists over time31 and the improvement in mental health when violence ceases.32
Another limitation is that it is not possible to say whether a woman who states that she does not feel abused perceives in reality the relationship as abusive, but is either unwilling or unable to reveal this to others. We should therefore consider that the uIPV category includes women who do not want to disclose the abuse.
Although population-based surveys are considered the best way to obtain accurate data on the prevalence of IPV33 and Caetano et al34 found that violence related variables are not the main factors determining participation in the survey, some degree of bias due to non-response rate of 34% could exist, especially because the participation rate was not homogeneous through the age groups.
The TTM used as a framework has a number of limitations we have to take into account. First of all, an abusive relationship is not comparable to substance addiction or other dysfunctional behaviours to which the TTM has been applied. As Chang et al15 observe, it is the perpetrator, and not the woman, the one who has a problem behaviour. Even if there is for the woman some room for action, her behaviour changes occur in the context of a relationship, where the counter-reaction of the abuser determines the subsequent evolution. The TTM probably is insufficient to capture the complexity of IPV; nonetheless it is a useful tool to guide the professional in supporting the woman according with her timeline.35
The documentation in this study attesting to the high prevalence of uIPV and its association with the same number of health problems as pIPV highlights the need for the efforts of health professionals and public health to be targeted at unperceived abuse, so as to help women recognise their situation and take the necessary decisions to preserve their health. Health professionals, aware of the fact that certain health problems may be linked to unperceived abuse, could contribute to awareness of IPV by helping women establish a link between their physical and psychological problems and their partner's abusive behavior.14
As can be seen from the results, asking a woman directly in a survey whether she felt abused would result in the majority of cases going undetected. In all likelihood, this direct question would prove equally inappropriate in clinical practice, where it is advisable to use suitable interview techniques adjusted to the stage in which the woman finds herself, as suggested by the guidelines drawn up to address IPV in a health-care context.35,36
About three quarters of the women experiencing intimate partner violence (IPV) do not consider themselves abused. The effects of IPV on women's health are well documented; it is not known, however, whether such health effects are present when women still fail to perceive the abuse as such.
What does this study contribute to the literature?Our results suggest that unperceived IPV is far from being harmless and is associated with at least as many health problems and as much medication use and health-service utilization as perceived IPV. Depression and other mental health problems show the greatest magnitude of association, but women experiencing unperceived IPV are also more likely than abuse-free women to report suboptimal self-rated health, asthma, stomach ulcer, accidents in the preceding 12 months and smoking habit. Greater public-health efforts are needed to address unperceived abuse, in order to help women recognise the problem and take appropriate decisions to preserve their health and wellbeing.
M. Sonego and A. Gandarillas contributed to conception and design, analysis and interpretation of data, drafting the manuscript and final approval of the version published. B. Zorrilla, L. Lasheras, and M. Pires contributed to conception and design, acquisition of data, interpretation of data, revising the article critically for important intellectual content and final approval of the version published. A. Anes and M. Ordobás contributed to analysis and interpretation of data, revising the article critically for important intellectual content and final approval of the version published.
FundingNone.
Conflict of interestNone.












