



The 3rd International Nursing and Health Sciences Students and Health Care Professionals Conference (INHSP)
Más datosThis study aimed to analyze the effectiveness of gentle prenatal yoga toward depression and abnormal serotonin hormone levels in pregnant women aged <20 and >35 years old.
MethodThis study was conducted at Bara Baraya Health Center, Antang Health Center, Kapasa Health Center, and Mamajang Health Center. The applied research design in this study was a quasi-experiment with a non-equivalent control group design approach. Samples were selected using a purposive sample technique. The instrument used was the Beck Depression Inventory (BDI) questionnaire. The number of samples in this study was 24 respondents divided into 2, 12 in the intervention group and 12 in the control group. Sample criteria in this study were pregnant women aged <20 and >35 years old, having been in trimester II-III with the gestational age of ≥20 to <31 weeks, and not having complications in pregnancy.
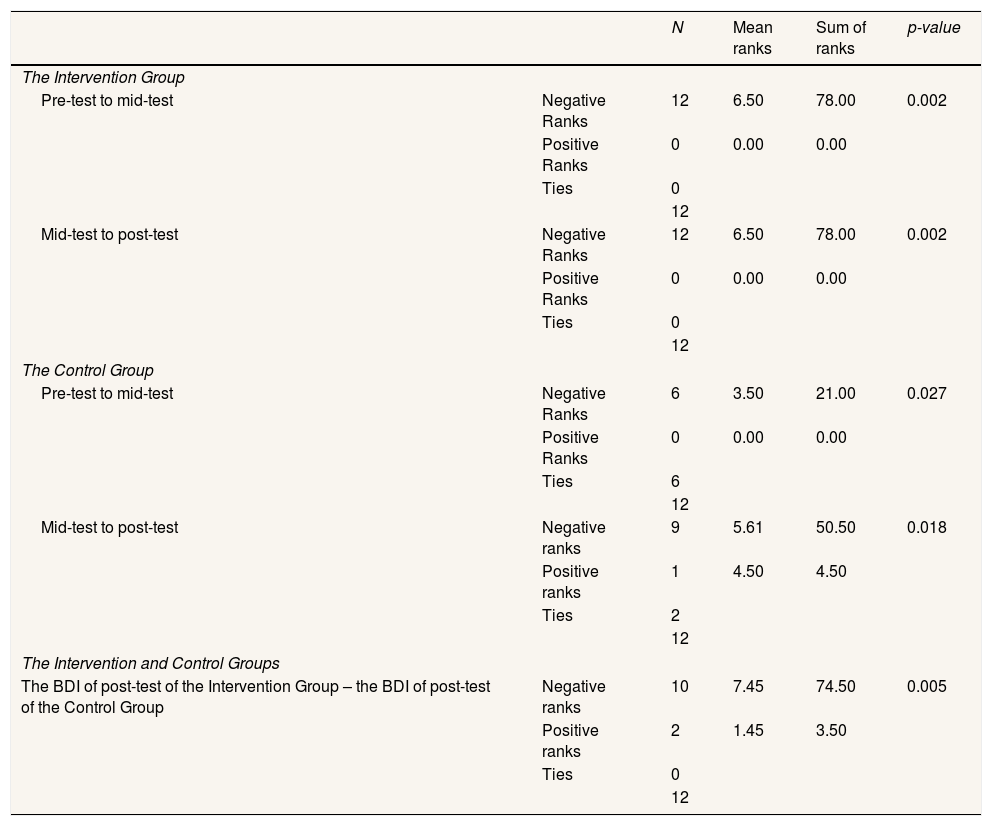
ResultsThe mean values for the intervention group were 6.50 in the pre-test to the mid-test and 6.50 in the mid-test to the post-test. Meanwhile, the mean values for the control group were 5.61 in the pre-test to the mid-test and 4.50 in the mid-test to the post-test. This indicated that the intervention group experienced a significantly reduced level of depression based on the BD-II (Beck Depression Inventory-II) scores when compared to the control group. Furthermore, based on the comparison of the post-test data between the intervention group and the control group, it was obtained the p-value of 0.005 (α<0.05).
ConclusionThere were differences in BDI-II (Beck Depression Inventory-II) scores between the intervention group and the control group after receiving prenatal gentle yoga treatment.
During pregnancy, women are very vulnerable to experience psychological disorders. One of the psychological disorders is depression. Depression in pregnant women occurs due to the failure of coping mechanisms of pregnant women during the anxiety period. Generally, depression is a complex mood disorder that is a situation in which individuals are unable to relieve the pressure that occurs that refers to emotional disorders. Depression comes from the word “depressare” and the Latin classic word “deprimere”. “Deprimere” literally means “press down” or interpreted as “under.” Meanwhile, “premere” means “depressed.” Therefore, depression can be concluded as depressed, sad, upset, and inferior feelings.1 Depression is a mood disorder that causes loss of energy and interest, feeling guilty, difficulty concentrating, experiencing loss of appetite, or even thought of death or committing suicide, followed by other symptoms on changes in activity, cognitive abilities, speech, and vegetative function (including sleep, sexual activity, and other biologic rhythms).2
Several factors influence depression in pregnant women. Besides being influenced by hormonal factors, it is also influenced by the age of women during pregnancy. Women who are pregnant at the age of <20 years old are very susceptible to psychological disorders that can trigger complications in pregnancy. Complications during pregnancy are one of the leading causes of death among women aged 15–19 years old.3 Meanwhile, risks for pregnant women aged over 35 years old, especially primigravida, are medical risks associated with an aging reproductive system and an aging body.4 During pregnancy, women experience significant changes in their physiological and psychological functions. The process of adjusting to this new situation can then cause psychological disorders. Pregnancy is a period of crisis that involves profound psychological factors that occur because of enormous somatic changes. This is caused by hormonal changes, which then also lead to pregnant women's emotions becoming unstable. In addition to physical factors, psychosocial factors can also increase the psychological burden on pregnant women. It can also be influenced by information about the birthing experience that they receive.5 To determine the level of psychological problems in pregnant women, it can be found out by using a BDI measurement scale.6 The Beck Depression Inventory-Second Edition (BDI-II) is a rating scale consisting of 21 multiple response items to assess the severity of depressive symptoms, including cognitive (psychological) and somatic (physical) symptoms. Patients are asked to consider each question item related to their feelings during the past two weeks. The BDI has shown good psychometrics in the population of pregnant women. Based on a study of the American College of Obstetricians and Gynecologists Committee Opinion No. 453, it is an appropriate screening tool in the population of pregnant women patients.7
The undertaken management in midwifery to reduce depression and childbirth experience of pregnant women is physical exercise such as the pregnancy exercise, the Lamaze method, meditation, prenatal yoga, or relaxation yoga. A pregnancy exercise is a form of exercise programmed by the technical implementation unit of the health service to prevent pregnancy complications. However, according to a study conducted by Fitriani (2018),8 prenatal yoga is more effective than pregnancy exercise in reducing back pain in pregnant women.9 It can be seen from the mean value of prenatal yoga that it is greater than the mean value of pregnancy exercise. This is also in line with a study conducted by Field et al. (2014) that yoga has a more positive effect on pregnant women reducing stress, anxiety, and sleep disorders. It is also in line with a study conducted by Rao et al. (2015) that, based on a systematic review, yoga effectively reduces anxiety, depression, and acute and chronic pain in the population of adults without side effects. Therefore, intervention with yoga can also improve psychological health (anxiety, depression, depression, and stress) and improve quality of life.
MethodsThe applied research design in this study was a quasi-experiment with a non-equivalent control group design approach. The design involved two groups, i.g. the intervention group and the control groups. Each group was tested three times, i.e. pre-test, mid-test, and post-test. The instrument used was the Beck Depression Inventory (BDI) questionnaire. The number of samples in this study was 24 respondents divided into 2, 12 in the intervention group and 12 in the control group. Sample criteria in this study were pregnant women aged <20 and >35 years old, having been in trimester II-III with the gestational age of ≥20 to <31 weeks, and not having complications in pregnancy.
Research locationThis study was conducted from January to June 2020 and had received an ethical approval recommendation with protocol number UH19121115. The study was conducted in four health centers in Makassar, i.g. Bara Baraya Health Center, Antang Health Center, Kapasa Health Center, and Mamajang Health Center.
Data sourceThe collected data was demographic data (age, educational level, and occupation) and respondents’ depression level data using questionnaire sheets in the form of the Beck Depression Inventory-II (BDI-II).
Data collection techniqueThe researcher gave questionnaire sheets in the form of the Beck Depression Inventory Scale-II (BDI-II). After that, the obtained data were then documented on the observation sheet.
Data analysisThe applied analysis method and statistical tests depend on the analyzed variable. In this study, the applied analysis method was comparative hypothesis testing for numerical variables with abnormal data distribution using the Wilcoxon test.
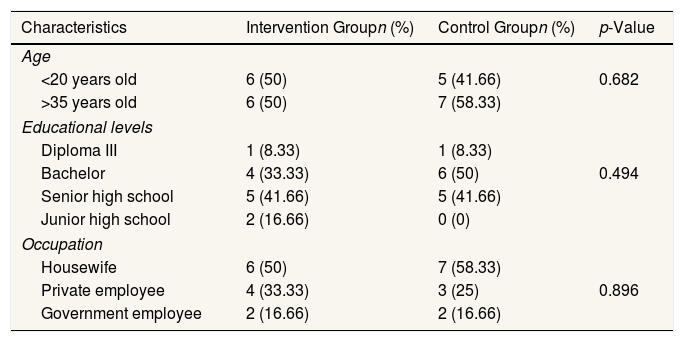
ResultsCharacteristics of respondents.
| Characteristics | Intervention Groupn (%) | Control Groupn (%) | p-Value |
|---|---|---|---|
| Age | |||
| <20 years old | 6 (50) | 5 (41.66) | 0.682 |
| >35 years old | 6 (50) | 7 (58.33) | |
| Educational levels | |||
| Diploma III | 1 (8.33) | 1 (8.33) | |
| Bachelor | 4 (33.33) | 6 (50) | 0.494 |
| Senior high school | 5 (41.66) | 5 (41.66) | |
| Junior high school | 2 (16.66) | 0 (0) | |
| Occupation | |||
| Housewife | 6 (50) | 7 (58.33) | |
| Private employee | 4 (33.33) | 3 (25) | 0.896 |
| Government employee | 2 (16.66) | 2 (16.66) | |
a Chi-squared test.
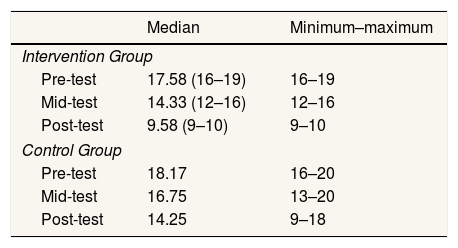
The result of the Wilcoxon test on the comparison of BDI-II scores of pre-test, mid-test, and post-test of the intervention and control groups.
| Median | Minimum–maximum | |
|---|---|---|
| Intervention Group | ||
| Pre-test | 17.58 (16–19) | 16–19 |
| Mid-test | 14.33 (12–16) | 12–16 |
| Post-test | 9.58 (9–10) | 9–10 |
| Control Group | ||
| Pre-test | 18.17 | 16–20 |
| Mid-test | 16.75 | 13–20 |
| Post-test | 14.25 | 9–18 |
a Wilcoxon signed-rank test.
The result of hypothetical testing using wilcoxon test on the comparison of BDI-II scores of pre-test, mid-test, and post-test of the intervention and control groups.
| N | Mean ranks | Sum of ranks | p-value | ||
|---|---|---|---|---|---|
| The Intervention Group | |||||
| Pre-test to mid-test | Negative Ranks | 12 | 6.50 | 78.00 | 0.002 |
| Positive Ranks | 0 | 0.00 | 0.00 | ||
| Ties | 0 | ||||
| 12 | |||||
| Mid-test to post-test | Negative Ranks | 12 | 6.50 | 78.00 | 0.002 |
| Positive Ranks | 0 | 0.00 | 0.00 | ||
| Ties | 0 | ||||
| 12 | |||||
| The Control Group | |||||
| Pre-test to mid-test | Negative Ranks | 6 | 3.50 | 21.00 | 0.027 |
| Positive Ranks | 0 | 0.00 | 0.00 | ||
| Ties | 6 | ||||
| 12 | |||||
| Mid-test to post-test | Negative ranks | 9 | 5.61 | 50.50 | 0.018 |
| Positive ranks | 1 | 4.50 | 4.50 | ||
| Ties | 2 | ||||
| 12 | |||||
| The Intervention and Control Groups | |||||
| The BDI of post-test of the Intervention Group – the BDI of post-test of the Control Group | Negative ranks | 10 | 7.45 | 74.50 | 0.005 |
| Positive ranks | 2 | 1.45 | 3.50 | ||
| Ties | 0 | ||||
| 12 | |||||
a Wilcoxon signed-rank test.
Based on the statistical tests in Table 1, the characteristics of the respondents did not show a significant difference based on age, educational level, and occupation between respondents from the intervention group and the control group.
Furthermore, in Table 2, the BDI-II scores of the intervention group showed that a median value of the pre-test was 17.58, meaning that respondents were in the clinical depression threshold. In the mid-test, it was 14.33, meaning that respondents were in the category of mild mood disorders. In the post-test, it was 9.58, meaning that respondents were in the category of fair mood. Meanwhile, the BDI-II scores of the control group showed that a median value of the pre-test was 18.17, meaning that respondents were within the clinical depression threshold. In the mid-test, it was 16.75, meaning that respondents were still in the category of the clinical depression threshold. In the post-test, it was 14.25, meaning that respondents were in mild mood disorders.
Table 3 showed the Wilcoxon test result on the post-test between the Intervention group and the control group. From the table, the obtained p-value was 0.005 (α< 0.05). Therefore, it can be concluded that there were differences in BDI-II (Beck Depression Inventory-II) scores between the intervention group and the control group after being given a prenatal gentle yoga treatment. After being given the prenatal gentle yoga treatment eight times, the difference in BDI-II (Beck Depression Inventory) scores can be seen, which was very significant between the intervention group and the control groups. Although both groups experienced decreased BDI-II scores, the number of respondents who experienced a score decreased was still different. The number of respondents in the intervention group who experienced decreased BDI-II scores was higher than the number of respondents in the control group. The mean values for the intervention group were 6.50 in the pre-test to the mid-test and 6.50 in the mid-test to the post-test. Meanwhile, the mean values for the control group were 5.61 in the pre-test to the mid-test and 4.50 in the mid-test to the post-test. This indicated that the intervention group experienced a significant decrease in depression on the BDI-II (Beck Depression Inventory-II) scores compared to the control group. Therefore, it can be concluded that prenatal gentle yoga treatment affected the recovery of depression levels in pregnant women aged <20 and >35 years old.
Depression is a leading cause of mental disability and is a significant contributor to disease throughout the world. Globally, the prevalence of depression and depressive symptoms has increased in the last few decades. Depression is one of the most common disorders affecting women during pregnancy.10 The prenatal period of being a mother is a challenging period that can cause significant psychological, social, and biological changes and has been considered as a gate of increased vulnerability to the development of mental illness.5 Depression is a complex mood disorder in pregnant women. Prenatal depression can negatively affect the physical and mental health of the mother and fetus. Antidepressant therapy can reduce symptoms of prenatal depression. However, it has a negative impact on the body. Antidepressant therapy can increase the risk of postpartum bleeding and adversely affect the fetus. Therefore, yoga is currently being developed for pregnancy. It aims to restore the physiological functions of the body by regulating the balance between the body and mind.11
The prenatal gentle yoga treatment influences the decreased BDI-II (Beck Depression Inventory-II) scores. The yoga movement covers a combination of physical postures and spiritual practices, aiming to make the body relax so that the body and mind become calm and comfortable.
Prenatal gentle yoga is yoga that is designed to be safe, gentle, and very helpful for pregnant women. It is an appropriate strategy for treating maternal depression. One of the principles of prenatal yoga is to increase attention, empower, and focus on the health of the mind of pregnant women.12 A study conducted by Field et al. (2008)13 has mentioned the positive effects of yoga for pregnant women, namely to reduce stress, anxiety, and physical complaints during pregnancy, to reduce the discomfort of pregnancy, to minimize birthing pain, and to accelerate the opening of the birth canal during birthing.14 Prenatal gentle yoga is considered to have effects to improve nervous system regulation and the function of the physiological system (immunity, endocrine, neurotransmitter, and cardiovascular) and improve the mind's health to achieve a balance between the body and mind. Therefore, it can reduce hypertension during pregnancy, premature birthing, and the Section Caesarea (SC).15
ConclusionThe provision of prenatal gentle yoga treatment effectively reduces depression levels in pregnant women aged <20 and >35 years old. This was indicated by the results of BDI-II (Beck Depression Inventory-II) scores before being given the treatment (pre-test), four weeks after being given the treatment (mid-test), and eight weeks after being given the treatment (post-test). The result showed that pregnant women experienced decreased levels of depression.
Conflicts of interestThe authors declare no conflict of interest.
Peer-review under responsibility of the scientific committee of the 3rd International Nursing, Health Science Students & Health Care Professionals Conference. Full-text and the content of it is under responsibility of authors of the article.










