




To describe serum levels of calcium, copper, selenium, magnesium, iron and zinc and evaluate their relationship with maternal socio-demographic characteristics and dietary variables in women in the first trimester of pregnancy.
MethodCross-sectional study with 1279 participants from the INMA cohorts.
ResultsThe concentrations of the elements analyzed were within the normal range. Associations with higher levels of these metals were found for calcium with white meat intake (p=0.026), for copper with excess body weight (p <0.01), low social class (p=0.03) and being multipara (p <0.01), for magnesium with being over 35 years old (p=0.001), high social class (p=0.044), primiparous status (p=0.002) and low daily intake of bread (p=0.009) and legumes (p=0.020); for zinc with university education (p=0.039) and residence in Gipuzkoa (p <0.01), and for selenium with residence in Valencia (p <0.01), university education (p=0.001), vitamin B6 supplementation (p=0.006), fish intake (> 71g/day) (p=0.014) and having been born in Spain (p=0.001). Further, lower iron levels were associated with being overweight (p=0.021) or obese (p <0.001) and vitamin B12 supplementation (p=0.006).
ConclusionsOur results suggest that trace elements in the analyzed cohorts are adequate for this stage of pregnancy. The variability in these elements is mainly linked to socio-demographic and anthropometric variables.
Describir las concentraciones de calcio, cobre, selenio, magnesio, hierro y zinc en muestras de suero de gestantes en el primer trimestre y evaluar la relación con las características sociodemográficas maternas y las variables de dieta.
MétodoEstudio transversal con 1279 participantes de las cohortes INMA.
ResultadosLas concentraciones de los elementos analizados estuvieron dentro de los límites de referencia. El calcio se asoció con el consumo de carne blanca (p=0,026). Los valores elevados de cobre se asociaron con tener exceso de peso (p <0,01), clase social baja (p=0.03) y ser multípara (p <0,01). Los valores más elevados de magnesio se asociaron con tener más de 35 años (p=0,001), clase social alta (p=0,044), ser primípara (p=0,002) y bajo consumo diario de pan (p=0,009) y legumbres (p=0,020). El zinc se asoció con tener estudios universitarios (p=0,039) y con la cohorte de Gipuzkoa (p <0,01). Los valores más altos de selenio se asociaron con la cohorte de Valencia (p <0,01), tener estudios universitarios (p=0,001), tomar suplementos de vitamina B6 (p=0,006), consumo de pescado>71g/día (p=0,014) y ser española (p=0,001). Los valores más bajos de hierro se asociaron con tener exceso de peso (p=0,021) u obesidad (p <0,001) y con tomar suplementos de vitamina B12 (p=0,006).
ConclusionesNuestros resultados sugieren que los oligoelementos en las cohortes analizadas son adecuados para esta etapa del embarazo. La variabilidad de estos elementos está asociada principalmente a las variables sociodemográficas y antropométricas.
Trace elements are bioelements that play a significant role in keeping the body healthy.1 The human body cannot produce them, and therefore, we need to obtain them at appropriate doses from our diet. Both deficiency and excess may have a negative impact on body functions and the body's needs vary depending on the stage of the growth. Nutrition is vital during pregnancy for both the expectant mother and the developing fetus. Notably, the nutritional requirements of pregnant women differ from those of non-pregnant women of the same age. They also vary according to the week of pregnancy, with few differences compared to non-pregnant women during the first trimester; demands increasing during the second trimester; and a sharp rise during the third trimester, due to the rapid development of the fetus. Daily dietary reference intakes (DRIs) for pregnant women in Spain, published by the Spanish Federation of Nutrition, Food and Dietetics Societies2 in 2010 were: 1000-1300mg/d for calcium (Ca), 350-400mg/d for magnesium (Mg), 1000μg/d for copper (Cu), 27mg/d for iron (Fe), 60μg/d for selenium (Se) and 11-13mg/d for zinc (Zn). Serum levels in the following ranges are considered normal: Ca 8.5-10.2mg/dL, Fe 60-180μg/dL, Mg 0.75-1.25 mmol/L, Cu 70-140μg/dL, Se 70-150 ng/mL and Zn 0.66-1.10μg/mL.3
Fe is necessary for proper development of the placenta, as well as bone and organ formation in the fetus. Iron-deficiency anemia is relatively common among pregnant women and may increase the risk of some complications, including preterm delivery and low infant birth weight. To prevent maternal anemia, it is recommended that pregnant women take a daily oral supplement of 30 to 60mg of elemental Fe.4
Zn is important for protein synthesis, cell division, and nucleic acid metabolism. Deficiency in this element is manifested in different ways, depending on its severity, but in particular, may have a negative impact on the nervous and reproductive systems. Cu is essential for oxidative metabolism, cell growth, development of connective tissue and hemoglobin synthesis.5 Deficiency in this element can cause bone deformations, as well as cardiovascular problems. Se is part of the key enzyme glutathione peroxidase, seems to be involved in platelet function and helps to neutralize heavy metals such as mercury, lead, arsenic and cadmium. Further, deficiency in this element affects all components of the immune system. During pregnancy, there is active transport to the fetus through the placenta and Se deficiency is reported to be associated with a variety of adverse outcomes including miscarriage, preterm delivery, gestational diabetes and preeclampsia.6
Mg is a key element for fetal growth and is one of the most abundant nutrients in the human body. It is involved in cellular respiration, protein synthesis, maintenance of cardiovascular health, regulation of cellular function and the action of collagen, among many other functions. Deficiency in Mg during pregnancy has been associated with preeclampsia and preterm delivery, as well as low infant birth weight.7
Lastly, Ca is another element necessary for normal fetal growth.8 Among its functions, in addition to providing structure and rigidity to the bones, it plays a key role in muscle contractility, the transmission of signals from the brain nerves to the rest of the body, the circulation of the blood and the production of hormones and enzymes for various body functions. Lower maternal serum Ca levels have been associated with pregnancy-induced hypertension and preeclampsia.
The objective of this work was to describe serum levels of Ca, Fe, Mg, Se, Cu and Zn, and evaluate their relationship with maternal socio-demographic, anthropometric and dietary variables in women from cohorts from Valencia and Gipuzkoa (Spain) in their first trimester of pregnancy.
MethodStudy populationStudy participants were enrolled in the INMA Project (from the Spanish: Infancia y Medio Ambiente, meaning childhood and the environment: www.proyectoinma.org). A cross-sectional study was designed. We gathered information from women in the INMA Valencia and Gipuzkoa cohorts during their routine check-up in the first trimester of pregnancy (Valencia n=855; Gipuzkoa n=638). The final study population was composed of 1279 women (Valencia n=656, Gipuzkoa n=623). Samples were collected between February 2004 and June 2005 in Valencia and between May 2006 and February 2008 in Gipuzkoa, and Mg was only analyzed in the Valencia cohort (n=656). Informed consent was obtained from all the participants before inclusion. The hospital ethics committees of each area approved the research protocols.
Socio-demographic and dietary characteristicsData on socio-demographic characteristics were collected through questionnaires. Occupational status data were classified into two categories according to whether the women were in work. Social class was based on occupation and five categories were considered in accordance with the Spanish adaptation of the British Registrar General's Social class classification (I being the highest socioeconomic position and V the lowest). In order to increase the statistical power for the analysis, social class was further grouped into two categories: manual worker or lower class (IV and V) and non-manual worker or higher class (I-III). Educational level was classified according to the highest level attained into three categories: up to primary school, secondary school and university. Body mass index (BMI) before pregnancy was classified as underweight: <18.5km/m2; normal weight: 18.5-24.9kg/m2; overweight: 25-29.9kg/m2; or obese: ≥ 30kg/m2. Smoking status information was classified as: smoker during pregnancy, quit at the beginning of pregnancy, ex-smoker (quit earlier than at the beginning of pregnancy) or never-smoker. The daily consumption of alcohol was recorded as grams of alcohol consumed daily and was subsequently categorized into two categories: ≤ 5g/day and> 5g/day. Food and mineral or vitamin supplement intake was also evaluated using a food-frequency questionnaire (FFQ) during pregnancy. The FFQ used was a version of Willett's questionnaire adapted for use in a Spanish population9. Regarding vitamin and mineral supplementation, information was collected on the intake of vitamin B6,vitamin B12, vitamin D,Ca,Fe,Mg and Zn supplements. The food frequency variables were categorized at the median for the analysis.
Chemical analysis- 1)
Sample preparation
Serum samples were prepared for ICP-MS analysis by a direct alkali dilution method. Briefly, samples were diluted 1:15-50 with an alkali solution consisting of 2% butanol (Honeywell Research Chemicals, Seelze, Germany), 0.05% EDTA (Sigma-Aldrich, St. Louis MO, USA), 0.05% Triton X-100 (Sigma- Aldrich),1% NH4OH (Romil,Cambridge,UK) and 20μg/g of the internal standards Sc,Ge and Rh. Finally, the samples were vortexed and analyzed.
- 2)
Instrumentation and analysis
An inductively coupled plasma mass spectrometry system (Agilent 7700x ICP-MS, Agilent Technologies, Tokyo, Japan) equipped with an octopole reaction system, employing a collision/reaction cell, was used for measuring concentrations of six elements in human serum: Ca, Mg, Fe, Cu, Zn, and Se. Two modes were used for the analysis of Se: collision mode using helium and reaction mode using hydrogen gas. The hydrogen mode has certain benefits over using helium for Se analysis. Hydrogen removes doubly charged species, and due to its smaller size, it can increase the sensitivity of Se measurements.
- 3)
Quality control
The level of detection for each element was estimated as three times the standard deviation (SD) of blanks (alkali solution) and a signal-to-noise ratio of 3. The accuracy and precision of each measurement was verified by analyzing commercially available reference materials: Seronorm human serum lot MI0181 (SERO, Billingstad, Norway) and NIST animal serum SRM 1598a (National Institute of Standards and Technology, Gaithersburg MD, USA).
Blanks and reference materials were treated along with the serum samples collected and analyzed at the beginning, in the middle and at the end of each run. Metal concentrations were corrected according to the variations in the three daily measurements of the Seronorm reference material. The correction was performed by adding to each measurement the difference between the daily mean of the reference measures and the overall mean of the reference measures. These measurements were performed at the Institute of Environmental Medicine at the Karolinska Institutet (Sweden).
Statistical analysisDescriptive statistics were calculated for each metal. A bivariate analysis was carried out between each metal and the defined variables overall and by cohort. Student's t-test or analysis of variance was performed depending on the number of categories of the independent variable (see Appendix online). Multivariable linear regression models were built to estimate the association between serum levels of metals and the independent variables. The variables with a p ≤ 0.20 in the bivariate analysis were initially included in the models and those that were statistically significant (p <0.05) were kept in the model, following a backward selection procedure. Statistical analyses were carried out using IBM SPSS for Windows, version 24.
We also performed permutational multivariate analysis of variance to test the null hypotheses of no association between multivariate variance in serum levels of Ca, Cu, Fe, Se and Zn, and socio-demographic and dietary variables. To this end, two multivariate linear models were built: the first only considered dietary explanatory variables; and the second, only socio-demographic explanatory variables. The method for variable selection that we applied was stepwise backward regression. Finally, we also built a joint (socio-demographic-dietary) model with the variables selected in the former step and then applied the method of Borcard et al.10 to partition multivariate variance in serum levels of the metals into components explained by socio-demographic factors, by dietary factors, and by a shared fraction.
ResultsWe analyzed data from serum samples of 1279 women (51.3% from the Valencia cohort). Sample size, percentages and missing values of all the variables are shown in Table 1. Overall, 92% had been born in Spain, 61.3% were 30 years old or older, with a mean age of 30.7 years (31.3 and 30.1 years for the Gipuzkoa and Valencia cohorts respectively), 50.1% lived in urban areas, 77.2% had secondary or university studies, 78.5% were active workers, 51% belonged to the lowest social class and 55% were primipara. In relation to other variables, 24.7% had excess body weight, 17.4% smoked during pregnancy, 14.9% had smoked but quit before pregnancy and 1.1% consumed more than 5g of alcohol per day.
Maternal anthropometric, socio-demographic, and dietary characteristics.
| Variable | CategoriesMeana | N | %SDa | Missing data |
|---|---|---|---|---|
| 1279 | 100 | |||
| Socio-demographic variables | ||||
| Cohort | Gipuzkoa | 623 | 48.7 | 0 |
| Valencia | 656 | 51.3 | ||
| Season | Spring | 332 | 26.0 | 0 |
| Summer | 350 | 27.4 | ||
| Autumn | 303 | 23.7 | ||
| Winter | 294 | 23.0 | ||
| Country of birth | Spain | 1175 | 91.9 | 0 |
| Other | 104 | 8.1 | ||
| Age (years) | 30,7a | 4.1a | ||
| Age-cat (years) | <25 | 84 | 6.6 | 0 |
| 25-29 | 412 | 32.2 | ||
| 30-34 | 570 | 44.6 | ||
| ≥35 | 213 | 16.7 | ||
| Residence | Urban | 636 | 50.1 | 10 |
| No urban | 633 | 49.9 | ||
| Physical activity before pregnancy | <1 hour/week | 768 | 60.0 | 16 |
| 1-3 hours/week | 316 | 24.7 | ||
| >4 hours/week | 179 | 14.0 | ||
| Social class | No manual | 629 | 49.2 | 0 |
| Manual | 650 | 50.8 | ||
| Educational level | Up to Primary | 291 | 22.8 | 2 |
| Secondary | 511 | 40.0 | ||
| University | 475 | 37.2 | ||
| Mother's smoking habit | Never-smoker | 526 | 42.3 | 37 |
| Ex-smoker | 315 | 25.4 | ||
| Quit at the beginning of pregnancy | 185 | 14.9 | ||
| Smoker in pregnancy | 216 | 17.4 | ||
| Mother alcohol consumption | ≤5 g/day | 1249 | 97.7 | |
| >5 g/day | 14 | 1.1 | ||
| Mother alcohol consumption (g/day) | 0.28a | 1.1a | ||
| Parity | Primipara | 699 | 54.7 | 0 |
| Multipara | 580 | 45.3 | ||
| Gestation week | 13.10* | 1.27* | ||
| BMI (kg/m2) | Underweight | 50 | 3.9 | 1 |
| Normal weight | 912 | 71.4 | ||
| Overweight | 225 | 17.6 | ||
| Obese | 91 | 7.12 | ||
| Marital situation | Live with father | 1263 | 98.7 | 0 |
| No live with father | 16 | 1.3 | ||
| Occupational status | Employed | 1002 | 78.5 | 2 |
| Unemployed | 275 | 21.5 | ||
| Diet variables | ||||
| Calories (KJ/day) | ≤2000 | 516 | 40.3 | 0 |
| > 2000 | 747 | 58.4 | ||
| Proteins (g/day) | ≤99.50 | 461 | 36.5 | 16 |
| >99.50 | 802 | 63.5 | ||
| Fat (g/day) | ≤89.5 | 726 | 57.5 | 16 |
| >89.5 | 537 | 42.5 | ||
| Carbohydrates (g/day) | ≤250.50 | 687 | 54.4 | 16 |
| >250.50 | 576 | 45.6 | ||
| Dairy products (g/day) | ≤455 | 676 | 53.5 | 16 |
| >455 | 587 | 46.5 | ||
| Red meat (g/day) | ≤53.50 | 399 | 31.6 | 16 |
| >53.50 | 864 | 68.4 | ||
| White meat (g/day) | ≤30.45 | 551 | 43.6 | 16 |
| >30.45 | 712 | 56.4 | ||
| Fish (g/day) | ≤71 | 698 | 55.3 | 16 |
| >71 | 565 | 44.7 | ||
| Cereals and pasta (g/day) | ≤90.5 | 723 | 57.2 | 16 |
| >90.5 | 540 | 42.7 | ||
| Legumes (g/day) | ≤50 | 561 | 44.4 | 16 |
| >50 | 702 | 55.6 | ||
| Potatoes (g/day) | ≤61.5 | 288 | 47.0 | 667 |
| >61.5 | 324 | 52.9 | ||
| Bread (g/day) | ≤42 | 571 | 45.2 | 16 |
| >42 | 692 | 54.8 | ||
| Supplement variables | ||||
| Supplement Vit B12 | No | 354 | 27.7 | 0 |
| Yes | 925 | 72.3 | ||
| Supplement Vit B6 | No | 888 | 69.4 | 0 |
| Yes | 391 | 30.6 | ||
| Supplement Vit D | No | 962 | 75.2 | 0 |
| Yes | 317 | 24.8 | ||
| Supplement Ca | No | 915 | 71.5 | 0 |
| Yes | 354 | 28.5 | ||
| Supplement Fe | No | 836 | 65.4 | 0 |
| Yes | 442 | 34.6 | ||
| Supplement Mg | No | 903 | 70.6 | 0 |
| Yes | 376 | 29.4 | ||
| Supplement Zn | No | 903 | 70.6 | 0 |
| Yes | 376 | 29.4 | ||
BMI: Body mass index; SD: standard deviation.
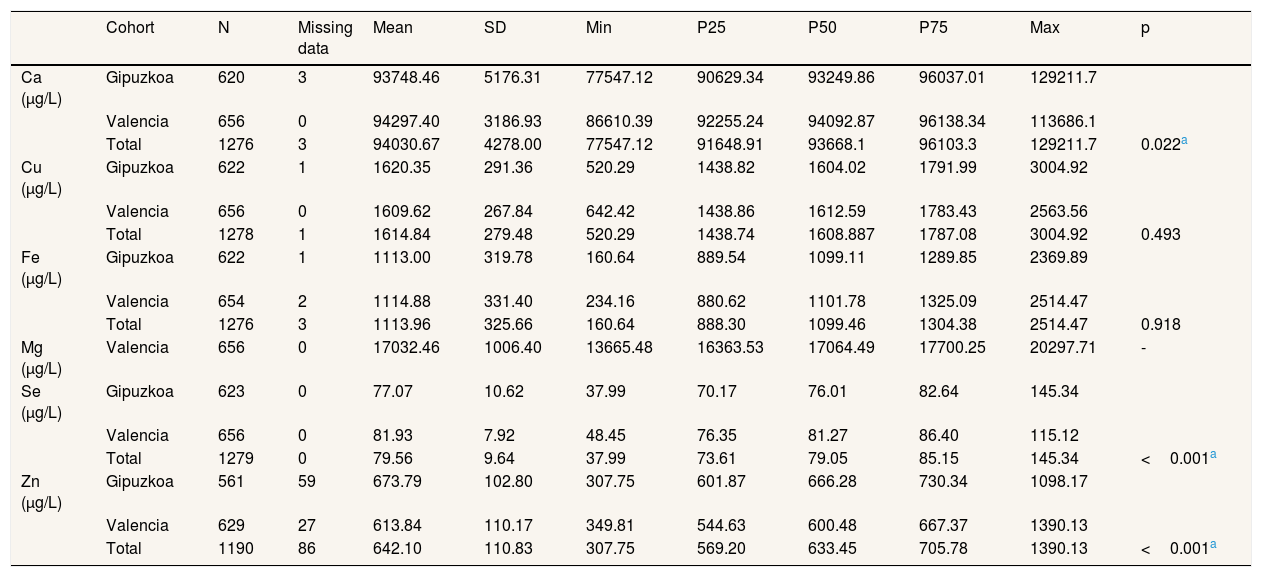
Sample size, missing data, mean, SD, minimum, maximum and percentiles (25th, 50th and 75th) for each metal are presented in Table 2 by cohort. Mean and standard deviation of the levels were 94030.7±4278.0μg/L for Ca, 1614.8±279.5μg/L for Cu, 1113.9±325.7μg/L for Fe, 17032.5±1006.4μg/L for Mg, 79.56±9.64μg/L for Se and 642.1±110.8μg/L for Zn.
Concentrations of Ca, Cu, Fe, Mg, Se and Zn (μg/L) in serum samples during the first trimester of pregnancy by cohort and the whole sample. t-test independent samples analysis.
| Cohort | N | Missing data | Mean | SD | Min | P25 | P50 | P75 | Max | p | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ca (μg/L) | Gipuzkoa | 620 | 3 | 93748.46 | 5176.31 | 77547.12 | 90629.34 | 93249.86 | 96037.01 | 129211.7 | |
| Valencia | 656 | 0 | 94297.40 | 3186.93 | 86610.39 | 92255.24 | 94092.87 | 96138.34 | 113686.1 | ||
| Total | 1276 | 3 | 94030.67 | 4278.00 | 77547.12 | 91648.91 | 93668.1 | 96103.3 | 129211.7 | 0.022a | |
| Cu (μg/L) | Gipuzkoa | 622 | 1 | 1620.35 | 291.36 | 520.29 | 1438.82 | 1604.02 | 1791.99 | 3004.92 | |
| Valencia | 656 | 0 | 1609.62 | 267.84 | 642.42 | 1438.86 | 1612.59 | 1783.43 | 2563.56 | ||
| Total | 1278 | 1 | 1614.84 | 279.48 | 520.29 | 1438.74 | 1608.887 | 1787.08 | 3004.92 | 0.493 | |
| Fe (μg/L) | Gipuzkoa | 622 | 1 | 1113.00 | 319.78 | 160.64 | 889.54 | 1099.11 | 1289.85 | 2369.89 | |
| Valencia | 654 | 2 | 1114.88 | 331.40 | 234.16 | 880.62 | 1101.78 | 1325.09 | 2514.47 | ||
| Total | 1276 | 3 | 1113.96 | 325.66 | 160.64 | 888.30 | 1099.46 | 1304.38 | 2514.47 | 0.918 | |
| Mg (μg/L) | Valencia | 656 | 0 | 17032.46 | 1006.40 | 13665.48 | 16363.53 | 17064.49 | 17700.25 | 20297.71 | - |
| Se (μg/L) | Gipuzkoa | 623 | 0 | 77.07 | 10.62 | 37.99 | 70.17 | 76.01 | 82.64 | 145.34 | |
| Valencia | 656 | 0 | 81.93 | 7.92 | 48.45 | 76.35 | 81.27 | 86.40 | 115.12 | ||
| Total | 1279 | 0 | 79.56 | 9.64 | 37.99 | 73.61 | 79.05 | 85.15 | 145.34 | <0.001a | |
| Zn (μg/L) | Gipuzkoa | 561 | 59 | 673.79 | 102.80 | 307.75 | 601.87 | 666.28 | 730.34 | 1098.17 | |
| Valencia | 629 | 27 | 613.84 | 110.17 | 349.81 | 544.63 | 600.48 | 667.37 | 1390.13 | ||
| Total | 1190 | 86 | 642.10 | 110.83 | 307.75 | 569.20 | 633.45 | 705.78 | 1390.13 | <0.001a |
P: percentile; SD: standard deviation.
Table 3 summarizes the results of multiple linear regression models for each metal. Ca levels were related to daily white meat consumption (p=0.026). Higher levels of Cu were related to excess body weight (p<0.001), low social class (p=0.003) and being multipara (p <0.001). On the other hand,lower levels of Cu were related to bread intake of less than 42g /day (p=0.013) and residence in Gipuzkoa, after adjustment for the other variables. With reference to Se, higher levels were related to residence in Valencia (p <0.001), having a university degree (p = 0.001),taking B6 vitamin supplements (p = 0.006) and a fish intake of more than 71 g/day (p = 0.008), after adjustment for the other variables. Women born outside Spain showed lower Se levels (p <0.001). In regard to Fe, lower levels were related to having excess body weight (p=0.021) or obesity (p <0.01) and taking vitamin B12 supplements (p = 0.006). Higher levels of Mg were associated with being over 35 years old (p=0.001), high social class (p=0.044), primiparous status (p=0.002) and low daily bread (p=0.009) and legume (p=0.020) intake, after adjustment for the other variables.
Linear regression model for association between levels of Ca, Cu, Se, Mg, Fe, Zn and sociodemographic and dietary variables.
| Dependent variable | Independent variables | β (95%CI) | p |
|---|---|---|---|
| Ca | Cohort (Gipuzkoa vs. Valencia) | 216.22 (−24.02; 456.61) | 0.078 |
| White meat consumption (≤30.45 g/day vs.>30.45 g/day) | 549.44 (65.40; 1033.48) | 0.026 | |
| Cu | Cohort (Gipuzkoa vs. Valencia) | −29.96 (−49.36; −10.59 | 0.002 |
| BMI (kg/m2) | |||
| 18.5-25 | - | ||
| <18.5 | −69.98 (−143.18; 11.21) | 0.094 | |
| 25<30 | 102.62 (63.26; 141.99) | <0.001 | |
| ≥35 | 170.40 (111.71; 229.08) | <0.001 | |
| Social class (no manual vs. manual) | 45.32 (15.14; 75.50) | 0.003 | |
| Parity (primipara vs. multipara) | 92.31 (62.43; 122.18) | <0.001 | |
| Bread consumption (≤42 g/day vs.>42 g/day) | −49.35 (−88.19; −10.52) | 0.013 | |
| Se | Cohort (Gipuzkoa vs. Valencia) | 4.69 (3.40; 5.98) | <0.001 |
| Country of birth (Spain vs. Other) | −3.27 (−5.17; −1.40) | 0.001 | |
| Educational level | |||
| Primary | - | ||
| Secondary | 0.99 (−0.36; 2.34) | 0.149 | |
| University | 2.29 (0.89; 3.69) | 0.001 | |
| Fish consumption (≤71 g/day vs.>71 g/day) | 1.29 (0.26; 2.33) | 0.014 | |
| B6 vitamin supplementation (no vs. yes) | 1.88 (0.54; 3.22) | 0.006 | |
| Fe | Cohort (Gipuzkoa vs. Valencia) | 31.96 (−7.08; 71.00) | 0.109 |
| BMI (kg/m2) | |||
| 18.5-25 | - | ||
| <18.5 | 56.37 (−36.17; 148.92) | 0.232 | |
| 25<30 | −55.48 (−102.72; −8.24) | 0.021 | |
| ≥35 | −143.82 (−213.61; −73.93) | <0.001 | |
| B12 vitamin supplementation (no vs. yes) | −60.93 (−104.61; −17.24) | 0.006 | |
| Mg | Age (years) | ||
| 25-29 | - | ||
| <25 | 47.95 (−320.39; 224.50) | 0.730 | |
| 30-34 | 19.35 (−164.78; 203.07) | 0.836 | |
| >35 | 423.22 (167.52; 678.93) | 0.001 | |
| Social class (no manual vs. manual) | −163.73 (−323.15; −4.31) | 0.044 | |
| Parity (primipara vs. multipara) | −256.18 (−421.60; −90.76) | 0.002 | |
| Bread consumption (≤42 g/day vs.>42 g/day) | −241.70 (−423.59; −59.82) | 0.009 | |
| Legumes consumption (≤50 g/day vs.>50 g/day) | −182.36 (−335.97; −28.76) | 0.020 | |
| Zn | Cohort (Gipuzkoa vs. Valencia) | −28.21 (−34.60; −21.82) | <0.001 |
| Age (years) | |||
| 25-29 | - | ||
| <25 | −4.89 (−31.07; 21.28) | 0.714 | |
| 30-34 | −1.46 (−15.59; 12.66) | 0.839 | |
| >35 | −20.57 (−38.80; −2.34) | 0.027 | |
| Educational level | |||
| Primary | - | ||
| Secondary | 4.35 (−11.72; 20.41) | 0.596 | |
| University | 17.85 (0.89; 34.80) | 0.039 |
BMI: body mass index; 95%CI: 95% confidence interval.
Finally, higher levels of Zn were related to having a university degree (p=0.039) and being from the Gipuzkoa cohort (p <0.001), and lower levels of Zn were related to being over 35 years old (p=0.027), after adjustment for the other variables.
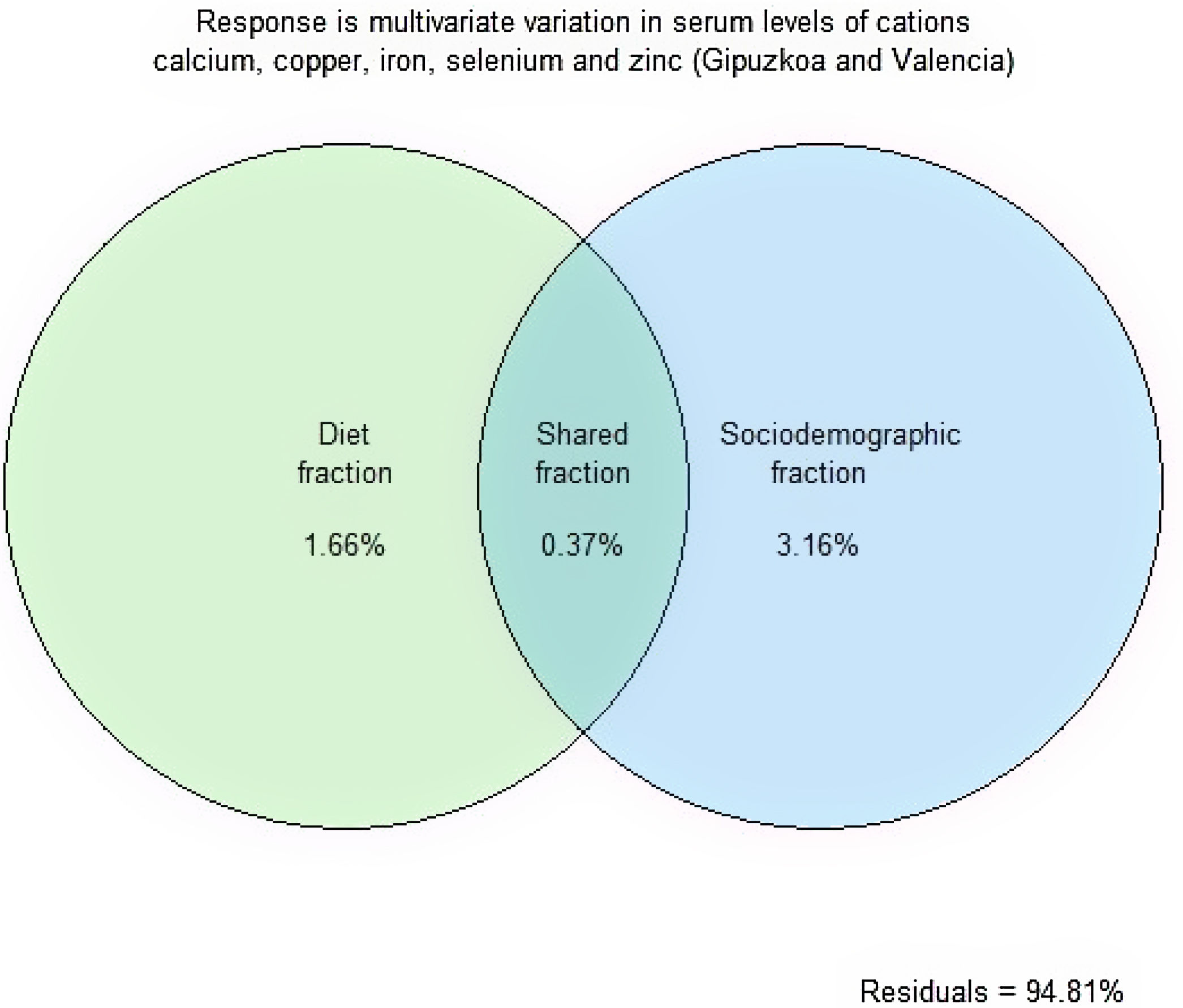
Table 4 shows that the multivariate variance in serum levels of Ca, Cu, Fe, Se and Zn was associated with body mass, parity, educational level and country of origin (socio-demographic model) and also with white bread and vitamin B6 intake (dietary model). BMI and country of origin emerge as the most important among the explanatory variables considered. Although the influence of both socio-demographic conditions and diet on serum levels appears to be rather modest, the partitioning of variance in the joint model (Fig. 1) suggests that, overall, socio-demographic conditions are more influential than diet itself. Table 5 summarizes the results of previous studies.
PERMANOVA. The response or outcome, which is constituted by multivariate variation in serum levels of Ca, Cu, Fe, Se and Zn (for both cohorts, Gipuzkoa and Valencia), is explained in terms of either a purely diet model or in terms of a purely socio-demographic model. Adjusted sums of squares and permutation-based p-values are reported.
| Variable | Df | SS | R2 | F | p |
|---|---|---|---|---|---|
| Diet model | |||||
| White bread intake | 1 | 40.3 | 0.0075 | 8.20 | 0.001 |
| Vitamin B6 intake | 1 | 33.6 | 0.0063 | 6.84 | 0.001 |
| Residual | 1069 | 5246.0 | 0.9796 | - | - |
| Total | 1071 | 5355.0 | 1.0000 | - | - |
| Socio-demographic model | |||||
| Body mass index | 1 | 61.1 | 0.0114 | 12.57 | 0.001 |
| Parity | 1 | 36.2 | 0.0068 | 7.45 | 0.001 |
| Education level | 2 | 28.4 | 0.0053 | 2.93 | 0.003 |
| Country of origin | 3 | 55.5 | 0.0104 | 3.81 | 0.001 |
| Residual | 1064 | 5166.1 | 0.9647 | - | - |
| Total | 1071 | 5355.0 | 1.0000 | - | - |

Venn diagram showing how multivariate variation in serum levels of Ca, Cu, Fe, Se and Zn was partitioned among a diet component and a socio-demographic component. Numbers are R2 values (%). The diet component includes white bread intake and vitamin B6 intake. The socio-demographic component includes body mass index, parity, education level and country of origin.
Trace elements concentrations in serum samples from women in different studies.
| Author | Year | Country | Sample size | Mean (SD) | |
|---|---|---|---|---|---|
| Ca (μg/L) | Sukonpan12 | 2005 | Thailand | 40 | 97000 (7000) |
| Ainy13 | 2006 | Iran | 48 | 92000 (6000) | |
| Punthumapol15 | 2008 | Thailand | 36 | 89900 (3100) | |
| Tong16 | 2010 | China | 90 | 21600 | |
| Kanagal14 | 2014 | India | 60 | 89700 (6900) | |
| Arun7 | 2017 | Nepal | 35 | 95900 (6200) | |
| Mg (μg/L) | Sukonpan12 | 2005 | Thailand | 40 | 20700 |
| Li19 | 2010 | China | 100 | 9800 | |
| Kanagal14 | 2014 | India | 60 | 15700 (7200) | |
| Arun7 | 2017 | Nepal | 35 | 20300 (1600) | |
| Punthumapol15 | 2008 | Thailand | 36 | 20400 (1900) | |
| Cu (μg/L) | Awadallah21 | 2004 | Jordan | 52 | 1750 (420) |
| Zhang23 | 2013 | China | 2380 | 1026 | |
| Jariwala20 | 2014 | India | 42 | 1614 (295) | |
| Choi22 | 2016 | Korea | 245 | 1650 | |
| Polanska24 | 2017 | Poland | 539 | 1980 (570) | |
| Zn (μg/L) | Awadallah21 | 2004 | Jordan | 52 | 770 (160) |
| Izquierdo26 | 2007 | Spain | 159 | 654 (12.9) | |
| Zhang23 | 2013 | China | 2380 | 920 | |
| Jariwala20 | 2014 | India | 42 | 514 (149) | |
| Shen28 | 2015 | China | 1447 | 900 | |
| Choi22 | 2016 | Korea | 245 | 570 | |
| Khoushabi27 | 2016 | Iran | 60 | 749 | |
| Polanska24 | 2017 | Poland | 539 | 910 (270) | |
| Liu34 | 2017 | China | 1400 | 740 | |
| Fe (μg/L) | Awadallah21 | 2004 | Jordan | 52 | 690 (260) |
| Zhang23 | 2013 | China | 2380 | 900 | |
| Jariwala20 | 2014 | India | 42 | 1132 (519) | |
| Shen28 | 2015 | China | 1447 | 800 | |
| Khoushabi27 | 2016 | Iran | 60 | 744 | |
| Liu34 | 2017 | China | 1400 | 1315 | |
| Se (μg/L) | Kantola31 | 2004 | Finland | 216 | 81 (27) |
| Izquierdo26 | 2007 | Spain | 159 | 99.59 (21.7) | |
| Ejezie32 | 2012 | Nigeria | 120 | 112.3 | |
| Jariwala20 | 2014 | India | 42 | 70 (15) | |
| Choi22 | 2016 | Korea | 245 | 94 | |
| Liu34 | 2017 | China | 1400 | 77.6 |
SD: standard deviation.
We analyzed trace element levels in pregnant women in their first trimester of pregnancy. Our results reveal that the main variables related to these levels are BMI, social class and cohort. According to Abbassi-Ghanavati et al.11, serum Ca between 88,000μg/L and 106,000μg/L can be considered normal and our results fall within this range (94,030.7μg/L). Further, the Ca levels in our sample of pregnant women are in line with those observed in several previous studies7,12,13 (with values of 95,900μg/L, 97,000μg/L and 92,000μg/L respectively). On the other hand, they are a little higher than those obtained by Kanagal et al.14 (89,700μg/L), and Punthumapol and Kittichotpanich15 (89,900μg/L), and much higher than those found in a study carried out in China by Tong16 (21,600μg/L). Some studies have shown Ca levels to be related to body weight, levels being significantly lower in those with excess body weight,17,18 but we did not find any such relationship in our study. Regarding age, unlike other authors,18 we found an association close to statistical significance, levels decreasing with increasing age (p=0.077).
Regarding Mg, our results (17,000μg/L) are within the normal range for Mg of between 16,000μg/L and 22,000μg/L11. The levels we observed were similar to those reported by Kanagal et al.14 (15,700μg/L) and slightly lower than those observed by Punthumapol and Kittichotpanich15 (20,400μg/L), Arun et al.7 (20,300μg/L) and Sukonpan and Phupong12 (20,700μg/L). In contrast, a study carried out in China by Li19, showed levels of serum Mg well below those obtained in this study (9800μg/L).
The mean Cu level in our study population (1615μg/L) was within the normal range of between 1120μg/L and 1990μg/L11. Similar levels have been observed in other studies20–22 (1614μg/L, and 1650μg/L and 1750μg/L, respectively). On the other hand, Cu levels considerably different from ours have been observed in China23 and in Poland24 (1026μg/L and 1980μg/L, respectively). Wilson et al.25 reported significantly higher levels in obese women than underweight, normal weight or overweight women, as in our study. We found a trend related to BMI (with the highest levels in obese women), while others have observed an opposite trend.17
Again, in the case of Zn, the levels we observed (642μg/L) lie within the normal range of between 570μg/L and 880μg/L.11 These results were in agreement with those found in previous studies in Spain26 and Iran27 (654μg/L and 749μg/L, respectively). Studies carried out in China23,28 and Poland24 showed higher levels (920μg/L, 900μg/L and 910μg/L, respectively), while studies carried out in Korea22 and India20 showed lower levels (570μg/L and 514μg/L respectively). We found an association between Zn and educational level, which could be an indicator of social class. Nevertheless, other authors did not find this pattern29.
As for Se, our results were consistent with studies carried out in Spain30 and Finland31 with reported values of 81μg/L, while a study from India20 found lower values of 70μg/L. On the other hand, higher values were found in Korea,22 Spain26 and Africa32 (94μg/L, 99.59μg/L and 112.3μg/L, respectively). In our study, Se levels appear to be related to fish consumption, which is consistent with other research findings.33
Fe levels between 720μg/L and 1430μg/L can be considered normal,11 and our results are in that range (1114μg/L). Similar results have been reported in China23 and India20 (900μg/L and 1132μg/L respectively), while some studies have shown slightly lower values21,27,28 (690μg/L, 800μg/L and 744μg/L respectively), and another study in China,34 found values slightly higher than ours (1500μg/L). We observed that being overweight or obese was associated with significantly lower serum Fe levels, a pattern that has been observed previously15,25.
Social inequalities in dietary habits have been widely described and indicate that the lowest social classes tend to have less balanced and less healthy diets. Pregnant women with lower social status have fewer healthy habits, including a less healthy diet, more harmful behaviors, and poorer monitoring during pregnancy. Indeed, the role of education as a social determinant of diet has been confirmed by several authors as the most robust independent predictor of healthy dietary habits.35
The strengths of the study are the sample size (n=1279) and the fact that we gathered data on and adjusted models for a large number of factors in the first trimester, especially socio-demographic characteristics. Regarding its limitations, the descriptive and cross-sectional character of the design means that we cannot ascertain causality in the associations observed, measurements were taken at only one point during pregnancy, and the spectroscopy measurements of the metals were element-specific not species-specific. Another limitation is that the information regarding some of the behavioral variables (smoking and alcohol consumption) was self-reported, an approach which may underestimate the prevalence of socially disapproved behaviors.
ConclusionsOur results indicate that the Ca, Cu, Se, Fe, Mg and Zn levels in both cohorts were adequate and within the ranges considered normal for pregnant women. More than half of the sample did not take supplements, except in the case of vitamin B12 (72%). Among the variables considered, those with the best explanatory value of the levels of these trace elements were anthropometric and socio-demographic variables and within these, BMI, social class, educational level and cohort. This study will serve as a basis for future research, in particular, to identify trends in these elements through pregnancy and their possible relationship with the later development of the child.
Poor nutritional status is known to carry a higher risk of disease. This risk is greater during pregnancy since not only maternal health is at stake, but also the proper development of the fetus. Therefore the establishment and knowledge of reference values is of vital importance.
What does this study add to the literature?This study provides relevant data on serum metal levels in pregnant women and their relationship with socio-demographic and anthropometric characteristics, supplementation during pregnancy and diet. The follow-up of clinical variables during pregnancy and the knowledge of socio-demographic conditions, supplementation, vitamins, minerals and diet of pregnant women are vital to ensure adequate care during pregnancy. This article will serve as a basis for future work assessing the evolution of these trace elements throughout pregnancy in order to improve perinatal outcomes and subsequent child development.
What are the implications of the results?It is necessary to implement measures to intervene in healthy lifestyles (healthy diet, not smoking, avoiding a sedentary lifestyle, etc.) as well as care and attention during pregnancy. A balanced diet must be sufficient to cover the needs in a way that it contains all nutrients (proteins, carbohydrates, fats, vitamins and minerals) in adequate amounts. The requirements of minerals (Ca, Cu, Fe, Mg, Zn, Se, etc.) and vitamin (B12) are adequately covered by the consumption of raw fruit and vegetables, whole grains, raw olive oil and dairy products. On the other hand, it may be advisable to pay special attention to pregnant women with excess weight in relation to Fe control, as well as vitamin B12 supplementation.
Fish consumption, avoiding the most mercury-contaminated species (swordfish, shark, bluefin tuna), has a beneficial effect on health due to its high content in proteins of great nutritional value, omega-3 fatty acids, vitamin D and antioxidant substances (including Se). Considering that the variability of all these elements is mainly associated with socio-demographic and anthropometric variables, it is necessary to promote healthy habits and lifestyles, as well as self-care during pregnancy.
Juan Alguacil.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsStudy design: M. Begoña Zubero, S. Llop, M. Murcia, A. Molinuevo, F. Ballester, M. Levi, M. Lozano, L. Santa-Marina.
Methodology: M. Begoña Zubero, L. Santa-Marina.
Literature review: S. Llop, A. Irizar, F. Ballester, M. Levi, M. Lozano, M. Ayerdi.
Data collection and clean-up: A. Irizar, M. Ayerdi.
Data analysis and interpretation: M. Begoña Zubero, M. Murcia, A. Molinuevo.
Writing the article: M. Begoña Zubero, S. Llop, F. Ballester, M. Levi, M. Lozano, L. Santa-Marina.
Analysis and critical review: A. Irizar, M. Murcia, A. Molinuevo, M. Ayerdi.
Final version approval: M.B. Zubero, S. Llop, A. Irizar, M. Murcia, A. Molinuevo, F. Ballester, M. Levi, M. Lozano, M. Ayerdi, L. Santa-Marina.
AcknowledgementsWe want to acknowledge all the INMA families for their altruistic participation in the study, without which it would have not been possible to carry out this work. We also wanted to thank Nerea Urbieta for her contribution to the work.
FundingThis study is part of the INMA (Infancia y Medio Ambiente) project. It was supported by grants from Instituto de Salud Carlos III (FIS-FEDER: 06/0867, 09/00090, 13/1944, 16/1288, 19/1338; Miguel Servet- FEDER: CP15/0025; Miguel Servet-FSE: MS15/0025), by the Council of Gipuzkoa (DFG15/009) and by the Health Department of the Basque Government.
Conflicts of interestWe wish to confirm that there are no known conflicts of interest associated with this publication that could have influenced its outcome.













