



The 1st International Conference on Safety and Public Health
Más datosTo identify the risk factor of Stroke in health institution employees.
MethodThe research design was cross-sectional with 107 people who participated in this survey using purposive sampling method.
ResultsThe relationship between family history with the incidence of stroke obtained p value (p<0.05), the relationship between smoking habits with the incidence of stroke p value=0.012 (p<0.05), the relationship between lack of physical activity with the incidence of stroke obtained p=0.476 (p> 0.05), lack of consumption of fruits and vegetables obtained a value of p=0.091 (p>0.05) and alcohol consumption with the incidence of stroke obtained a value of p=0.616 (p> 0.05).
ConclusionsRelationship between family history, smoking habits with the incidence of stroke.
Stroke is a non-infectious disease that causes the first disability and second death in the world.1 Based on WHO data, stroke victims number 15 million in the world with a total of 5 million deaths and 5 million others experience permanent disabilities each year.2,3 Stroke is a cerebrovascular disease that is found not only in developed and developing countries. Stroke has get single of the greatest origins of disability in western nations. The incidence of stroke in the Netherlands ranks third as the cause of DALY's (disability adjusted life years).4
The number of stroke sufferers is greater in developing countries in Asia compared to developed countries. The incidence of stroke in China reaches 1.5–2 million people each year. Ischemic stroke is the near common case of stroke and the factors that influence it are genetic factors, environmental factors, and their relationship.5 The incidence of stroke in Indonesia reaches 500,000 people per year, including 125,000 people (2.5%) die and the rest are mildly or severely disabled. Ischemic stroke is around 80% of all stroke cases, while the incidence of hemorrhagic stroke is only about 20% of all stroke case.6,7 In Indonesia, The prevalence of stroke has expanded by 8.3/1000 population in 2007 to 12.1/1000 population in 2013.8
Increased body mass and the number of risk will increase the potential for the occurrence of stroke. Modifiable risk factors for stroke include a history of stroke, hypertension, heart disease, diabetes mellitus, asymptomatic carotid disease, transient ischemic attack, hypercholesterolemia, oral contraceptive use, narcotic use, antiphospholipid antibodies, obesity, smoking, alcoholics, hyperuricemia, increased hematocrit. While the factors that cannot be modified are age, sex, heredity, and race/ethics.9
MethodThis was a cross-sectional approach in South Sulawesi, Indonesia. This research is a quantitative analytic study designed with a cross sectional approach. The results of medical examinations in the Health Service EXPO Event South Sulawesi 2018 were used as secondary data in this study. The population in this study were employees of the municipal/district health office totaling 126 people. A total of 107 people on the health check form and fulfilling the inclusion criteria were sampled in this study. Secondary data was obtained from the results of a health examination conducted at communicable disease POSBINDU during the Health Service EXPO Event.
Data collected in this study include data on age, sex, family history of illness, history of self-illness, smoking history, physical activity, consumption of vegetables and fruit, and alcohol consumption. Data analysis conducted in this research is univariate analysis and bivariate analysis. This study used univariate analysis to specify the frequency of data processing, namely age, sex, history of stroke, family history of illness, physical activity, utilization of vegetables and fruits, alcohol consumption, and smoking habits. While the bivariate analysis was carried out to determine the relationship of two variables namely the dependent variable and the independent variable by using parametric test analysis namely Pearson correlation analysis with the SPSS program.
ResultsResults are research findings in the form of data (tables and figures) from observations. The results should be clear and concise (Table 1).
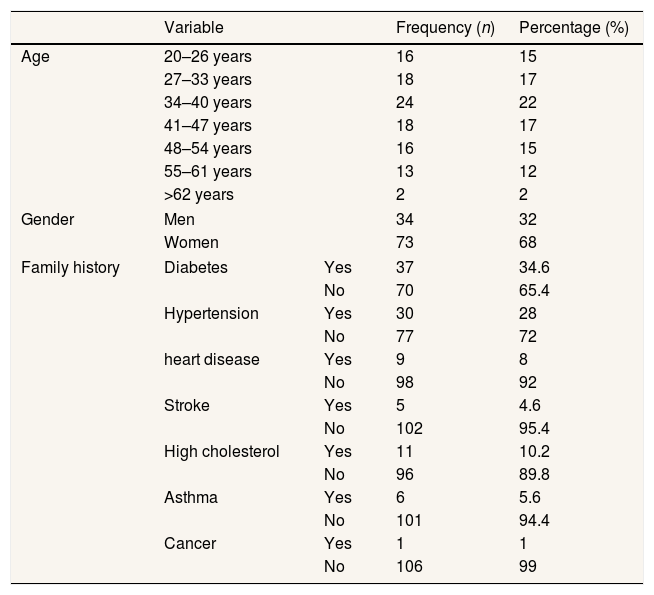
Proportion of risk factor for stroke incidence.
| Variable | Frequency (n) | Percentage (%) | ||
|---|---|---|---|---|
| Age | 20–26 years | 16 | 15 | |
| 27–33 years | 18 | 17 | ||
| 34–40 years | 24 | 22 | ||
| 41–47 years | 18 | 17 | ||
| 48–54 years | 16 | 15 | ||
| 55–61 years | 13 | 12 | ||
| >62 years | 2 | 2 | ||
| Gender | Men | 34 | 32 | |
| Women | 73 | 68 | ||
| Family history | Diabetes | Yes | 37 | 34.6 |
| No | 70 | 65.4 | ||
| Hypertension | Yes | 30 | 28 | |
| No | 77 | 72 | ||
| heart disease | Yes | 9 | 8 | |
| No | 98 | 92 | ||
| Stroke | Yes | 5 | 4.6 | |
| No | 102 | 95.4 | ||
| High cholesterol | Yes | 11 | 10.2 | |
| No | 96 | 89.8 | ||
| Asthma | Yes | 6 | 5.6 | |
| No | 101 | 94.4 | ||
| Cancer | Yes | 1 | 1 | |
| No | 106 | 99 | ||
Source: Secondary Data, 2018.
The subjects were employees in health institution. Most of the participant (22%) were in the 34–40 years age category. The major (68%) of participant are female. Most of them without family history of disease.
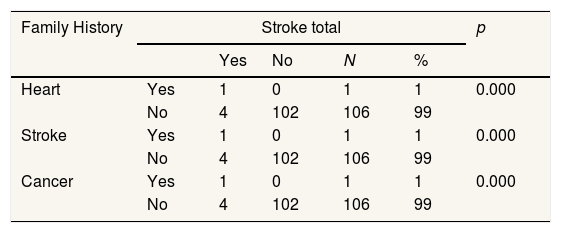
Based on Table 2, there is a relationship between heart disease in the family and the incidence of stroke (p=0.000). There is a related between stroke in the family and the incidence of stroke (p=0.000). For cancer (p=0.000) was significantly associated between cancer in the family and the occurrence of stroke.
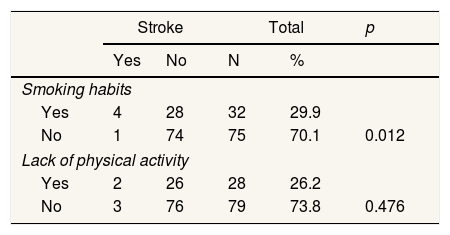
According to Table 3, there is a related between smoking habits and stroke incidence (p=0.012). There is no related between lack of physical activity and the incidence of stroke (p=0.476) in health agency employees who conduct examinations at non communicable disease POSBINDU Health Service EXPO Event.
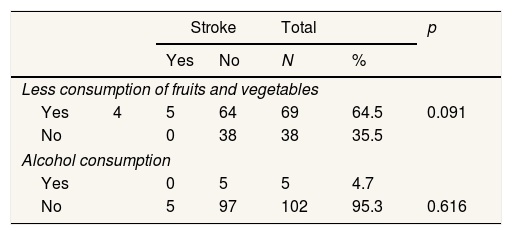
According to Table 4, there is no statistically significant difference in the lack of consumption of vegetables and fruit with the incidence of stroke (p=0.091). There is no relationship between alcohol consumption and the incidence of stroke among employees of health agencies who conduct examinations at noncommunicable disease POSBINDU Health Service EXPO Event (p=0.616).
Analysis of the relationship between fruits, vegetables and alcohol consumption with the Stroke incidene.
| Stroke | Total | p | ||||
|---|---|---|---|---|---|---|
| Yes | No | N | % | |||
| Less consumption of fruits and vegetables | ||||||
| Yes | 4 | 5 | 64 | 69 | 64.5 | 0.091 |
| No | 0 | 38 | 38 | 35.5 | ||
| Alcohol consumption | ||||||
| Yes | 0 | 5 | 5 | 4.7 | ||
| No | 5 | 97 | 102 | 95.3 | 0.616 | |
Source: Secondary Data, 2018.
The risk of stroke for heredity, experts say that there is a recessive gene that affects it. The gene is associated with diseases that are risk factors for stroke. Diseases associated with these genes include diabetes, hypertension, hyperuricemia, hyperlipidemia, coronary heart disease, and abnormalities in blood vessels that are hereditary. the testing using a bivariate analysis of family history based on study (history of heart disease, stroke, and family history with cancer) result a significant related with the incidence of stroke among health agency employees who carry out checks at noncommunicable diseases POSBINDU Health Service EXPO Event. This finding was consistent with previous studies that a family history of stroke is one of the risk factors for stroke complications. Our finding was consistent with previous studies that a family history of stroke is one of the risk factors for stroke complications. The risk of suffering from an ischemic stroke increased two times more in 500 women aged 18–44 years with a family history of stroke.10
A family disease history of diabetes, asthma, hypertension, and cholesterol are no significant relationship in stroke incidence. Family history is one of the potential risk factors associated with stroke incidence. However, family history is not an independent risk factor that causes a stroke. This dominant study did not have a significant related between family disease history of illness and the stroke incidence. Increased risk of stroke in family history (heredity) is obtained through several mechanisms, namely genetic factors, genetic sensitivity, cultural/environmental factors, and lifestyle as well as interactions between genetic and environmental factors.11
Smoking habitsSmoking is one of the main causes of heart problem and stroke. The incidence of stroke will increase when combined with other risk factors, especially hypertension. This study is following with research published by Aliah in Yogyakarta, it shows smoking is significantly related to the incidence of stroke and smokers are at 4.51 times the risk of stroke compared to nonsmokers (p=0.000; OR=4.51; 95% CI=2.107–9669).12 Other studies state that the risk of stroke will increase by about 2–3 times in smokers compared to nonsmokers and will only disappear after stopping smoking for 5–10 years.13
Lack of physical activityThis study shows that there is no significant related between less physical activity and the incidence of stroke. Different findings were obtained by Perawaty (2014) which states that people who have less physical activity have a risk of 3.46 times greater stroke than those who have lots of physical activity.14 WHO report which explains that a sedentary lifestyle or physical inactivity is the main cause of death and disease. Physical activities such as sports carried out with the principle of FIT (frequency, intensity, and time) can minimize the risk of death from heart problems and stroke, help prevent and reduce hypertension, and can control the risk of obesity by up to 50%.2 Research on stroke risk factors in American blacks reports that low physical activity has the potential to be a contributing factor to stroke incidence and is obtained RR: 2.07; 95%; CI: 1.25–3.43.15
Less consumption of fruits and vegetablesThe results of this study pointed that that there was no relationship significantly between consuming fewer fruits and vegetables with stroke incidence among health agency workers who examined at noncommunicable disease POSBINDU Health Service EXPO Event. In contrast to previous studies in Japan, fruits and also green and yellow vegetable associates with the risk of death from stroke in men and women. Eating vegetables and fruits reduces the potential of stroke by 20–40% in both women and men.16
Vegetables and fruits contain various nutrients including vitamins, minor minerals, fiber, and various biologically active components. This component is known as phytochemicals which have complementary and (complementary) mechanisms in antioxidant activity, reduce thrombotic aggregation, alter cholesterol metabolism, and reduce blood pressure.17
Alcohol consumptionThe results of this research are in accordance with previous study that examining the risk factors for stroke in the black race of America and the result is that the consumption of alcohol in small amounts in the acute or chronic categories after being controlled by smoking and hypertension factors showed no significant relationship, OR: 1.68; 95%; CI: 0.84–3.35.15 Another study conducted in Japan which states that there is a difference in the risk of stroke between drinkers every week and those who only consume alcohol occasionally.18 This study is also in accordance with a cohort study conducted on 38,156 men in health professions in the United States. It is found that individuals who consume large amounts of alcohol and more than 2 times/day is a main factor in the occurrence of ischemic stroke.19
In one of the hadiths, the Messenger of Allah explained that there is no better favor after the true belief except healthy favors (al-fityah). Therefore, he always advised his friends to multiply one of the best prayers, namely to always be given forgiveness (al-’afw) and safety (al-’afiyah) from all kinds of dangers, including illness, both physical and mental illness.20
ConclusionsBased on 11 independent variables studied, 4 variables were found that had a relationship significantly with stroke incidence. There is a relationship between family history (heart, stroke, cancer) with stroke incidence. Smoking habits with the incidence of stroke have a significant relationship. There is no relationship between, consumption of vegetables and fruit, physical activity, and consumption of alcohol, with the incidence of stroke.
Suggestions for similar research, which need to be improved in the measurement instrument (questionnaire). Because of the weaknesses in this study, there are several risk factors that are not in accordance with the calculation standards, such as consumption of fruits and vegetables that are not measured based on 24-h food recall and physical activity measurements that are not according to WHO standards.
Conflicts of interestsThe authors declare that they have no conflict of interest.
Peer-review under responsibility of the scientific committee of the 1st International Conference on Safety and Public Health (ICOS-PH 2020). Full-text and the content of it is under responsibility of authors of the article.











