



To determine the association between caries, body mass index (BMI) and social class in child population of the Valencia region (Spain) at 6, 12 and 15 years, and study.
MethodsIn a cross sectional study of 1326 children aged 6 (n=488), 12 (n=409) and 15 years (n=433) who took part in the 2010 Oral Health Survey of the Valencia region, the ICDAS II criteria were employed for diagnosing and coding all the teeth examined. The quantitative BMI values on a continuous scale were grouped into 3 categories (normal weight, overweight, obese) based on a table adjusted for age and gender. The highest-ranking occupation of the parents was taken to indicate the social class of the child.
ResultsThe mean BMI was 17.21 at 6 years, 21.39 at 12 years and 22.38 at 15 years. No significant differences in caries indexes (DMFT or dft) by degree of obesity stratified by social class were found in any of the age groups studied. There was no significant correlation between BMI and DMFT-dft in any of the age groups.
ConclusionsObesity is not associated with dental caries in schoolchildren of this population
Determinar la asociación entre la caries, el índice de masa corporal (IMC) y la clase social en la población infantil de la Comunidad Valenciana (España) a los 6, 12 y 15 años de edad.
MétodoSe realizó un estudio transversal con una muestra de 1326 niños/as de 6 años (n=488), 12 años (n=409) y 15 años (n=433) de edad. Se emplearon los criterios del ICDAS II para el diagnóstico y la codificación de todos los dientes examinados. Los valores cuantitativos del IMC se agruparon en tres categorías (peso normal, sobrepeso y obesidad) según una tabla ajustada por edad y sexo. Para determinar la clase social se consideró la ocupación de mayor nivel de los padres.
ResultadosLa media del IMC fue de 17,21 a los 6 años, de 21,39 a los 12 años y de 22,38 a los 15 años. No se observaron diferencias significativas en los índices de caries (DMFT o dft) por grado de obesidad y estratificado según clase social en ninguno de los grupos de edad. No hubo correlación significativa entre el IMC y el DMFT-dft en ninguno de los grupos.
ConclusionesLa obesidad no está asociada con la caries dental en los niños y las niñas de la muestra estudiada.
In recent decades, changes in lifestyle and diet have been accelerated by industrialization, urbanization, economic development and market globalization. Their impact on health and nutrition has been significant, notably through higher carbohydrate intake and lower physical activity levels, particularly among the younger members of the population. As a result, the prevalence of child obesity has shot up throughout the world and has become a serious public health problem with grave consequences.1 A high body mass index (BMI) is a complex metabolic condition involving behavioral, environmental and genetic components.2 Previous studies have shown a positive association between dental caries and BMI. Overweight or obese children have a greater likelihood of suffering dental caries than those of normal weight.3,4 The relationship between dental caries and body weight is such that dietary interventions designed to reduce the incidence of dental caries may also reduce the development and persistence of excess weight.5
Other factors that might influence the association between caries and obesity, such as social class, have also been studied. When both obesity and poverty are present, caries levels may rise.6
Caries and obesity are multi-faceted conditions, influenced by a diversity of factors: psychosocial, behavioral and genetic aspects, eating habits, educational level and social class all play a part.2,7–10 Furthermore, sugar intake is a decisive factor for both.11 The challenge in studying this association lies in measuring the confounders or effect modifiers (diet, socioeconomic status, age, and so on) fully and in a standardized manner.12,13 Tooth decay causes in the human dentition irreversible destruction with masticatories implications and other related quality of life. Preventing tooth decay in children ages remains a priority in public health in industrialized countries.14
The aim of this study was to analyze the relationship between caries, body mass index (BMI) and social class in 6, 12 and 15-year-old children of the Valencia region (Spain).
MethodsStudy design and study groupThis was a cross-sectional study. The 6, 12 and 15-year-old child population of the Valencia region of Spain comprises around 40,000 children in each age group, who attend 1200 primary and secondary schools. To measure their BMI to a level of precision of 0.04 with an estimated standard deviation in the mean BMI of around 3 or 4 depending on the age group, at a 95% confidence level, it was estimated that the minimum sample size should be 400 children from each age group. Cluster sampling was provided by the public health authority of Valencia. From 1200 schools in the region, 79 clusters were selected at random, with between 15 and 20 children in each. The sample size was 1326. Of these children, 484 were 6 years old, 409 were 12 years old and 433 were 15 years old.
Clinical examinationThe three examiners were calibrated for ICDAS II caries criteria. First they carried out a calibration online (https://www.icdas.org/icdas-e-learning-course), then they performed an exercise with 10 children. The reliability of their measurements was assessed by reference to a gold standard (an experienced examiner). The weighted Kappa values of the 3 examiners all exceeded 0.85.
The World Health Organization (WHO) recommendations were followed during the clinical examinations in the schools. A 60W lamp was used as the light source. The intraoral examinations were performed with a no. 5 plain mouth mirror and a WHO type periodontal probe, both sterilized. They were carried out in November and December 2010.15
Parental consentPermission to conduct the study was obtained from the school authorities and from the head teachers of the schools involved. Signed informed consent to examine the children and to obtain information was also obtained from the parents of the children prior to the oral health examination. The study was approved by the Human Research Ethical Committee of the University of Valencia (approval #H1352114553202) and complied with the recommendations of the Declaration of Helsinki.
CariesThe ICDAS II criteria were employed for diagnosing and coding all the teeth examined.16 The ICDAS II codes classify each decayed tooth in 6 stages of caries, ranging from sound (code 0) to extensive cavity with visible dentin (code 6).
The outcome quantitative variables of caries indexes considered in temporary dentition at 6 years of age were:
- •
d1–6 ft: decayed codes ICDAS II 1 to 6 and filled teeth count.
- •
d4–6 ft: decayed codes ICDAS II 4 to 6 and filled teeth count.
The outcome quantitative variables of caries indexes considered in permanent dentition at 12 and 15 years were:
- •
D1–6 MFT: decayed codes ICDAS II 1 to 6, missing and filled teeth count.
- •
D4–6 MFT: decayed codes ICDAS II 4 to 6, missing and filled teeth count.
To measure the BMI, the height and weight of each child were recorded at the same time of the clinical examination. The BMI was calculated by dividing the weight in kilograms by the height in meters squared: BMI=weight (kg)/height (m)2. The measurements were performed by three examiners previously trained with the completion of weighing and calculation of BMI with a standardized procedure. The children wore lightweight clothes and no footwear while being weighed. Two consecutive weightings were made and a weighted average was recorded. Height was also measured without footwear. The instruments used were a SECA Robusta 813® weighing scale and a height measuring rod from the same manufacturer. BMI was expressed as quantitative variable and also the BMI values on a continuous scale were grouped into 3 categories–taking the percentiles 85 and 97 as indicative of overweight and obesity respectively (http://www.who.int/growthref/who2007_bmi_for_age/en/).
Social classIn addition to age and gender, information was obtained on social status, using the classification based on parental occupation validated in Spain.17 The highest-ranking occupation of the parents was taken to indicate the social class of the child. The classifications were:
I: professionals, senior management and senior technical grades.
II: other executives, middle-level technical grades, small employers and self-employed without higher education.
III: middle management.
IVa: skilled manual workers.
IVb: partly-skilled manual workers.
V: unskilled workers.
The social classes were recoded, classifying classes I and II as high social class, class III as middle class and classes IVa. IVb and V as low social class.
Statistical analysisThe data were analyzed with the SPSS 22.0® statistics application. Descriptive statistics with means and 95% confidence intervals were calculated for quantitative variables: BMI and caries indexes. Student's t-test, ANOVA and linear trend test were used to study differences between means in bivariate statistics. The Pearson correlation coefficient was used to test for linear relationships between quantitative variables. The significance level was set at p <0.05. Prior to the use of means comparison tests, the normal distribution was tested by the Kolmogorov-Smirnov test.
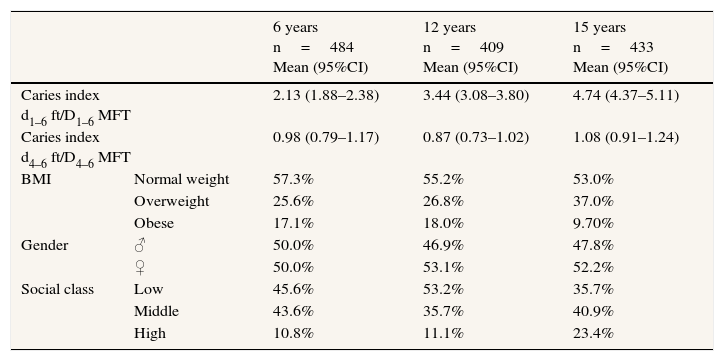
ResultsThe schoolchildren examined numbered 1326: 484 aged 6 years (242 boys and 242 girls), 409 aged 12 years (193 boys and 216 girls) and 433 aged 15 years (207 and 226 respectively). By social class, 42.5% were of low social class, 37.7% middle class and 14.5% upper class. By weight categories, 50.8% were of normal weight, 30.9% overweight and 18.3% obese. The mean body mass index (BMI) was 17.21 (17.02–17.48) at 6 years, 21.39 (21.01–21.79) at 12 years and 22.38 (22.08–22.69) at 15 years.
Table 1 shows the distribution by age of caries (dft/DMFT), BMI, gender and social class within the sample.
Caries indexes, body mass index, gender and social class by age (6, 12 and 15 years).
| 6 years n=484 Mean (95%CI) | 12 years n=409 Mean (95%CI) | 15 years n=433 Mean (95%CI) | ||
|---|---|---|---|---|
| Caries index d1–6 ft/D1–6 MFT | 2.13 (1.88–2.38) | 3.44 (3.08–3.80) | 4.74 (4.37–5.11) | |
| Caries index d4–6 ft/D4–6 MFT | 0.98 (0.79–1.17) | 0.87 (0.73–1.02) | 1.08 (0.91–1.24) | |
| BMI | Normal weight | 57.3% | 55.2% | 53.0% |
| Overweight | 25.6% | 26.8% | 37.0% | |
| Obese | 17.1% | 18.0% | 9.70% | |
| Gender | ♂ | 50.0% | 46.9% | 47.8% |
| ♀ | 50.0% | 53.1% | 52.2% | |
| Social class | Low | 45.6% | 53.2% | 35.7% |
| Middle | 43.6% | 35.7% | 40.9% | |
| High | 10.8% | 11.1% | 23.4% | |
95%CI: confidence interval of 95%; BMI: body mass index.
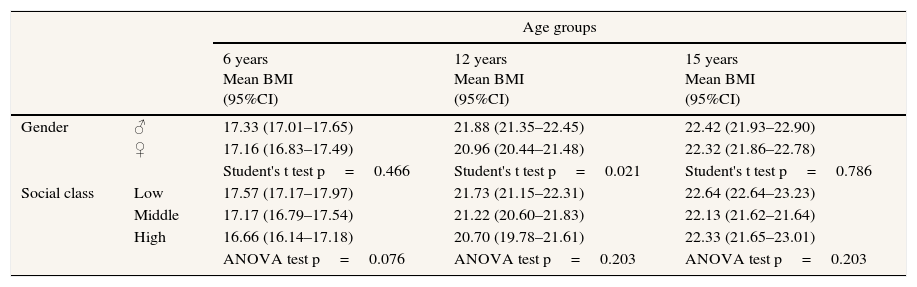
Table 2 shows the BMI distribution by gender and social class. No significant differences in BMI by social class were found at any of the three ages.
Distribution of body mass index by gender and social class.
| Age groups | ||||
|---|---|---|---|---|
| 6 years Mean BMI (95%CI) | 12 years Mean BMI (95%CI) | 15 years Mean BMI (95%CI) | ||
| Gender | ♂ | 17.33 (17.01–17.65) | 21.88 (21.35–22.45) | 22.42 (21.93–22.90) |
| ♀ | 17.16 (16.83–17.49) | 20.96 (20.44–21.48) | 22.32 (21.86–22.78) | |
| Student's t test p=0.466 | Student's t test p=0.021 | Student's t test p=0.786 | ||
| Social class | Low | 17.57 (17.17–17.97) | 21.73 (21.15–22.31) | 22.64 (22.64–23.23) |
| Middle | 17.17 (16.79–17.54) | 21.22 (20.60–21.83) | 22.13 (21.62–21.64) | |
| High | 16.66 (16.14–17.18) | 20.70 (19.78–21.61) | 22.33 (21.65–23.01) | |
| ANOVA test p=0.076 | ANOVA test p=0.203 | ANOVA test p=0.203 | ||
95%CI: confidence interval of 95%; BMI: body mass index.
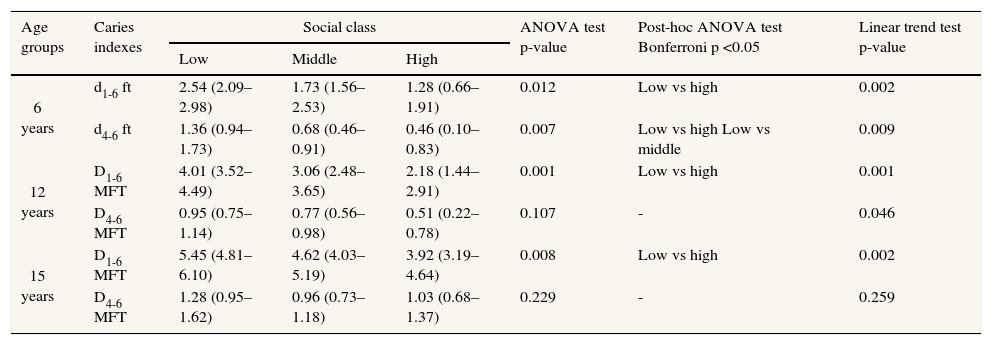
Significant differences and linear trends in caries indexes by social class were found in the three age groups studied. These differences were found among lower social class groups against high social class. A clear linear relationship between worsening social class and increased tooth decay was observed (Table 3).
Distribution of caries indexes by social class.
| Age groups | Caries indexes | Social class | ANOVA test p-value | Post-hoc ANOVA test Bonferroni p <0.05 | Linear trend test p-value | ||
|---|---|---|---|---|---|---|---|
| Low | Middle | High | |||||
| 6 years | d1-6 ft | 2.54 (2.09–2.98) | 1.73 (1.56–2.53) | 1.28 (0.66–1.91) | 0.012 | Low vs high | 0.002 |
| d4-6 ft | 1.36 (0.94–1.73) | 0.68 (0.46–0.91) | 0.46 (0.10–0.83) | 0.007 | Low vs high Low vs middle | 0.009 | |
| 12 years | D1-6 MFT | 4.01 (3.52–4.49) | 3.06 (2.48–3.65) | 2.18 (1.44–2.91) | 0.001 | Low vs high | 0.001 |
| D4-6 MFT | 0.95 (0.75–1.14) | 0.77 (0.56–0.98) | 0.51 (0.22–0.78) | 0.107 | - | 0.046 | |
| 15 years | D1-6 MFT | 5.45 (4.81–6.10) | 4.62 (4.03–5.19) | 3.92 (3.19–4.64) | 0.008 | Low vs high | 0.002 |
| D4-6 MFT | 1.28 (0.95–1.62) | 0.96 (0.73–1.18) | 1.03 (0.68–1.37) | 0.229 | - | 0.259 | |
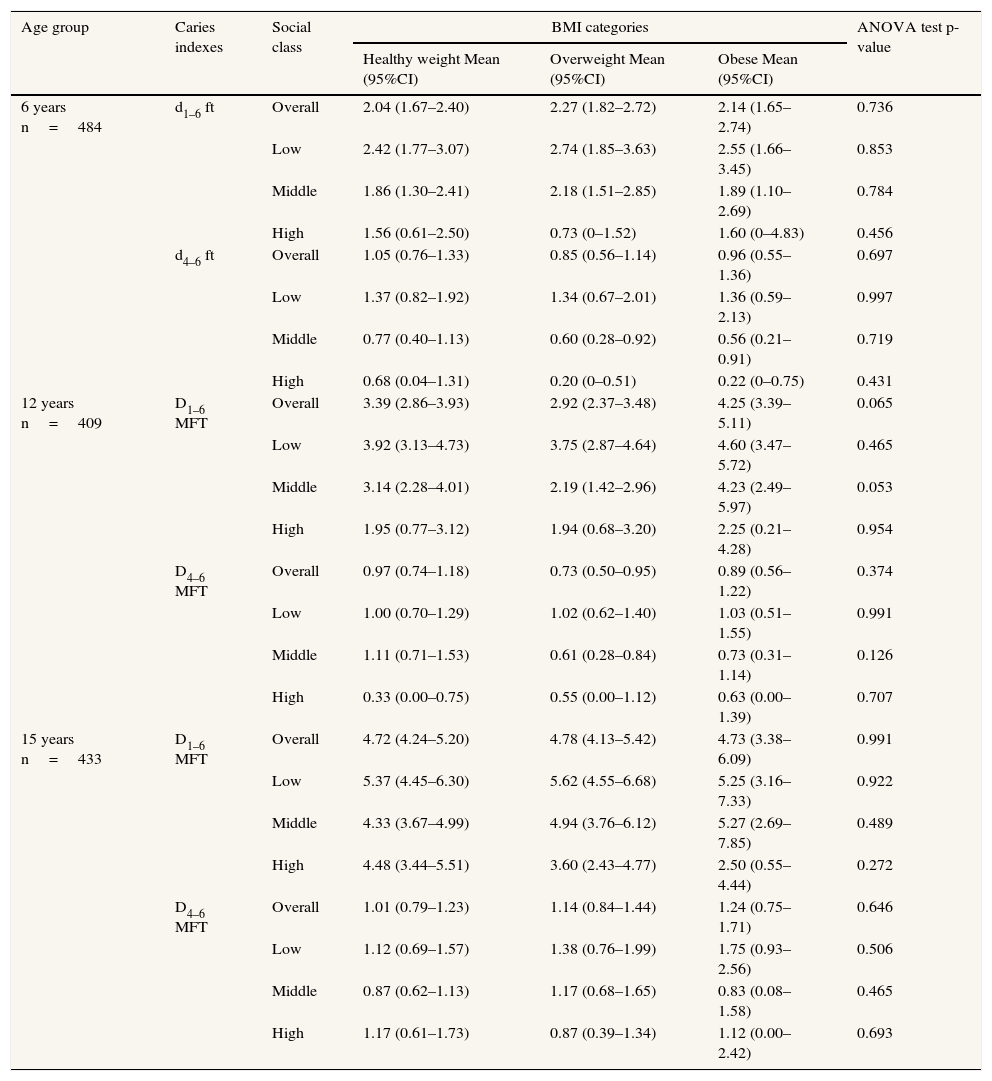
No significant differences in caries indexes (DMFT or dft) by degree of obesity stratified by social class were found in any of the age groups studied (Table 4).
Distribution of caries indexes by body mass index categories, stratified by social class.
| Age group | Caries indexes | Social class | BMI categories | ANOVA test p-value | ||
|---|---|---|---|---|---|---|
| Healthy weight Mean (95%CI) | Overweight Mean (95%CI) | Obese Mean (95%CI) | ||||
| 6 years n=484 | d1–6 ft | Overall | 2.04 (1.67–2.40) | 2.27 (1.82–2.72) | 2.14 (1.65–2.74) | 0.736 |
| Low | 2.42 (1.77–3.07) | 2.74 (1.85–3.63) | 2.55 (1.66–3.45) | 0.853 | ||
| Middle | 1.86 (1.30–2.41) | 2.18 (1.51–2.85) | 1.89 (1.10–2.69) | 0.784 | ||
| High | 1.56 (0.61–2.50) | 0.73 (0–1.52) | 1.60 (0–4.83) | 0.456 | ||
| d4–6 ft | Overall | 1.05 (0.76–1.33) | 0.85 (0.56–1.14) | 0.96 (0.55–1.36) | 0.697 | |
| Low | 1.37 (0.82–1.92) | 1.34 (0.67–2.01) | 1.36 (0.59–2.13) | 0.997 | ||
| Middle | 0.77 (0.40–1.13) | 0.60 (0.28–0.92) | 0.56 (0.21–0.91) | 0.719 | ||
| High | 0.68 (0.04–1.31) | 0.20 (0–0.51) | 0.22 (0–0.75) | 0.431 | ||
| 12 years n=409 | D1–6 MFT | Overall | 3.39 (2.86–3.93) | 2.92 (2.37–3.48) | 4.25 (3.39–5.11) | 0.065 |
| Low | 3.92 (3.13–4.73) | 3.75 (2.87–4.64) | 4.60 (3.47–5.72) | 0.465 | ||
| Middle | 3.14 (2.28–4.01) | 2.19 (1.42–2.96) | 4.23 (2.49–5.97) | 0.053 | ||
| High | 1.95 (0.77–3.12) | 1.94 (0.68–3.20) | 2.25 (0.21–4.28) | 0.954 | ||
| D4–6 MFT | Overall | 0.97 (0.74–1.18) | 0.73 (0.50–0.95) | 0.89 (0.56–1.22) | 0.374 | |
| Low | 1.00 (0.70–1.29) | 1.02 (0.62–1.40) | 1.03 (0.51–1.55) | 0.991 | ||
| Middle | 1.11 (0.71–1.53) | 0.61 (0.28–0.84) | 0.73 (0.31–1.14) | 0.126 | ||
| High | 0.33 (0.00–0.75) | 0.55 (0.00–1.12) | 0.63 (0.00–1.39) | 0.707 | ||
| 15 years n=433 | D1–6 MFT | Overall | 4.72 (4.24–5.20) | 4.78 (4.13–5.42) | 4.73 (3.38–6.09) | 0.991 |
| Low | 5.37 (4.45–6.30) | 5.62 (4.55–6.68) | 5.25 (3.16–7.33) | 0.922 | ||
| Middle | 4.33 (3.67–4.99) | 4.94 (3.76–6.12) | 5.27 (2.69–7.85) | 0.489 | ||
| High | 4.48 (3.44–5.51) | 3.60 (2.43–4.77) | 2.50 (0.55–4.44) | 0.272 | ||
| D4–6 MFT | Overall | 1.01 (0.79–1.23) | 1.14 (0.84–1.44) | 1.24 (0.75–1.71) | 0.646 | |
| Low | 1.12 (0.69–1.57) | 1.38 (0.76–1.99) | 1.75 (0.93–2.56) | 0.506 | ||
| Middle | 0.87 (0.62–1.13) | 1.17 (0.68–1.65) | 0.83 (0.08–1.58) | 0.465 | ||
| High | 1.17 (0.61–1.73) | 0.87 (0.39–1.34) | 1.12 (0.00–2.42) | 0.693 | ||
95%CI: confidence interval of 95%; BMI: body mass index.
There was no significant correlation between BMI and DMFT-dft in any of the age groups.
DiscussionChild obesity and dental caries in children constitute two major health problems in a large majority of countries nowadays and present great challenges for public health. In developed countries, child caries has remained stable, at low rates, since the early 21st century. The previous epidemiological study of oral health in children in the Valencia region of Spain —carried out in 2004 using the WHO diagnostic criteria18— estimated a caries prevalence of 32% in primary dentition and dft 1.08 at 6 years of age, and 42.5% caries prevalence in permanent teeth and DFMT 1.07 at 12 years of age. The caries data obtained in the present study are comparable. Moreover, the Spain-wide study of 2011 (the Aladino study) shows a high prevalence of obesity in the child population.19
Obesity and dental caries in children have been associated, although the results obtained in different studies are inconsistent and inconclusive. It is not clear whether they really are associated or whether they merely coexist simultaneously, as they share a common etiology and/or similar contributing factors. A number of authors have found an association between dental caries and obesity in young children and adolescents.10,20–26 However, not all the studies show the same strength of association, as some recognize that high weight is not per se an etiological factor in the development of caries,27 or that the association between overweight and caries prevalence is weak.3 Other authors show that overweight or obese adolescents have 1.6 times more interproximal caries than those of normal weight,23 although this is not the case in all age groups.20,23 Parental overweight has been considered a risk factor for the development of conditions such as obesity or caries in children.21 The children's predilection for particular foods, particularly sweets, sugar-rich foods —which have high levels of rapidly metabolized carbohydrates— and soft drinks, may explain the co-occurrence of child obesity and dental caries in many of the sample populations studied, since confounding risk factors such as frequency of intake, potentially cariogenic diets or poor oral hygiene are shared by both conditions.24
Among the systematic reviews and meta-analyses that have examined this association, Hooley et al.28 consider that there is evidence of an association between dental caries and BMI, although a clearer understanding of this association is needed.
The study by Hayden et al.26 indicates that when standardized definitions for the assessment of child obesity are used, a small overall association between obesity and level of caries in the permanent dentition is encountered: caries is more prevalent in obese children than in normal weight children. They find no association between obesity and caries in primary dentition.
The considerable heterogeneity of the studies could limit their external validity and the generalization of their results. Assessment of child weight status was not uniform across studies, and this variation in measurements may partly explain the inconclusive reports on the relationship between dental caries and obesity in the literature to date.26
The existence of studies conducted with similar methods to the present study supports its results concerning the absence of any relation between obesity and dental caries among schoolchildren in the Valencia region of Spain. Macek and Mitola,29 published the most heavily-weighted study based on participant numbers, and found no association between age-specific body mass index and increased dental caries prevalence and severity among US children. Nor did Sadeghi et al.30 find such an association in Iranian children. In the present study, the lack of association between dental caries and obesity could be influenced by factors related to the regular exposure of Valencian children to fluorine in toothpaste and to their being included in a weekly fluorinated mouthwash program at school. Additionally, the absence of such an association may relate to the fact that BMI in children changes substantially with age, and the changes are not correlated strictly with body fat.
Another confounding variable that may have influenced this relation is socio-economic class. Social class is considered an associated factor in the relation between BMI and dental caries.2–4,6,7,9,20–23,26,31,32 The factors that contribute to the two problems of caries and child obesity are both psychosocial and nutritional.9 The environment in which children spend their early years has an impact on their future oral health.23 Attending state rather than private schools has been shown to be a disadvantageous factor for caries prevalence, missing teeth and DMFT,7 as has residing in countries with a different level of development.4 These differences have been reflected in the conclusions of a recent meta-analysis: compared with normal weight children, obese children from industrialized countries have a significant relationship with caries, in contrast to those from non-industrialized countries.26
Family income has been considered a reliable predictor for child caries.3,22 Children with caries come from families with lower incomes, with parents of low educational levels and overweight mothers.21 Children of higher socioeconomic status who brush their teeth more often show a significantly lower prevalence and extent of DMFT, irrespective of weight status.2 The findings of the present study agree with numerous other studies in that decreasing socioeconomic status is associated with increasing development of caries,33 as has also been found in previous studies of the child population of Valencia.18 Recently, the latest epidemiological study of oral health in Spain, has shown a relationship between social disadvantage and presence of dental caries in both children and adults. Also observed a concentration of the disease in certain groups of individuals that suggest a change prevention strategies targeted specifically at risk groups.34
Gerdin et al.3 consider that there are two potential sources of bias in studies that examine the association between obesity and caries: the samples used and the role of socioeconomic status. As regards the former, the present study examined a representative random sample of the child population with appropriate sample sizes in each of the age groups, giving high power as well as highly reliable measurement of the different variables. A stratified statistical analysis was performed to check for the latter —possible socioeconomic bias. Analysis of the influence of social class on the relationship between caries and obesity found a lack of association in each of the three classes (high, middle and low), analyzed independently. Nevertheless, authors such as Marshall et al.21 did find caries and obesity coexisting in children of low social class.
In view of our outcomes, it may be concluded that there is no relation between obesity and caries in the child population, and social class does not influence this relationship. Future longitudinal studies could shed more light on the influence of social factors in the aetiology of both processes.35
Controlling overweight/obesity and caries in children needs to be approached as a public health problem and tackled through prevention, both in the school and in the family, by promoting health education in healthy lifestyle habits, paying particular attention to food. Strategies that address both diseases need to be considered, irrespective of whether or not there is really is an association between them.
Overweight, obesity and caries share aetiopathogenic factors that lead to their exhibiting a significant association in some populations but not in others. Consequently, BMI should not be used as a predictor variable in the different multi-variant models for caries. The multi-factor aetiology and considerable complexity of the interactions that occur during the two processes call for more profound research into lifestyle-related aspects, adopting a longitudinal rather than a cross-sectional perspective.
Editor in chargeLaura I. González Zapata.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Dental caries is a high prevalent multifactorial disease. The approach strategy should be based on the prevention of common risk factors with other prevalent diseases such as obesity and diabetes in developed countries. However, the association between caries and obesity is inconclusive in the literature.
What does this study add to the literature?The multifactorial etiology of caries implies difficulty to find a clear association between obesity and dental caries in children and young people of the Spanish population even stratifying by social class.
Conception and design of study: José Manuel Almerich-Silla, José María Montiel-Company. Acquisition of data: Teresa Almerich-Torres, Carlos Bellot-Arcís, José María Montiel-Company. Analysis and/or interpretation of data: Teresa Almerich-Torres, Carlos Bellot-Arcís, José María Montiel-Company, José Manuel Almerich-Silla. Drafting the manuscript: Carlos Bellot-Arcís, José María Montiel-Company, José Manuel Almerich-Silla. Revising the manuscript critically for important intellectual content: Teresa Almerich-Torres, Carlos Bellot-Arcís, José María Montiel-Company, José Manuel Almerich-Silla. Approval of the version of the manuscript to be published: Teresa Almerich-Torres, Carlos Bellot-Arcís, José María Montiel-Company, José Manuel Almerich-Silla.
FundingFinancial support for the research has been received through grants for Research Projects in Health and Disease Prevention and Prediction Programmes from the Valencia Regional Government Health Department in 2010, and grants for the Epidemiological Study of Oral Health in the Schoolchild Population of the Valencian Community 2010 (UV-INV-AE11-40221) from the University of Valencia.
Conflict of interestsNone.
The authors wish to thank Mary Georgina Hardinge for translating this paper.











