





Stem cell transplantation has been used for many years to treat haematological malignancies that could not be cured by other treatments. Despite this medical breakthrough, mortality rates remain high. Our purpose was to evaluate labour productivity losses associated with premature mortality due to blood cancer in recipients of stem cell transplantations.
MethodsWe collected primary data from the clinical histories of blood cancer patients who had undergone stem cell transplantation between 2006 and 2011 in two Spanish hospitals. We carried out a descriptive analysis and calculated the years of potential life lost and years of potential productive life lost. Labour productivity losses due to premature mortality were estimated using the Human Capital method. An alternative approach, the Friction Cost method, was used as part of the sensitivity analysis.
ResultsOur findings suggest that, in a population of 179 transplanted and deceased patients, males and people who die between the ages of 30 and 49 years generate higher labour productivity losses. The estimated loss amounts to over €31.4 million using the Human Capital method (€480,152 using the Friction Cost method), which means an average of €185,855 per death. The highest labour productivity losses are produced by leukaemia. However, lymphoma generates the highest loss per death.
ConclusionsFurther efforts are needed to reduce premature mortality in blood cancer patients undergoing transplantations and reduce economic losses.
Durante muchos años el trasplante de células madre se ha usado para tratar neoplasias hematológicas que no podrían haber sido curadas mediante otras terapias. A pesar de este avance médico, la ratio de mortalidad es aún elevada. Nuestro objetivo es evaluar las pérdidas de productividad laboral por mortalidad prematura debido a una neoplasia hematológica en receptores de trasplante de células madre.
MétodosSe recogieron datos primarios de las historias clínicas de pacientes con neoplasia hematológica, trasplantados durante los años 2006 y 2011 en dos hospitales españoles. Se realizó un análisis descriptivo y se calcularon los años potenciales de vida y los años potenciales de vida laboral perdidos. Las pérdidas de productividad laboral se estimaron usando el método del Capital Humano. El método de los Costes de Fricción se empleó como parte del análisis de sensibilidad.
ResultadosEn una población de 179 pacientes trasplantados y fallecidos, se dan mayores pérdidas de productividad laboral en varones y en personas de edades comprendidas entre los 30 y 49 años. La pérdida estimada está por encima de €31.4 millones usando el método del Capital Humano (€480,152 usando el método Costes Fricción), lo que significa una pérdida media de €185,855 por persona fallecida. Las mayores pérdidas globales son generadas por la leucemia. Sin embargo, el linfoma genera las mayores pérdidas por fallecimiento.
ConclusionesMayores esfuerzos son necesarios para reducir la mortalidad prematura de pacientes trasplantados por neoplasia hematológica y reducir el impacto económico y social asociado a la misma.
The attributable annual number of deaths worldwide due to cancer is predicted to rise from 7.6 million in 2008 to 13 million in 2030.1 The International Agency for Research of Cancer (IARC) estimated that 94.4 thousands deaths would occur in 2012 due to haematological malignancies (or blood cancer) in the 27 countries of the European Union (7.49% incidence rate).2 Spain follows a similar trend, with blood cancer (taking into account leukaemia, lymphoma and multiple myeloma) being the fourth most common cause of death among all types of cancers3 having caused an estimated 7.4 thousand deaths in 2012 which means a rate of 7.24%.2
Because of this high mortality rate, the development and progressive evolution of haematopoietic stem cell transplantation (HSCT) in recent decades has been an important medical advance. HSCT has become an effective treatment for malignant and benign haematological diseases that could not be cured by other therapies, allowing for an increasing number of patients to become long-term survivors.4,5 It is an essential part of the therapeutic strategy which is clinically recommended for blood cancer patients whose clinical condition indicates transplantation, are less than 65 years old (occasionally it can be higher) and are free of severe co-morbidities.4 In Spain, throughout Europe, its use has increased in a linear trend. In 2013, 2,945 transplantations were carried out in Spain in comparison with 1,974 transplantations in 2006.6 However, HSCT remains associated with significant morbidity and mortality rates5 and it is one of the most expensive treatments of specialized medicine in Spain.7
International and national studies have assessed labour productivity losses due to mortality and morbidity for many cancers.8–13 Some of them have focused on specific types of cancer such as cervical, pancreatic, prostate and a large number on breast cancer.14–17 However, to our knowledge, few studies have reported information about labour productivity losses due to blood cancer: one study was published two decades ago in Sweden, as part of a cost of illness analysis and took into account labour productivity losses due to morbidity and mortality in acute myeloid leukaemia,18 also two articles concerning chronic lymphocytic leukaemia and lymphoma were recently published in Germany,19,20 and in two articles about cancer, leukaemia and lymphoma were found to be amongst ten of the most costly cancers in terms of lost productivity due to premature cancer-related mortality.8,10
According to the national literature, just one Spanish study mentions “diseases of the blood and blood organs and disorders that affect immunity and the haematopoietic system” as an area of study and calculates losses in labour productivity due to death.13 Detailed information on different haematological diseases, stages or further treatments such as transplantation were not available in any national or international study. In addition, all of them follow the same methodology, the human capital method, and no specific study has been published on haematopoietic stem cell transplantation in spite of its increasing incidence in the society.
Our purpose is to provide detailed and useful information on affairs relating to one of the economic aspects of blood cancer. More specifically, our purpose is to estimate loss of labour productivity caused by the premature deaths of blood cancer patients who received stem cell transplantation.
MethodsDataSpain does not have a disaggregated national database containing details of treatments and mortality rates of malignant haematological diseases. Due to the lack of information, a primary database was created based on two hospital registries: Haematology Department of University Hospital of Virgen del Rocío (Seville) and Haematology Department of University Hospital of Virgen de las Nieves of Granada (Granada). The Clinical Research Ethics Committee of both health centres approved the study. Both hospitals are referenced in malignant haematological diseases in southeast and southwest in Spain, respectively. Our sample took into account the total adult population (over 16 years of age) in the provinces of Granada and Seville that received HSCT between 2006 and 2011 due to blood cancer and died before July 2012. Diagnoses of the patients were leukaemia, lymphoma, multiple myeloma, myelodisplastic syndrome and other malignant haematological diseases.
Study designWe used standard statistics to describe the sample. Deaths were calculated in terms of years of potential life lost (YPLL) and years of potential productive life lost (YPPLL). YPLL was calculated following the methodological recommendations of the Spanish National Statistics Institute (INE) which considers premature death to be the years a person would have left to live if not for an early mortality which does not occur at the usual age of death for its collective.21 The range of early mortality was considered to be between 1 to 69 years of age. Then, we transformed YPLL into YPPLL by estimating the number of total deaths during working age, in other words, between 16 and 65 years of age, being 65 the legal age of retirement at the time of the study in Spain. No discount rate was used for these calculations.
The costs due to early mortality were calculated by applying the human capital (HC) method to the field of health. This approach points out that negative effects on the health of an individual might cause undesirable effects on their productivity at work and at home, and may result in a loss of leisure time not just for patients but also for caregivers. So, in the case of a worker who leaves the labour market due to premature mortality, the potential labour productivity towards the end of their working life will have been lost by society.22,23
The average earnings (wage) of a worker are considered a reasonable estimation of labour productivity.23 An incidence approach was used. We calculated the number of deaths of working-age individuals. The age limit for workers to remain in the labour market was set at 65 years. Once the age of individuals at the time of death and their expected gross lifetime wages were known, the present and future flow of productivity lost because of premature death could be calculated. The expected earnings and the employment rate were applied to each case, controlled by age and gender up to the predetermined limit of 65 years. Our calculations were performed based on the average gross wage figures contained in the latest Spanish Wage Structure Survey of the National Statistics Institute.24 Employment data was obtained from the latest Labour Force Survey, also conducted by the National Statistics Institute, which defines the employment rate as the percentage of the population that is employed in relation to the total population of working age.25 The costs were actualized for 2009.
Our base case took into account the annual growth rate of labour productivity in Spain from 2001 to 2012 which was 0.9%,26 and 4.3% as the annual discount rate, which is the mean profitability of 10-year government bonds in Spain from 2002 to 2012.27 This is coherent with the recent methodological suggestions in economic evaluations.28 For the sensitivity analysis, we varied annual growth rates between 0%-2% and annual discount rates between 0%-6% as standard measures to facilitate comparison with international literature.28 We carried out an additional sensitivity analysis for estimating labour productivity losses using the friction cost (FC) method. According to this approach, workers who are forced to leave their jobs because of illness or mortality do not cause a large loss in productivity for society. The only productivity loss occurs while the post remains vacant. The authors estimated that this period could last between 2.5 and 3.5 months and it is called the “friction period”.29,30
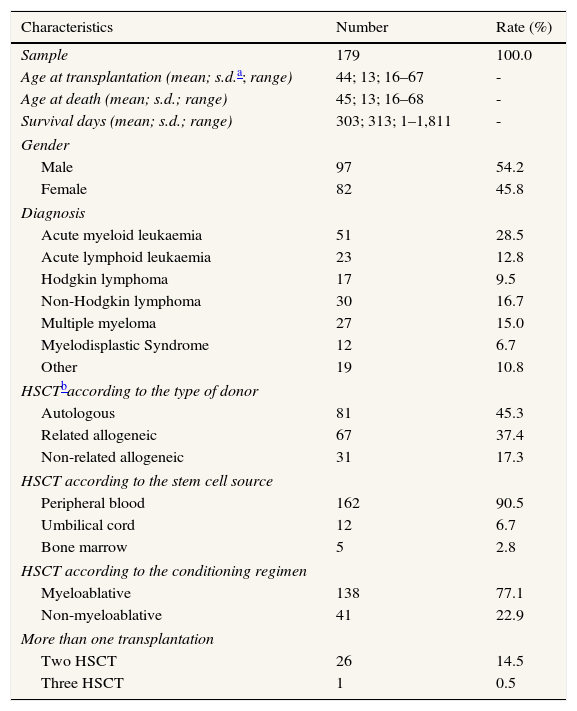
Results179 out of 496 patients over 16 years of age underwent transplantations between 2006 and 2011 and had died as of July 2012. The average age at death was 45. The mean survival time from the day of the transplantation day was less than one year (303 days). 54.2% of the patients were male. The disease with the highest rate of mortality was leukaemia (41.3%). 45.3% were autologous transplantations, 90.5% were peripheral blood transplantations and 77.1% of patients received a myeloablative conditioning regimen. The descriptive characteristics of the study sample are shown in Table 1.
Characteristics of patients.
| Characteristics | Number | Rate (%) |
|---|---|---|
| Sample | 179 | 100.0 |
| Age at transplantation (mean; s.d.a; range) | 44; 13; 16–67 | - |
| Age at death (mean; s.d.; range) | 45; 13; 16–68 | - |
| Survival days (mean; s.d.; range) | 303; 313; 1–1,811 | - |
| Gender | ||
| Male | 97 | 54.2 |
| Female | 82 | 45.8 |
| Diagnosis | ||
| Acute myeloid leukaemia | 51 | 28.5 |
| Acute lymphoid leukaemia | 23 | 12.8 |
| Hodgkin lymphoma | 17 | 9.5 |
| Non-Hodgkin lymphoma | 30 | 16.7 |
| Multiple myeloma | 27 | 15.0 |
| Myelodisplastic Syndrome | 12 | 6.7 |
| Other | 19 | 10.8 |
| HSCTbaccording to the type of donor | ||
| Autologous | 81 | 45.3 |
| Related allogeneic | 67 | 37.4 |
| Non-related allogeneic | 31 | 17.3 |
| HSCT according to the stem cell source | ||
| Peripheral blood | 162 | 90.5 |
| Umbilical cord | 12 | 6.7 |
| Bone marrow | 5 | 2.8 |
| HSCT according to the conditioning regimen | ||
| Myeloablative | 138 | 77.1 |
| Non-myeloablative | 41 | 22.9 |
| More than one transplantation | ||
| Two HSCT | 26 | 14.5 |
| Three HSCT | 1 | 0.5 |
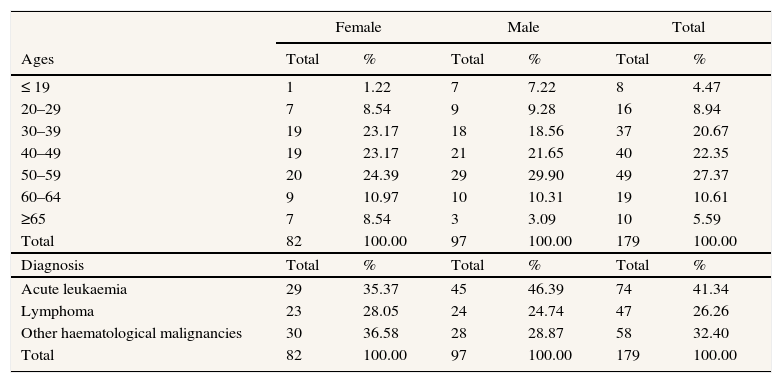
When distributing the deaths by age and gender, we found most of the deaths happened in the 50–59 age group (27.37%) followed by the 40–49 age group (22.35%). However, detailed information shows that for patients under 30 years of age, the death rate of men was higher than that of women (16.50% vs. 9.76%). On the other hand, over 30 years of age, the death rate of men was lower than that of women, except for the 50-59 age group (Table 2). As we can see in Table 2, leukaemia was the disease with the highest rate of mortality (41.34% of deaths) and the highest rate of death in men (46.39%). The YPLL and YPPLL was identified as 4,268 and 3,563 respectively (Table I in Appendix on-line).
Number of deaths by age group, diagnosis and gender.
| Female | Male | Total | ||||
|---|---|---|---|---|---|---|
| Ages | Total | % | Total | % | Total | % |
| ≤ 19 | 1 | 1.22 | 7 | 7.22 | 8 | 4.47 |
| 20–29 | 7 | 8.54 | 9 | 9.28 | 16 | 8.94 |
| 30–39 | 19 | 23.17 | 18 | 18.56 | 37 | 20.67 |
| 40–49 | 19 | 23.17 | 21 | 21.65 | 40 | 22.35 |
| 50–59 | 20 | 24.39 | 29 | 29.90 | 49 | 27.37 |
| 60–64 | 9 | 10.97 | 10 | 10.31 | 19 | 10.61 |
| ≥65 | 7 | 8.54 | 3 | 3.09 | 10 | 5.59 |
| Total | 82 | 100.00 | 97 | 100.00 | 179 | 100.00 |
| Diagnosis | Total | % | Total | % | Total | % |
| Acute leukaemia | 29 | 35.37 | 45 | 46.39 | 74 | 41.34 |
| Lymphoma | 23 | 28.05 | 24 | 24.74 | 47 | 26.26 |
| Other haematological malignancies | 30 | 36.58 | 28 | 28.87 | 58 | 32.40 |
| Total | 82 | 100.00 | 97 | 100.00 | 179 | 100.00 |
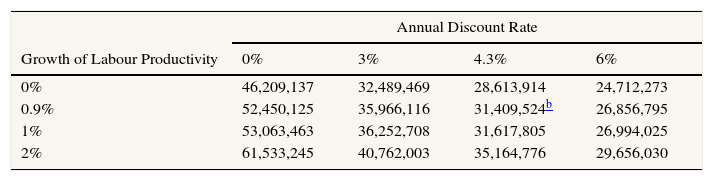
In our base case, we estimated €31.4 million as the cost of labour productivity lost due to premature mortality. The maximum and minimum values obtained in the sensitivity analysis ranged between €61.5 using 2% as the annual growth rate and 0% as the annual discount rate, and €24.7 million using 0% as the annual growth rate and 6% as the annual discount rate. The standard rate characterized by 1% annual growth rate and 3% as annual discount rate valued €36.2 million (Table 3).
Labour productivity losses (€) due to premature deaths in blood cancer patients undergoing HSCTa for the year 2009. Human Capital method.
| Annual Discount Rate | ||||
|---|---|---|---|---|
| Growth of Labour Productivity | 0% | 3% | 4.3% | 6% |
| 0% | 46,209,137 | 32,489,469 | 28,613,914 | 24,712,273 |
| 0.9% | 52,450,125 | 35,966,116 | 31,409,524b | 26,856,795 |
| 1% | 53,063,463 | 36,252,708 | 31,617,805 | 26,994,025 |
| 2% | 61,533,245 | 40,762,003 | 35,164,776 | 29,656,030 |
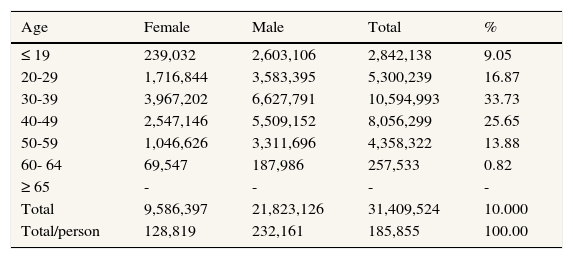
The average potential production loss per person was €185,855, taking into account our base case. Our results show that 69.5% of the total productivity losses are generated by men (€21,823,126) and 30.5% by women (€9,586,397). Additionally, almost 60% of productivity losses are generated by people who die between 30 and 49 years of age, and most of them between 30 and 39 (33.7%), in spite of the fact that in our sample most people died between the ages of 50 and 59 (Table 4).
Labour productivity losses (€) due to premature deaths by age group and gender in blood cancer patients undergoing HSCTa for the year 2009. Human Capital method. Base case (0.9%, 4.3%).
| Age | Female | Male | Total | % |
|---|---|---|---|---|
| ≤ 19 | 239,032 | 2,603,106 | 2,842,138 | 9.05 |
| 20-29 | 1,716,844 | 3,583,395 | 5,300,239 | 16.87 |
| 30-39 | 3,967,202 | 6,627,791 | 10,594,993 | 33.73 |
| 40-49 | 2,547,146 | 5,509,152 | 8,056,299 | 25.65 |
| 50-59 | 1,046,626 | 3,311,696 | 4,358,322 | 13.88 |
| 60- 64 | 69,547 | 187,986 | 257,533 | 0.82 |
| ≥ 65 | - | - | - | - |
| Total | 9,586,397 | 21,823,126 | 31,409,524 | 10.000 |
| Total/person | 128,819 | 232,161 | 185,855 | 100.00 |
Table 5 shows the cost of lost labour productivity by diagnosis, which was divided into three haematological disease groups according to their incidence: leukaemia, lymphoma and other haematological malignant diseases. The highest losses were accounted for by leukaemia (€15,141,521) because it had the highest death rate. However, lymphoma accounted the highest losses per death (€212,944) despite having the smallest number of deaths. This is because the average age of death in patients with lymphoma was the lowest for both males and females in comparison with other diagnoses.
Labour productivity losses (€) due to premature mortality by diagnosis in blood cancer patients undergoing HSCT, for the year 2009. Human Capital method. Base case (0.9%, 4.3%).
| Number of deaths (under 65 years old) | Average female age of death (s.d.) | Average male age of death (s.d.)a | Total productivity losses (€) | Total productivity losses/person (€) | |
|---|---|---|---|---|---|
| Acute leukaemia | 74 | 44 (10) | 41 (14) | 15,141,521 | 204,615 |
| Lymphoma | 46 | 43 (12) | 40 (13) | 9,795,424 | 212,944 |
| Other haematological malignancies | 49 | 52 (14) | 52 (12) | 6,472,579 | 132,093 |
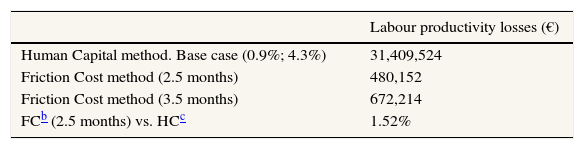
In a sensitivity analysis, the FC method showed labour productivity losses of €480,153 for society (€2,841 per person), assuming the friction period lasts 2.5 months. It rises to €672,214 (€3,977 per person) using 3.5 months as the friction period. The FC method shows 1.52% of the costs of those determined by the HC method (Table 6).
Sensitivity analysis of labour productivity losses (€) in blood cancer patients undergoing a HSCTa for the year 2009.
The IARC projected an increased incidence of cancer in Europe of 32% beginning in the mid-80s.2 Haematological malignancies has been one of cancers with the biggest increases in incident rate. In 2012, 186.7 thousand new cases of blood cancer were estimated in the EU-27 and 14.9 thousand in Spain.2 The predictions for Spain are now to reach 17.2 thousand new cases in 2015.3
This increased incidence makes it necessary to study the costs associated with different treatments to discover the economic impact on society (direct costs, indirect costs and informal care costs). Particularly, the European Society for Medical Oncology concluded, after reviewing many international articles, that labour productivity costs accounted for more than two-thirds of the total costs of cancer.9 However, few studies have been published relating to non-health care costs in the haematologic area, even though stem cell transplantation is an essential part of the treatment for increasing survival rate of patients and one of the most expensive therapies in Spain7. Our study partially fills the knowledge gap highlighted by many authors on non-health care costs in the haematologic area.19,20,31,32
We examined the potential labour productivity loss that society could gain if the transplantations were effective enough to allow oncohaematologic patients to survive and continue working in the labour market. This subgroup of patients received the best available treatment according to the clinical protocol, but premature mortality and productivity losses are still high. We conclude that, in a sample of 179 transplanted patients, 3,563 years of potential productivity have been lost and that the productivity losses for society because of early death have reached €31.4 million. In other words, our findings suggest that society could save on average €185,855 per surviving patient if they could have a quality of life good enough to continue working in the labour market. 69.5% of the total labour productivity losses are accounted for by men. This is due to the incorporation of economic information such as labour force participation and wage rates into the estimates, which usually inflate male costs relative to female cost.8,10–12 People who die between 30 and 49 years of age and leukaemia patients generate the higher losses. In contrast, losses are smaller using the Friction Cost method, representing just the 1.52% of losses showed by the Human Capital method. There is no agreement about which method is the best and both have been criticized.33 Some authors consider that HC method overestimates the results,29,30 however it is solidly grounded in neoclassical economic framework. In contrast, FC approach breaks basic axioms of economic theory due to the absence of a theoretical framework. This could possibly be one of the underlying reasons for the increased use of HC in applied studies, although there are other reasons that hamper the empirical application of the friction cost method.34
According to the international literature, which follows the Human Capital method, blood cancer is one of the most costly cancers in terms of cost of lost productivity due to premature mortality. A recent article published by Hanly et al.8 estimated the premature mortality costs of the 10 most common cancers in Ireland. They estimated that the most costly cancer in males, was leukaemia (€426,247 per death) followed by non-Hodgkin's lymphoma in the third position (€385,480 per death). Non-Hodgkin's lymphoma was the third highest in females (€157,289 per death). Kim et al.35 published a similar article studying the economic burden of cancer in Korea. Leukaemia was the second most costly cancer ($167,000 per death), Hodgkin's lymphoma was estimated at $157,000, non-Hodgkin's lymphoma at $128,000, and multiple myeloma at $89,000 per death. Bradley et al.10 estimated cancer-related productivity costs in US and they pointed out that Hodgkin's lymphoma was the second most expensive ($544,118 per death). Leukaemia was calculated at $240,387 and non-Hodgkin's lymphoma at $219,407 per death. Just two studies have focused on the estimation of loss labour productivity due to premature mortality associated with blood cancer, specifically in acute myeloid leukaemia in Sweden in 1994 and malignant lymphoma in Germany in 2000.18,19 Loss per patient could not be calculated because of the lack information in both articles about the number of deaths of people under 65 years of age. Costs are very different depending on the country, and these differences are due to the labour market conditions and wages. Also, variables, such as type of cancer, methodology used, age or gender, influence the results and make comparison between studies more difficult.10,14,33
Our results are in line with those reported by other national studies. Antoñanzas et al.12 concluded that labour productivity losses due to premature mortality are distributed in an unequal way by gender in oncologic patients, as they are higher in men. Their results show an average labour productivity loss per premature death due to cancer of €92,592 (prices actualized to the year 2003). In the same line, Oliva et al.13 estimated €90,550 per patient in 2011. However, their further study pointed out the differences in cost depending on the type of cancer.14 The losses were calculated as €69,332 and €52,486 per premature death in cervical and breast cancer, respectively. They also compared HC vs. FC methods, obtaining sharp differences between them. Just their first study took into account haematological diseases, estimating a total labour productivity loss of €189,828 per premature death.13 These results are totally in agreement with ours.
Several limitations of our study should be noted. The first limitation is our limited population on transplanted patients. This means that our results could not be extrapolated to the total blood cancer population in working age. Future directives for research could focus on amplifying our analysis using other Spanish health centres’ registries to increase the external validity of the present study and also using non-transplanted patients to compare results. The second limitation is related to the estimated average survival time. Given the short study period for people who had transplantation during 2010 and 2011, there could be a possible bias due to deaths out of the observational period. However, it is expected to be small. Thirdly, given the complexity of modelling employment rates for an uncertain future and following other studies, current employment rates were used in our analysis. Finally, the Friction Cost method determines the friction period as 2.5 or 3.5 months, however this period could be longer or shorter depending on the economic cycle of each country and its market labour.29,30,33
Our study is unique because the collection of premature mortality data is novel, takes into account the total transplanted population with blood cancer in two provinces, fills the lack of knowledge due to limited public information in Spain and captures three important domains: diagnosis, gender and age. Thus, this is the first study to examine labour productivity loss in a subgroup of transplanted patients.
As some authors have remarked, it is necessary to use a social perspective to gain in-depth knowledge of blood cancer treatment costs.31,32 Our results provide new information about labour productivity losses due to premature mortality of blood cancer patients who received a stem cell transplantation and add useful information about economic dimension that is valuable to society and decision-makers. They could be useful for future cost of illness studies in order to complement their epidemiological information.
Annual number of deaths due to blood cancer is rising every year. However, many few international studies have explored in-depth labour productivity losses due to premature mortality and none of them have focused on further treatment as stem cell transplantation. We give primary information to the international and national literature.
What does this study add to the literature?This paper gives further information on labour productivity losses due to premature mortality in Spanish blood cancer patients, specifically on patients undergoing stem cell transplantation as part of their treatment. These non-medical costs of blood cancer could be taking into account by policy-makers for future policies. These results are very useful for future Spanish and international cost of illness studies due to the primary and disaggregated data.
This study has no received financial support.
Contribution and authorshipM. Ortega-Ortega was the principal researcher and took primary responsibility for the paper. She coordinated the work jointly with J. Oliva-Moreno and JD. Jiménez-Aguilera and they analyzed statistically the database. A. Romero-Aguilar, I. Espigado-Tocino and M. Ortega-Ortega participated in data collection, aggregation and quality control of the databases. All the results were discussed among the authors. M. Ortega-Ortega wrote the first draft of the manuscript and the rest of the authors helped in the successive reviews up to the final version. All the authors have approved the final version.
Conflicts of interestThe authors report no potential conflicts of interest.
The authors would like to thank the collaboration of the University Hospital Virgen de las Nieves (Granada, Spain) and University Hospital Virgen del Rocío (Seville, Spain), specially to health professionals of Haematology Department of both hospitals for their support in this study. The authors also thank F. Márquez Malaver for his contribution to improve quality of data.












