



To examine the effect of perceived discrimination and self-rated health among the immigrant population in the Basque Country, Spain, and determine whether this effect varies according to region of origin, age, sex and education.
MethodsDescriptive cross-sectional study. The study population included immigrants aged 18 and older residing in the Basque Country. Data from the 2014 Foreign Immigrant Population Survey (n=3,456) were used. Log-binomial regression was used to quantify the association between perceived discrimination and self-rated health before and after checking for the selected characteristics.
ResultsAlmost 1 in 10 immigrant adults reports perceiving discrimination. In adjusted analyses, the immigrants perceiving discrimination were almost were 1.92 more likely to rate their health as poor (prevalence ratio: 1.92; 95% CI: 1.44–2.56) than those who did not report discrimination. This association did not vary according to region of origin, age, sex or educational level.
ConclusionsPerceived discrimination shows a consistent relationship with perceived health. Moreover, this association did not depend on the region of origin, age, sex or educational level of immigrants. These results show the need for implementing inclusive policies to eliminate individual and institutional discrimination and reduce health inequalities between the immigrant and native populations.
Examinar el efecto de la discriminación en la salud percibida en la población inmigrante en el País Vasco y si este efecto es explicado por las diferencias en la región de origen, la edad, el sexo y la educación.
MétodosEstudio descriptivo transversal cuya población de estudio fue la población inmigrante de 18 años y más de edad, en el País Vasco. Los datos proceden de la Encuesta de Población Inmigrante Extranjera 2014 (n=3456). Se utilizó la regresión log binomial para medir la asociación entre la discriminación y la salud percibida antes y después de controlar por las características seleccionadas.
ResultadosLa discriminación fue referida por casi uno de cada 10 inmigrantes. En los análisis ajustados, los inmigrantes que refirieron discriminación tuvieron 1,92 de probabilidad de tener mala salud (razón de prevalencia: 1,92; intervalo de confianza del 95%: 1,44-2,56) en comparación con quienes no la refirieron. Esta asociación no cambió según la región de origen, el sexo ni el nivel de estudios.
ConclusionesLa percepción de discriminación muestra una consistente relación con la salud percibida. Además, esta relación no depende del lugar de origen, la edad, el sexo ni el nivel de estudios de los inmigrantes. Estos resultados muestran la necesidad de implementar políticas inclusivas que eliminen la discriminación, tanto individual como institucional, para reducir las desigualdades en salud entre la población inmigrante y la autóctona
Studies investigating the relationship between racial/ethnic discrimination and health outcomes have increased over the past decade. Most of these studies have been conducted in the United States (US) and have focused on discrimination and self-rated health,1,2 mental health,2–4 cardiovascular diseases,5 diabetes,3 hypertension6 as well as use and access to health care.7 Consistently, these studies provide evidence of the negative or detrimental effects of discrimination on health outcomes.8
In Europe, the study of discrimination and health status has been steadily increasing over the last decade, especially in the immigrant population, the main source of racial and ethnic diversity in European societies.9 These studies show that discrimination explains a great proportion of the inequalities observed for health outcomes between the native and immigrant population.10–13 Over the past two decades, Spain has experience an intense arrival of immigrant population ranking fourth country in the European Union since 2010.14 Although the economic crisis has affected immigration, this population represent 12.7% of the Spanish population in 2016.15 In the Basque Country, where immigration has always been lower, the immigrant population represents 8.8% of the total population in 2016.15 However, it is one of the few regions that has grown in immigrant population during most of the period of economic crisis.16 The least impact of the crisis and its latest entry of the Basque Country have contributed to this situation. In addition, there have been lower cuts in social policies and less discriminatory towards immigrants, as in the case of the not application of the Royal Decree (RD) 16/2012, which excludes access to health services to immigrants in irregular situation.17
The increase of the immigrant population has changed the socio-demographic of Spain and led to an interest on learning about the health effects of migration processes and social factors such as the discrimination associated with the incorporation of this population into the host societies. The latter could lead to discrimination at both the individual (as a result of interpersonal relationships) and the institutional level (due to policies, structures and regulations that may be discriminatory).18 Recent evidence shows that discrimination is associated with poorer health outcomes, including self-rated health19–23 in Spain. However, most of these studies used convenience samples or aggregate immigrants regardless of country or region of origin into a single category.
Despite the evidence on the associations between discrimination and health status, it is unclear whether this association varies with the place of origin, gender, age or level of education. Differential discrimination exposures could be expected on immigrants according to place of origin as a result of the attitudes of the host population towards groups more distant culturally and historically. This differential effect could also be affected by contextual factors related to policies for immigrant integration. However, in Europe, a few studies examining the association between perceived discrimination and health taking into account the place of origin showed mixed results. Some studies have found a stronger association in immigrants from particular origins10,22 while other found an associations regardless of place of origin.10
Gender could also determine greater exposure to discrimination, and therefore, have a higher impact on women's health. However, evidence is still inconsistent with some studies reporting poor self-rated health associated with discrimination in women13,19 whereas others found this association among men.22 Other important factors such as age13 and education13,21 could modify the effect of discrimination on health. However, evidence is inconsistent with some studies suggesting a stronger association between discrimination and poor health among younger and highly educated immigrants,19,24 whereas other among the least educated immigrants.25 Therefore, to elucidate these gaps in the literature, this study aims to examine the association between perceived discrimination and self-rated health among the immigrant population in the Basque Country, Spain; and whether this association varies with region of origin, age, gender or education.
MethodsStudy design and populationThe study used data from the Foreign Immigrant Population Survey 2014 (EPIE). The EPIE is a representative cross-sectional survey of the immigrant population residing in family dwellings in the Basque Country, Spain (N=5912). This survey has been conducted every four years by the Basque Government since 2010. The EPIE 2014 collected information on the living conditions of the immigrant population and included information on health status and health care utilization. A random sampling design stratified by place of birth and place of residency using information from the 2013 Census data was used. Information was collected via family (5912) and individual (2350) questionnaires. All the interviews used in this study were performed in Spanish. Moreover, the completion rates for family and individual questionnaires were 73.5% and 69.3%, respectively. These analyses are based on the family questionnaires.
VariablesThe outcome was self-rated health, a multidimensional measure of physical and psychological health, shown to be a significant predictor of morbidity and mortality and use of health care.26 Self-rated health was evaluated using the question “How is your health in general?”, with answers from very good to very bad. For analytical purposes, self-rated health was specified as good (very good and good) and poor (fair, bad and very bad).8
The independent variable, perceived discrimination, was collected through the question “In the past year, have you suffered problems of social rejection because of your social or geographical origin, race, ethnicity, culture, language, religion or administrative status?”, with answers of yes and no.
Consistent with previous studies,23 we considered region of origin (Europe, Africa, Latin America and Asia), age (18-24, 25-34, 35-49, >49 years), gender, educational attainment (primary or less, secondary and graduate or higher), employment status (employed, unemployed and others), administrative situation (permanent resident, non-permanent resident and irregular resident), and length of stay in the Basque Country (<5, 5-10, >10 years).
Of total EPIE participants (n=5912), we excluded those younger than 18 years of age (n=1661), those born in countries with a Human Development Index (HDI) very high in 2015 (≥0.83) (n=302) and those born in the Basque country (n=493). These exclusions resulted in an analytical sample of 3456.
Statistical analysisDescriptive statistics for selected characteristics were calculated for the total population and according to region of origin. In addition, prevalence estimates for self-rated health were calculated for each covariate according to region of origin. Chi-square and Cochran-Mantel-Haenszel statistics were used to assess significance associations between each covariate and region of origin and each covariate and self-rated health according to region of origin. We used log-binomial regression to quantify the association between discrimination and self-rated health before and after controlling for selected covariates. We tested interactions terms between discrimination and each covariate considered as effect measure modifier (region of origin, age, gender and education) in the fully-adjusted model.
Data management procedures were carried out using SPSS 22.0. (IBM, Armonk, NY) whereas the statistical analyses were conducted using SUDAAN 11.0.1 (RTI, Research Triangle Park, NC) to take into account the complex sampling design and yield unbiased standard error estimates. Sample sizes presented in Table 1 were un-weighted, but all other estimates (proportions, standard errors, prevalence ratios [PR] and their 95% confidence intervals [95%CI]) were weighted.
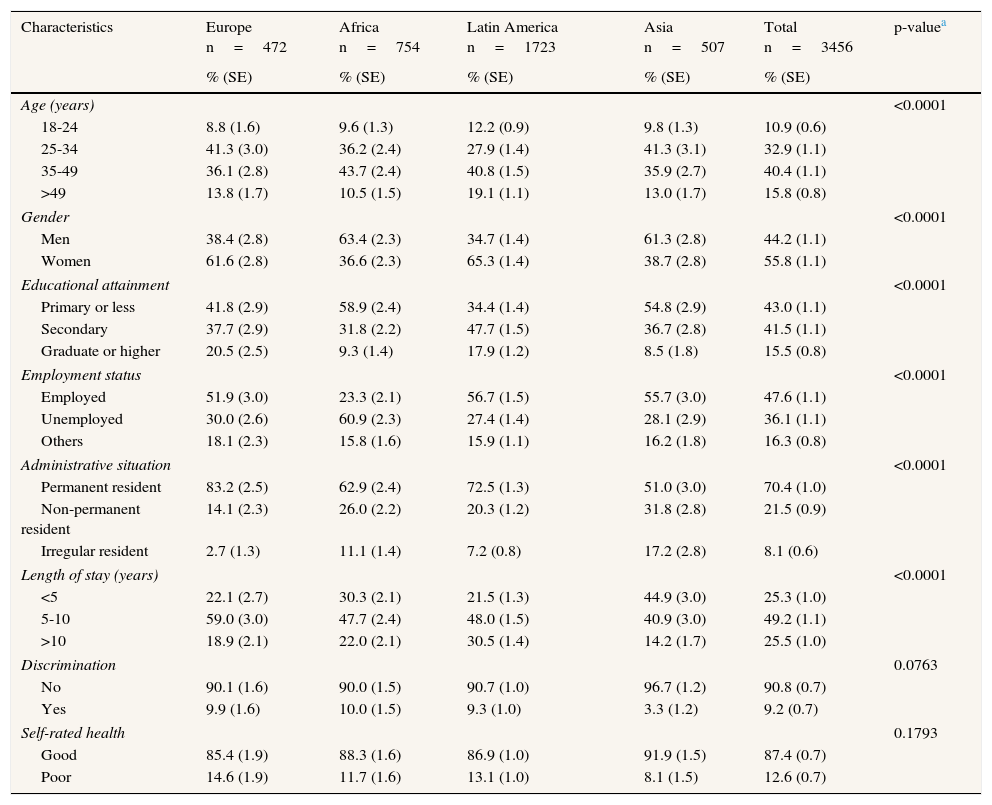
Distribution of selected characteristics for participants of the Foreign Immigrant Population Survey according to regions of origin: Basque Country, Spain, 2014.
| Characteristics | Europe n=472 | Africa n=754 | Latin America n=1723 | Asia n=507 | Total n=3456 | p-valuea |
|---|---|---|---|---|---|---|
| % (SE) | % (SE) | % (SE) | % (SE) | % (SE) | ||
| Age (years) | <0.0001 | |||||
| 18-24 | 8.8 (1.6) | 9.6 (1.3) | 12.2 (0.9) | 9.8 (1.3) | 10.9 (0.6) | |
| 25-34 | 41.3 (3.0) | 36.2 (2.4) | 27.9 (1.4) | 41.3 (3.1) | 32.9 (1.1) | |
| 35-49 | 36.1 (2.8) | 43.7 (2.4) | 40.8 (1.5) | 35.9 (2.7) | 40.4 (1.1) | |
| >49 | 13.8 (1.7) | 10.5 (1.5) | 19.1 (1.1) | 13.0 (1.7) | 15.8 (0.8) | |
| Gender | <0.0001 | |||||
| Men | 38.4 (2.8) | 63.4 (2.3) | 34.7 (1.4) | 61.3 (2.8) | 44.2 (1.1) | |
| Women | 61.6 (2.8) | 36.6 (2.3) | 65.3 (1.4) | 38.7 (2.8) | 55.8 (1.1) | |
| Educational attainment | <0.0001 | |||||
| Primary or less | 41.8 (2.9) | 58.9 (2.4) | 34.4 (1.4) | 54.8 (2.9) | 43.0 (1.1) | |
| Secondary | 37.7 (2.9) | 31.8 (2.2) | 47.7 (1.5) | 36.7 (2.8) | 41.5 (1.1) | |
| Graduate or higher | 20.5 (2.5) | 9.3 (1.4) | 17.9 (1.2) | 8.5 (1.8) | 15.5 (0.8) | |
| Employment status | <0.0001 | |||||
| Employed | 51.9 (3.0) | 23.3 (2.1) | 56.7 (1.5) | 55.7 (3.0) | 47.6 (1.1) | |
| Unemployed | 30.0 (2.6) | 60.9 (2.3) | 27.4 (1.4) | 28.1 (2.9) | 36.1 (1.1) | |
| Others | 18.1 (2.3) | 15.8 (1.6) | 15.9 (1.1) | 16.2 (1.8) | 16.3 (0.8) | |
| Administrative situation | <0.0001 | |||||
| Permanent resident | 83.2 (2.5) | 62.9 (2.4) | 72.5 (1.3) | 51.0 (3.0) | 70.4 (1.0) | |
| Non-permanent resident | 14.1 (2.3) | 26.0 (2.2) | 20.3 (1.2) | 31.8 (2.8) | 21.5 (0.9) | |
| Irregular resident | 2.7 (1.3) | 11.1 (1.4) | 7.2 (0.8) | 17.2 (2.8) | 8.1 (0.6) | |
| Length of stay (years) | <0.0001 | |||||
| <5 | 22.1 (2.7) | 30.3 (2.1) | 21.5 (1.3) | 44.9 (3.0) | 25.3 (1.0) | |
| 5-10 | 59.0 (3.0) | 47.7 (2.4) | 48.0 (1.5) | 40.9 (3.0) | 49.2 (1.1) | |
| >10 | 18.9 (2.1) | 22.0 (2.1) | 30.5 (1.4) | 14.2 (1.7) | 25.5 (1.0) | |
| Discrimination | 0.0763 | |||||
| No | 90.1 (1.6) | 90.0 (1.5) | 90.7 (1.0) | 96.7 (1.2) | 90.8 (0.7) | |
| Yes | 9.9 (1.6) | 10.0 (1.5) | 9.3 (1.0) | 3.3 (1.2) | 9.2 (0.7) | |
| Self-rated health | 0.1793 | |||||
| Good | 85.4 (1.9) | 88.3 (1.6) | 86.9 (1.0) | 91.9 (1.5) | 87.4 (0.7) | |
| Poor | 14.6 (1.9) | 11.7 (1.6) | 13.1 (1.0) | 8.1 (1.5) | 12.6 (0.7) | |
SE: standard error.
Descriptive statistics for sociodemographic characteristics, discrimination and self-rated health for the study population are presented in Table 1. Participants were mostly between the ages of 25 to 49 years (73.3%), women (55.8%), to report being employed (47.6%) and to have at least a secondary education (67%). Most participants are permanent residents (70.4%) and 49.2% have between 5 and 10 years residing in the Basque Country. Less than 10% reported any experience of discrimination whereas 12.6% reported their health as poor. When examining these variables across region of origin, participants from Latin America were more likely to be older than 34 years of age; those from Africa and Asia were more likely to be males; those from Europe have higher education; those from Africa are less likely to be employed; those from Europe are more likely to be permanent residents whereas those from Asia were less likely to be permanent residents (all p-values <0.001). Finally, discrimination and self-rated health were not associated with region of origin.
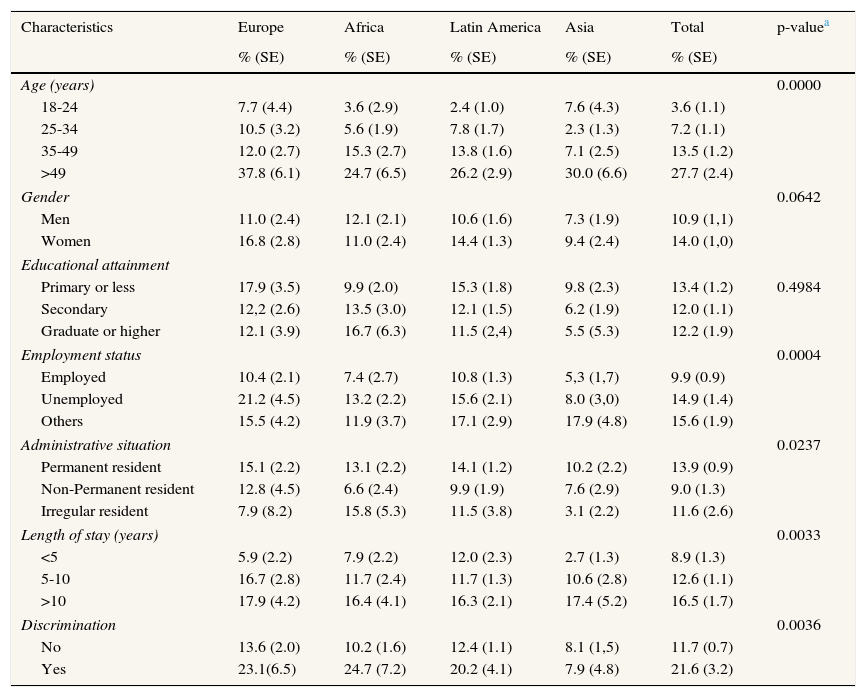
Table 2 shows the prevalence estimates for self-rated health for selected characteristics for the total population and according to region of origin. Poor self-rated health was more common among immigrants aged >49 years (27.7%), women (14%), those with less education (13.4%), unemployed (14.9%), permanent residents (13.9%) and with more than 10 years residing in Basque Country (16.5%). In addition, at least one in 5 immigrants reporting discrimination rated their health as poor (21.6%). These patterns were consistent across region of origin with few exceptions: among immigrants with an irregular resident status, the prevalence of poor self-rated health was more common from Africa (15.8%) and less common among those from Asia (3.1; p=0.024). Similarly, prevalence estimates were higher for those from Latin America (17.1%) and Asia (17.9%) reporting other employment arrangements (p <0.01). Finally, immigrants from Asia reporting not experience of discrimination were more likely to rate their health as poor as compared to their counterparts reporting discrimination (8.1 vs 7.9%; p=0.004). There was not association of gender and education with self-rated health across region of origin.
Prevalence estimates for poor self-rated health for selected characteristics for participants of the Foreign Immigrant Population Survey according to regions of origin: Basque Country, Spain, 2014.
| Characteristics | Europe | Africa | Latin America | Asia | Total | p-valuea |
|---|---|---|---|---|---|---|
| % (SE) | % (SE) | % (SE) | % (SE) | % (SE) | ||
| Age (years) | 0.0000 | |||||
| 18-24 | 7.7 (4.4) | 3.6 (2.9) | 2.4 (1.0) | 7.6 (4.3) | 3.6 (1.1) | |
| 25-34 | 10.5 (3.2) | 5.6 (1.9) | 7.8 (1.7) | 2.3 (1.3) | 7.2 (1.1) | |
| 35-49 | 12.0 (2.7) | 15.3 (2.7) | 13.8 (1.6) | 7.1 (2.5) | 13.5 (1.2) | |
| >49 | 37.8 (6.1) | 24.7 (6.5) | 26.2 (2.9) | 30.0 (6.6) | 27.7 (2.4) | |
| Gender | 0.0642 | |||||
| Men | 11.0 (2.4) | 12.1 (2.1) | 10.6 (1.6) | 7.3 (1.9) | 10.9 (1,1) | |
| Women | 16.8 (2.8) | 11.0 (2.4) | 14.4 (1.3) | 9.4 (2.4) | 14.0 (1,0) | |
| Educational attainment | ||||||
| Primary or less | 17.9 (3.5) | 9.9 (2.0) | 15.3 (1.8) | 9.8 (2.3) | 13.4 (1.2) | 0.4984 |
| Secondary | 12,2 (2.6) | 13.5 (3.0) | 12.1 (1.5) | 6.2 (1.9) | 12.0 (1.1) | |
| Graduate or higher | 12.1 (3.9) | 16.7 (6.3) | 11.5 (2,4) | 5.5 (5.3) | 12.2 (1.9) | |
| Employment status | 0.0004 | |||||
| Employed | 10.4 (2.1) | 7.4 (2.7) | 10.8 (1.3) | 5,3 (1,7) | 9.9 (0.9) | |
| Unemployed | 21.2 (4.5) | 13.2 (2.2) | 15.6 (2.1) | 8.0 (3,0) | 14.9 (1.4) | |
| Others | 15.5 (4.2) | 11.9 (3.7) | 17.1 (2.9) | 17.9 (4.8) | 15.6 (1.9) | |
| Administrative situation | 0.0237 | |||||
| Permanent resident | 15.1 (2.2) | 13.1 (2.2) | 14.1 (1.2) | 10.2 (2.2) | 13.9 (0.9) | |
| Non-Permanent resident | 12.8 (4.5) | 6.6 (2.4) | 9.9 (1.9) | 7.6 (2.9) | 9.0 (1.3) | |
| Irregular resident | 7.9 (8.2) | 15.8 (5.3) | 11.5 (3.8) | 3.1 (2.2) | 11.6 (2.6) | |
| Length of stay (years) | 0.0033 | |||||
| <5 | 5.9 (2.2) | 7.9 (2.2) | 12.0 (2.3) | 2.7 (1.3) | 8.9 (1.3) | |
| 5-10 | 16.7 (2.8) | 11.7 (2.4) | 11.7 (1.3) | 10.6 (2.8) | 12.6 (1.1) | |
| >10 | 17.9 (4.2) | 16.4 (4.1) | 16.3 (2.1) | 17.4 (5.2) | 16.5 (1.7) | |
| Discrimination | 0.0036 | |||||
| No | 13.6 (2.0) | 10.2 (1.6) | 12.4 (1.1) | 8.1 (1,5) | 11.7 (0.7) | |
| Yes | 23.1(6.5) | 24.7 (7.2) | 20.2 (4.1) | 7.9 (4.8) | 21.6 (3.2) | |
SE: standard error.
Perceived discrimination was most common among immigrants with at least 10 years (10.4%) and those unemployed (10.6%; p <0.05; data not shown). For region of origin, perceived discrimination was most common among European immigrants aged 18-24 (14.5%), with permanent resident status (11.2%) and unemployed (14.2%); African immigrants with irregular resident status (22.4%); and Asian immigrants with non-permanent resident status (7.4%; all p-values <0.05).
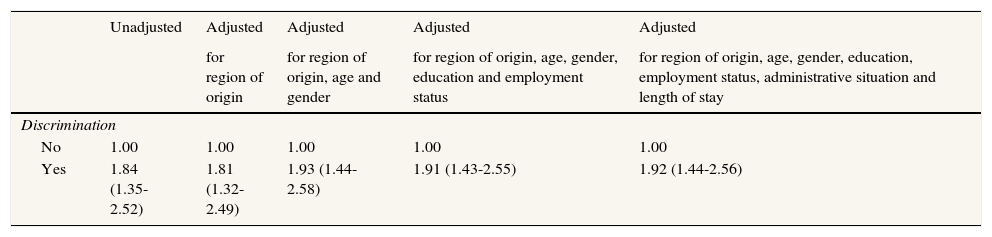
Participants reporting discrimination had 1.84 (95%CI: 1.35-2.52) higher probability of rating their health as poor when compared with their counterparts who do not report discrimination (Table 3). This association persists and slightly increases after adjustment for region of origin, age and gender (PR: 1.93; 95%CI: 1.44-2.58). Moreover, this association remained nearly unchanged when controlling for region of origin, age, gender, education, employment status, legal status, and length of stay in Basque Country (PR: 1.92; 95%CI: 1.44-2.56). Finally, this association did not vary with region of origin, age, gender or education (all p-values for the interactions >0.20).
Prevalence ratios unadjusted and adjusted with their 95%CI for poor self-rated health: Basque Country, 2014.
| Unadjusted | Adjusted | Adjusted | Adjusted | Adjusted | |
|---|---|---|---|---|---|
| for region of origin | for region of origin, age and gender | for region of origin, age, gender, education and employment status | for region of origin, age, gender, education, employment status, administrative situation and length of stay | ||
| Discrimination | |||||
| No | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 1.84 (1.35-2.52) | 1.81 (1.32-2.49) | 1.93 (1.44-2.58) | 1.91 (1.43-2.55) | 1.92 (1.44-2.56) |
Our finding of a positive association between perceived discrimination and self-rated health is consistent with studies in other countries1,10,11,27,28 suggesting that discrimination may be an important factor explaining the differences in health within the immigrant population and relative to the native population. In Spain two studies showed that immigrants reporting perceived discrimination were almost twice more likely to rate their health as poor compared with their counterparts who did not report such experience.19,20 Our findings concurred with these studies as we found a similar association between perceived discrimination and self-rated health.
It is worth underscoring the low prevalence of perceived discrimination in our study (<10% with range of 10% to 3.3% across immigrants groups) compared to studies conducted in Spain19–21,23 and in other European countries.11,13 The reasons for the low prevalence could be both methodological and contextual. On the one hand, evidence on social or health population surveys shows a lower response rate among the most excluded immigrant populations, specifically those with less education and lower socioeconomic position,29 leading to selection bias of this population.30 The low participation rate in surveys with random sampling of the most excluded immigrants population may explain the prevalence of perceived discrimination observed in the Foreign Immigrant Population Survey compared to the prevalence of discrimination observed in surveys using convenience samples (∼40%).13,20,23 It is possible that these studies findings may represent a selection bias and those perceiving discrimination are overrepresented. On the other hand, the Basque Country region has a lower rate of immigration than other Spanish regions and other countries where this association has been studied; the latter may afford less hostility of the local population towards immigration, with an index of tolerance towards immigration relatively high without major changes in the last ten year.31 In addition, the Basque Country has been the only autonomous community with social and health policies maintained or improved during the crisis, and policies with greater social protection than other autonomous communities.32,33 Specifically and in terms of access to the public health system, the Basque Country has implemented measures to alleviate the exclusion of illegal immigrants posed by the Royal Decree Law 16/2012 implemented from the state government in 2012. Thus, the effects of a major tolerance towards immigration from the native population and the integration of anti-discriminatory social policies may help explain the lower perception of discrimination in the Basque Country compared with similar studies in Spain19,21 and Europe.10
While discrimination seems to affect a small proportion of immigrant population, we found an association between perceived discrimination and self-rated health regardless of region of origin, age, gender and education. These findings, consistent with those found in Germany11 and the US,27 showed the same effect of discrimination among immigrants or ethnic groups, despite a different level of exposure to discrimination. Thus, the similarities in response to discrimination are more important than cultural differences, gender and educational attainment, or other characteristics. These results point to the Importance of policies aimed at directly reducing discrimination such as promotion of long-term residence and family reunion policies which are associated with lower levels of perceived discrimination.34 In fact, a European study examining the association between discrimination and self-rated health in different types of countries according to their integration policies (exclusionist, assimilationist and inclusive), stated the importance of social and cultural expression of identity in the public sphere to avoid perceived discrimination.9 Thus, integration policies may have direct impact to reduce health disparities between the immigrant and native populations.
There are several limitations that may have affected our results. First, this is a cross-sectional study precluding from establishing a temporal relationship between exposure and outcome. Second, although discrimination is a multidimensional phenomenon, this study used a single-item question to measure discrimination making it difficult to clarify the role of the different forms of discrimination on health and related factors. Finally, given the sample size, we could not disaggregate at the countries of birth level and only large regions of origin could be considered during the analyses. However, and once excluded the immigrant population from the developed countries, this disaggregation has allowed us to examine whether the association between discrimination and self-rated health was different across the large regions of origin studied, although the diversity within each region could masked and diluted the value of origin in this association. However, our use of, at least, the main regions of origin is important as most studies have examined the immigrant population as a whole9,19,20,24 or have focused only on immigrants from particular countries.13,22 Finally and most importantly, despite these limitations, we used data from a representative survey of the immigrant population, conducted by the Basque Country Government, including information on the health status of the immigrant population and the social determinants of health inequalities.
Our study shows that among immigrants, those perceiving experiences of discrimination were almost twice more likely to rate their health as poor compared with their counterparts who do not report similar experiences. This association did not change with region of origin, age, gender or educational attainment. This study has the potential to advance our knowledge on the detrimental effects of discrimination on health of immigrant populations underscoring the importance of implementing inclusive policies to eliminate individual and institutional discrimination. Such policies may allow labor market mobility, access to health system, family reunion, long-term residence, access to nationality and political rights to promote a sentiment of belonging and an easy integration for the immigrant population.34,35 These policies may contribute to reduce health inequalities between the immigrant and native populations in an increasingly diverse society as a consequence of the recent flux of immigrants. In fact, in Spain, the immigrant population comprises one of the most vulnerable groups when it comes to the effects of the economic crisis. The latter may affect living conditions, increase discrimination in the job market as well as issues with legal status and citizenship. In addition, in the years to come, the tightening of conditions for access to certain benefits and public services such as health care could have very negative consequences on the health of the immigrant population. This new situation will need to support social policies that allow improving the living conditions of the immigrant population.
Recent evidence shows that discrimination is associated with poorer health outcomes, including self-rated health in immigrant population. However, the evidence is not consistent regarding the effect of place of origin, gender, age and education on the association between discrimination and poor health. Moreover, most of these studies used convenience samples or aggregate immigrants regardless of country or region of origin into a single category.
What does this study add to the literature?This study shows that among immigrants, those perceiving experiences of discrimination were almost twice more likely to rate their health as poor. Moreover, this association did not vary with region of origin, age, gender, or educational attainment. These findings indicate the importance of implementing inclusive to eliminate individual and institutional discrimination. These policies could prevent negative consequences on the health of immigrants, and thus, to reduce health inequalities between the immigrant and native populations.
Julia Bolívar.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsE. Rodriguez-Alvarez and L.N. Borrell were responsible for the study concept and design. E. Rodriguez-Alvarez and Y. González-Rábago wrote the first draft of the manuscript. N. Lanborena and L.N. Borrell were responsible for conceptualizing and designing the analysis as well as interpreting the results. All authors critically reviewed and approved the final version of the article.
AcknowledgementsThe authors acknowledge Luis Sanzo and Xabier Aierdi (Department of Employment and Social Policies of the Basque Government, Spain) for providing the data for this study.
FundingThis study was supported by the University of the Basque Country UPV/EHU (project EHU14/55].
Conflicts of interestNone.











