




Birthweight by gestational age charts enable fetal growth to be evaluated in a specific population. Given that maternal profile and obstetric practice have undergone a remarkable change over the past few decades in Spain, this paper presents new Spanish reference percentile charts stratified by gender, parity and type of delivery. They have been prepared with data from the 2010–2014 period of the Spanish Birth Statistics Bulletin.
MethodsReference charts have been prepared using the LMS method, corresponding to 1,428,769 single, live births born to Spanish mothers. Percentile values and mean birth weight are compared among newborns according to gender, parity and type of delivery.
ResultsNewborns to primiparous mothers show significantly lower birthweight than those born to multiparous mothers (p<0.036). Caesarean section was associated with a substantially lower birthweight in preterm births (p<0.048), and with a substantially higher birthweight for full-term deliveries (p<0.030). Prevalence of small for gestational age is significantly higher in newborns born by Caesarean section, both in primiparous (p<0.08) and multiparous mothers (p<0.027) and, conversely, the prevalence of large for gestational age among full-term births is again greater both in primiparous (p<0.035) and in multiparous mothers (p<0.007).
ConclusionsResults support the consideration of establishing parity and type of delivery-specific birthweight references. These new charts enable a better evaluation of the impact of the demographic, reproductive and obstetric trends currently in Spain on fetal growth.
Las tablas de peso al nacer por edad gestacional permiten evaluar el crecimiento fetal en una población específica. Dado que el perfil materno y la práctica obstétrica han experimentado un sustancial cambio en las últimas décadas en España, este trabajo propone nuevas tablas de referencia de percentiles estratificadas por sexo, paridad y tipo de parto, elaboradas con los datos del periodo 2010-2014 del Boletín Estadístico de Partos.
MétodosLas curvas de referencia han sido elaboradas mediante el método LMS, correspondientes a 1.428.769 nacidos vivos de partos simples y madres españolas. Se comparan los valores por percentiles y la media del peso al nacer, por sexo, paridad y tipo de parto.
ResultadosLos nacidos de madres primíparas muestran un peso menor que los nacidos de multíparas (p<0,036). Los nacidos pretérmino por cesárea tienen un peso menor que los nacidos pretérmino por parto vaginal (p<0,048), mientras que ocurre lo contrario en los nacidos a término (p<0,030). La prevalencia de nacidos pequeños para la edad gestacional es mayor entre los nacidos por cesárea de madres tanto primíparas (p<0,08) como multíparas (p<0,027), y la prevalencia de nacidos grandes para la edad gestacional es mayor entre los nacidos a término de madres tanto primíparas (p<0,035) como multíparas (p<0,007).
ConclusionesLos resultados apoyan establecer referencias de peso al nacer por paridad y tipo de parto. Estas nuevas curvas permiten una mejor evaluación del impacto de las actuales tendencias demográficas, reproductivas y obstétricas en España sobre el crecimiento fetal.
Fetal growth and birth outcome are associated with perinatal survival and health, with the patterns of postnatal growth, and with differential risk for cognitive, metabolic and cardiovascular disease later in life.1 Birthweight and gestational age are the main perinatal indicators that support this relationships between fetal and postnatal stages, as both variables (i.e. reduced birthweight and/or preterm births) have been associated with epigenetic, hormonal and metabolic regulation mechanisms affecting health throughout life cycle.2 Birthweight for gestational age charts allow assessing the prevalence of small for gestational age (SGA) newborns, those born with a birthweight under 10th percentile for their gestational age. However, fetal growth charts prepared for one specific population are not appropriate for evaluating growth in different populations as clinically important differences in both the mean birthweight and percentile values may be found.3 These differences are due to biosocial characteristics of the population used as the reference and the study methodology. Thus, it is important to differentiate between reference growth curves and standard growth curves, as Rao and Tompkins4 remember: reference curves show the fetal growth of a particular population at a specific time, while standard curves show how a newborn should grow according to an ideal healthy growth, and hence are of prescriptive nature.
Different growth charts by gestational age and sex have been designed for Spanish newborns based on hospital data.5–9 Some of these charts are still widely used in the Spanish public health system for assessing birth outcome and infant growth although Spain has officially adopted the new WHO standards for term births and up to five years old children.10 Most recently, Ramos et al.11 and González-González et al.12 have proposed models for calculating optimal fetal and neonatal weight curves from population and hospital data respectively, and García-Muñoz Rodrigo et al.13 have published the first growth standards for very preterm Spanish newborns (22-28 weeks) using data from 62 hospitals. Most of these charts were prepared without differentiating parity and type of delivery. However, parity is a well-recognized predictor of infant birthweight, with infants born to primiparous women registering significantly lower birthweight and higher prevalence of intrauterine growth restriction (IUGR).14 At the same time, the increasing rates of induced deliveries and Cesarean sections (CS) before week 37 has been associated with the increased prevalence of preterm births with extremely low weight in developed countries.15,16
The profile of Spanish (national) mothers has undergone a significant change over the past decades, with a sustained increase in the percentage of mothers who start reproducing at later ages, as well as in the rates of obstetric interventions in general, and CS deliveries in particular.17 From 2008 onwards the economic crisis is strengthening these trends,18 specifically the growing predominance of primiparous mothers of ever-increasing age. According to the latest available data,19 54.3% of Spanish mothers are primiparous with an average age for first maternity of 31.06 years, while the rate of CS is 25.2% —a figure that is double that recommended by WHO20—, with higher rates in private hospitals and in public hospitals with a lower technological level.21 As proposed for other European countries,22 these trends in maternal profile and obstetric practices might be contributing towards trends of lowering mean birthweight and increasing prevalence of low birth weight (LBW: birthweight under 2,500 grams) described in Spain.17 In this context, to stablish and compare charts of birthweight by parity and type of delivery may contribute both to a fitter evaluation of the impact of these trends on gestational growth and birth outcome in Spain, and to a greater understanding of the causes underlying the sustained increase in the rate of CS in the country.
With these aims, using data from the Spanish Birth Statistics Bulletin for the period 2010-2014, the aim of this study is to prepare new reference charts of birthweight by gestational age in Spain, stratified by sex, parity and type of delivery.
MethodsData and final sampleThe percentile tables and charts presented in this study have been prepared with cross-sectional data from the period 2010-2014 of the Spanish Birth Statistics Bulletin (BEP, Boletín Estadístico de Partos), the compulsory civil registration of all births whatever the nationality or legal status of residence of the parents provided annually by the Spanish National Institute of Statistics as microdata files. The process of data collection and its implications both for the quality and interpretation of the epidemiological results derived from this source have been evaluated by Juárez,23,24 and Río et al.25 Validation studies have concluded that data provided by the Spanish Birth Statistics Bulletin are quite reliable (κ=0.74 for gestational age, and κ=0.88 for birthweight) when compared with hospital birth data, although misreporting was significantly higher among immigrants.23 Besides this problem, newborns from immigrant mothers (n=419,161, 18.9% of all live births) have been excluded due to their relevant contribution to national natality as well as to the notorious differences in origin, lifestyles, reproductive behaviour and birth outcome among the main groups of foreign mothers in Spain.26 Therefore, percentile tables and charts proposed should apply only to Spanish mothers. 4.1% (n=71,435) of the Spanish mothers were originally immigrants that obtained the Spanish citizenship, and 2.9% (n=50,098) have a foreign husband or steady partner.
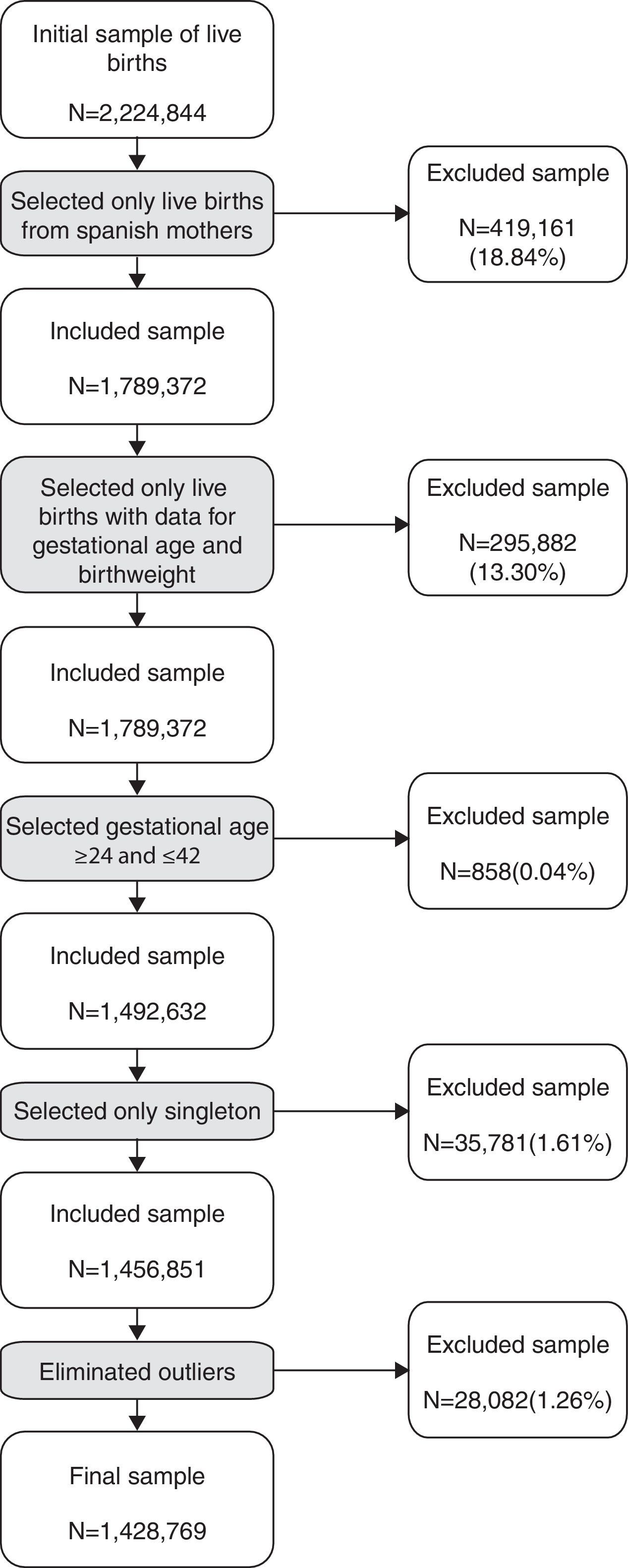
Figure 1 shows the process of selection of final sample. First, among newborns from Spanish mothers, stillbirths (n=419,161, 18.8%) were excluded. Among live births, newborns without data on gestational age and birthweight (n=295,882, 13.3% of all live births) were also eliminated, as well as those born at gestational ages before 24 and after 42 weeks (n=858, 0.0%), and from multiples pregnancies (n=35,781, 1.6%). Finally, implausible data were also eliminated with outlier limits set at ±1.5 standard deviation (SD). Final sample includes 1,428,769 live births from singleton deliveries of Spanish mothers (74.4%, n=1,062,319 by vaginal delivery, and 25.6%, n=366,450 by CS delivery), corresponding to 64.2% (n=2,224,844) of the total live births born in Spain in 2010-2014, and to 79.8% (n=1,789,372) of those from Spanish mothers. Final sample does not differ from the excluded data in maternal profile (age at birth, and educational level and occupation), although the rate of primiparity is slightly higher (54.9% compared to 52.5%, respectively; p<0.001) and the rate of CS deliveries slightly lower (25.6% and 26.5, respectively; p<0.001).
Statistical analysis
Percentile tables and curves by sex, parity (primiparous or multiparous mothers) and type of delivery (vaginal or by CS delivery) were prepared according to the LMS method.27 The LMS method provides three curves for each percentile chart. The first is curve L (λ), which results from non-linear transforming of birthweight, so this variable follows a normal distribution. The second curve, M (μ), corresponds to the median (percentile 50) or average as the distribution of the variable of interest now has a Gaussian distribution due to adjustment for curve L. The last curve, S (σ), corresponds to the coefficient of variation. To obtain parameters λ, μ and σ, L, M and S curves were adjusted by polynomic regression thus the curves obtained are those which best represent an adjustment of these parameters that allow a graphic representation of percentile charts and the calculation of exact z-scores (Z) for any value. Formula 1 allows calculating the values for each percentile:
being C the birthweight of a percentile, L, M and S are the value of these parameters given in Tables I-VIII of the online Appendix of this article for a specific gestational age, and Z the corresponding z-score for this percentile.
Birthweight charts and curves corresponding to 3rd, 10th, 50th, 90th and 97th percentiles according to parity, type of delivery and sex of the newborn are shown in Tables I-VIII and Figures I-VIII of the online Appendix of this article. From the SD values of the mean included in the tables, STATA software v.12 allows assessing the differences in mean birthweight (50th percentile values) by gestational age for both sexes according to parity and type of delivery. The SD of mean birthweight for each gestational age was calculated using formula 2:

Besides, formula 3 allows obtaining the z-score of a birthweight referred to a reference curve in order to assess the prevalence of SGA and Large for Gestational Age (LGA) by parity and type of delivery:
being X the weight in grams.
For each sex, the reference curve chosen is that established for newborns delivered vaginally and to primiparous mothers (Tables I and III of the online Appendix of this article).
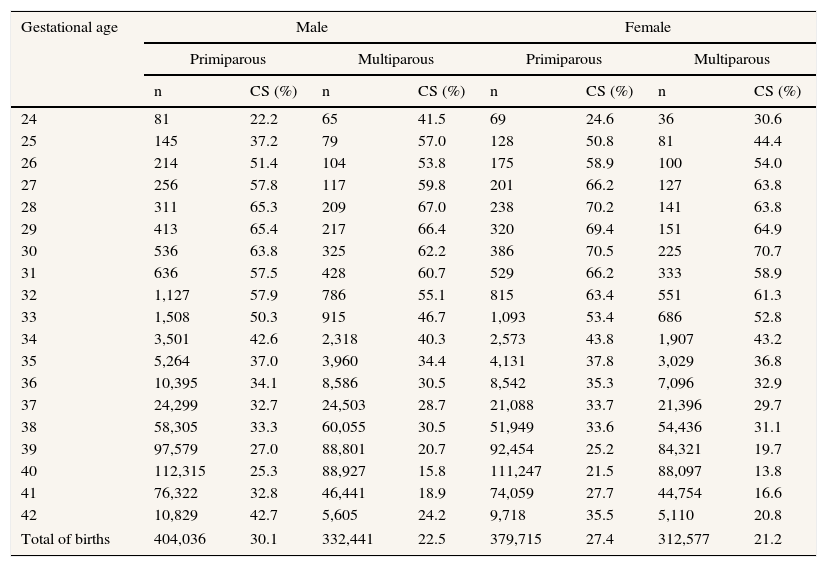
ResultsShown in Table 1 are the number of total births (N) and prevalence of CS delivery by gestational age, sex of the newborn, and parity. The highest rates of CS deliveries occurred between weeks 28 and 32, and then again after week 40, both in primiparous and multiparous mothers. The total rate of CS deliveries was significantly higher for primiparous than for multiparous mothers (28.8% and 21.8% respectively; χ2=8,896.015; d.f.=1; p<0.001, both sexes considered). The rate of CS was significantly higher among primiparous mothers both in preterm births (males: χ2=53.211, d.f.=1, p<0.001; and females: χ2=29.557; d.f.=1; p<0.001) and in term births (males: χ2=5,492.929; d.f.=1; p<0.001; and females: χ2=3,495.540, d.f.=1, p<0.001).
Number of total births and prevalence of Cesarean section deliveries in the study population (data from Spanish Birth Statistics Bulletin, single live births, Spanish mothers, 2010-2014).
| Gestational age | Male | Female | ||||||
|---|---|---|---|---|---|---|---|---|
| Primiparous | Multiparous | Primiparous | Multiparous | |||||
| n | CS (%) | n | CS (%) | n | CS (%) | n | CS (%) | |
| 24 | 81 | 22.2 | 65 | 41.5 | 69 | 24.6 | 36 | 30.6 |
| 25 | 145 | 37.2 | 79 | 57.0 | 128 | 50.8 | 81 | 44.4 |
| 26 | 214 | 51.4 | 104 | 53.8 | 175 | 58.9 | 100 | 54.0 |
| 27 | 256 | 57.8 | 117 | 59.8 | 201 | 66.2 | 127 | 63.8 |
| 28 | 311 | 65.3 | 209 | 67.0 | 238 | 70.2 | 141 | 63.8 |
| 29 | 413 | 65.4 | 217 | 66.4 | 320 | 69.4 | 151 | 64.9 |
| 30 | 536 | 63.8 | 325 | 62.2 | 386 | 70.5 | 225 | 70.7 |
| 31 | 636 | 57.5 | 428 | 60.7 | 529 | 66.2 | 333 | 58.9 |
| 32 | 1,127 | 57.9 | 786 | 55.1 | 815 | 63.4 | 551 | 61.3 |
| 33 | 1,508 | 50.3 | 915 | 46.7 | 1,093 | 53.4 | 686 | 52.8 |
| 34 | 3,501 | 42.6 | 2,318 | 40.3 | 2,573 | 43.8 | 1,907 | 43.2 |
| 35 | 5,264 | 37.0 | 3,960 | 34.4 | 4,131 | 37.8 | 3,029 | 36.8 |
| 36 | 10,395 | 34.1 | 8,586 | 30.5 | 8,542 | 35.3 | 7,096 | 32.9 |
| 37 | 24,299 | 32.7 | 24,503 | 28.7 | 21,088 | 33.7 | 21,396 | 29.7 |
| 38 | 58,305 | 33.3 | 60,055 | 30.5 | 51,949 | 33.6 | 54,436 | 31.1 |
| 39 | 97,579 | 27.0 | 88,801 | 20.7 | 92,454 | 25.2 | 84,321 | 19.7 |
| 40 | 112,315 | 25.3 | 88,927 | 15.8 | 111,247 | 21.5 | 88,097 | 13.8 |
| 41 | 76,322 | 32.8 | 46,441 | 18.9 | 74,059 | 27.7 | 44,754 | 16.6 |
| 42 | 10,829 | 42.7 | 5,605 | 24.2 | 9,718 | 35.5 | 5,110 | 20.8 |
| Total of births | 404,036 | 30.1 | 332,441 | 22.5 | 379,715 | 27.4 | 312,577 | 21.2 |
n: number of total births; CS: Cesarean section.
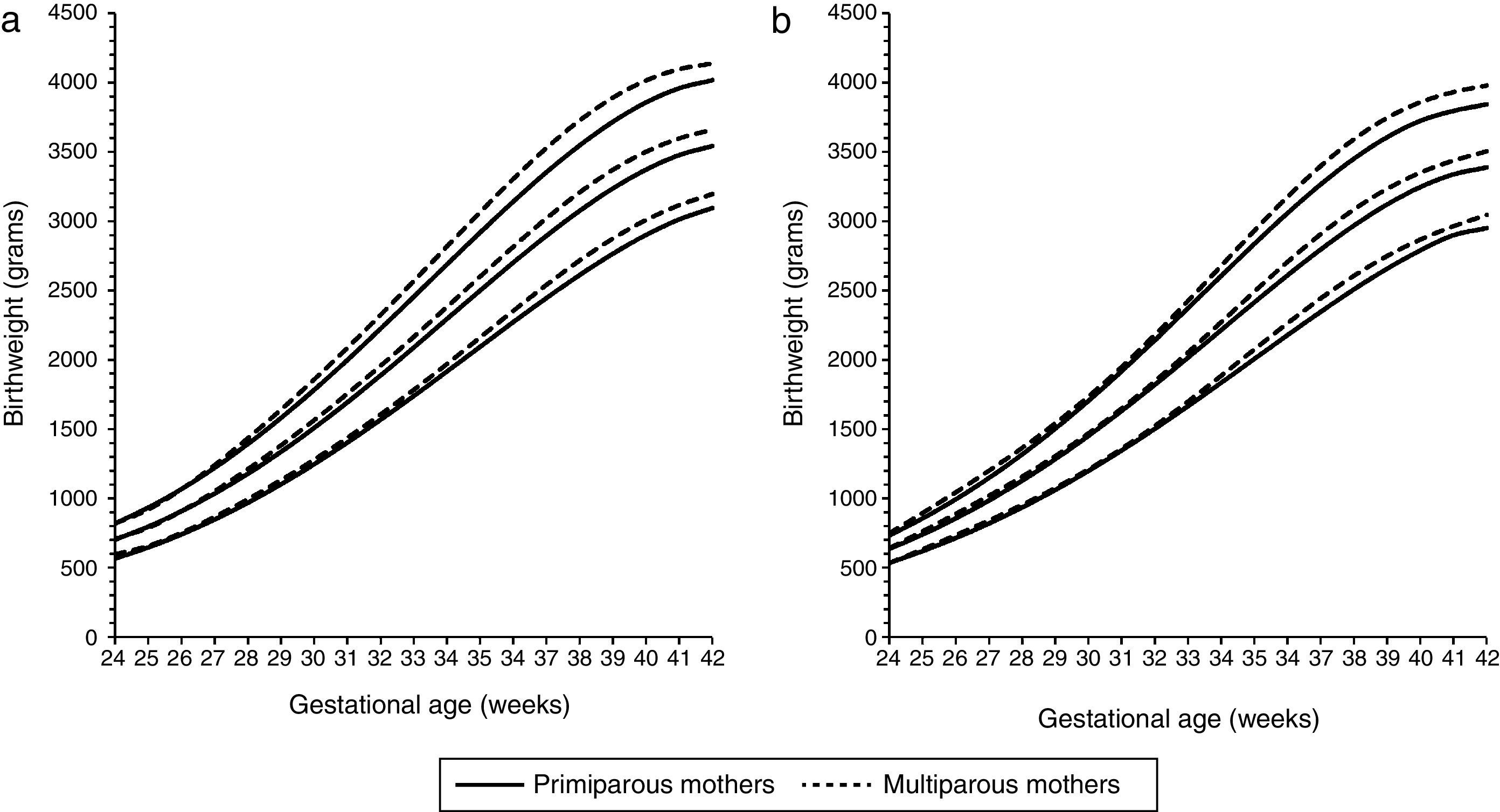
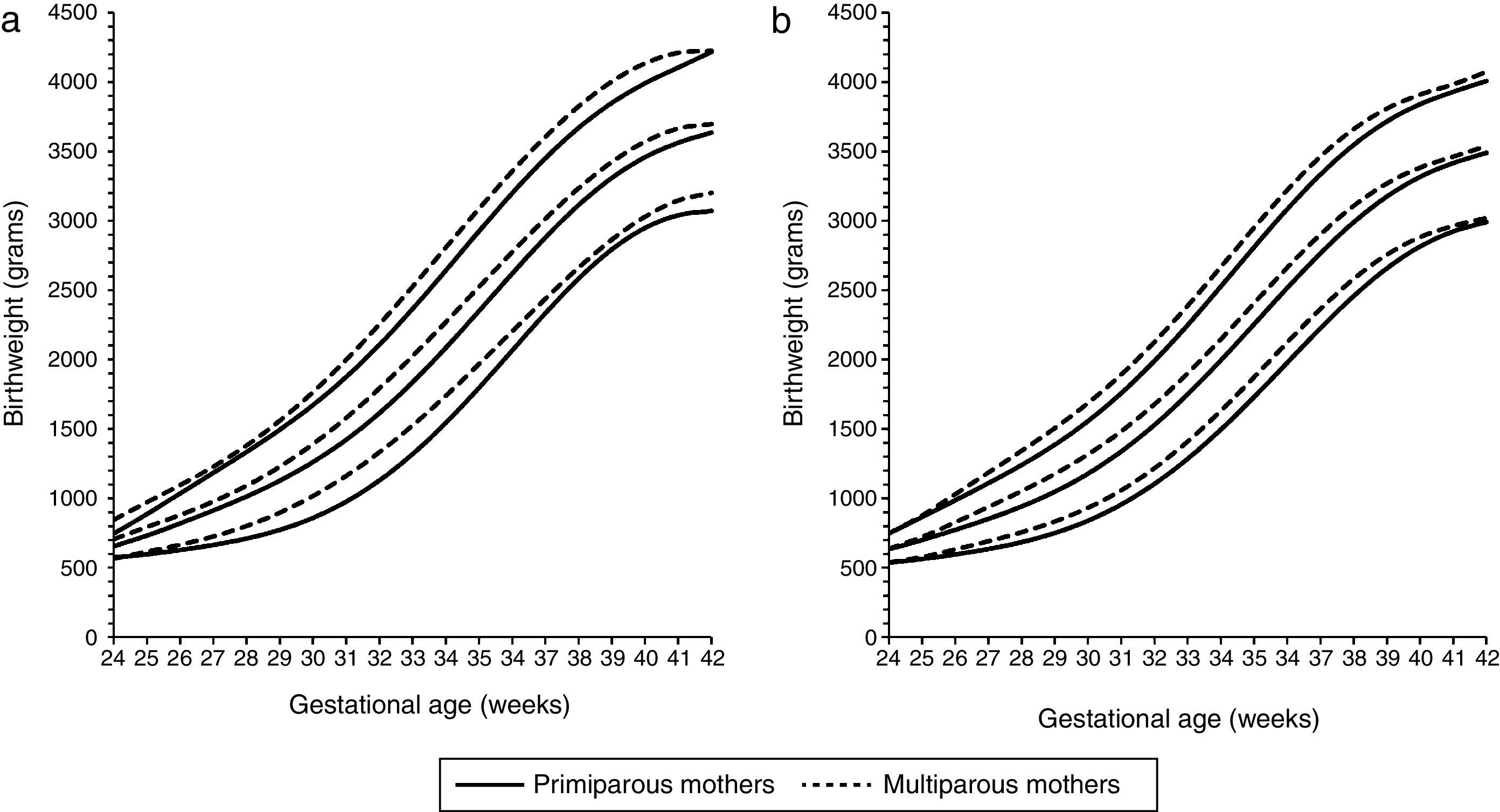
Tables I-VIII (and Figures I-VIII) of the online Appendix of this article present the percentile values and L, M and S parameters proposed for evaluating birthweight by gestational age, sex, parity and type of delivery in newborns of Spanish mothers. Based on these data, Figures 2 and 3 present the birthweight charts (10th, 50th and 90th percentiles) for newborns to primiparous and multiparous women according to sex and type of delivery. Independently of sex and type of delivery, the mean birthweight (50th percentile) of newborns to primiparous mothers was significantly lower than that of newborns to multiparous mothers (from gestational age 30 weeks in males and 34 weeks in females born by vaginal deliveries, respectively, and from 25 and 26 weeks, respectively, in those born by CS deliveries: p<0.036; Tables IX-XII of the online Appendix).


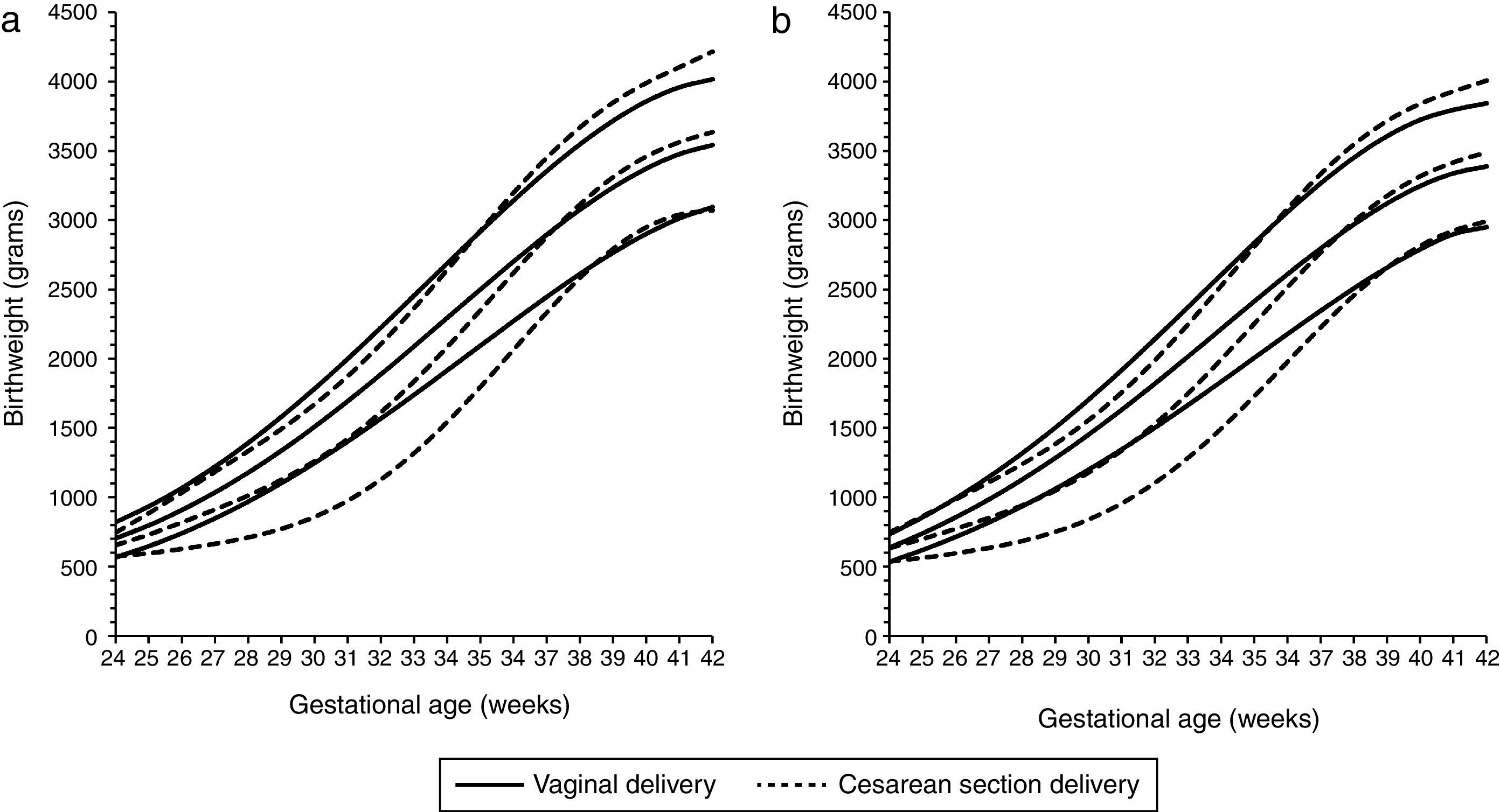
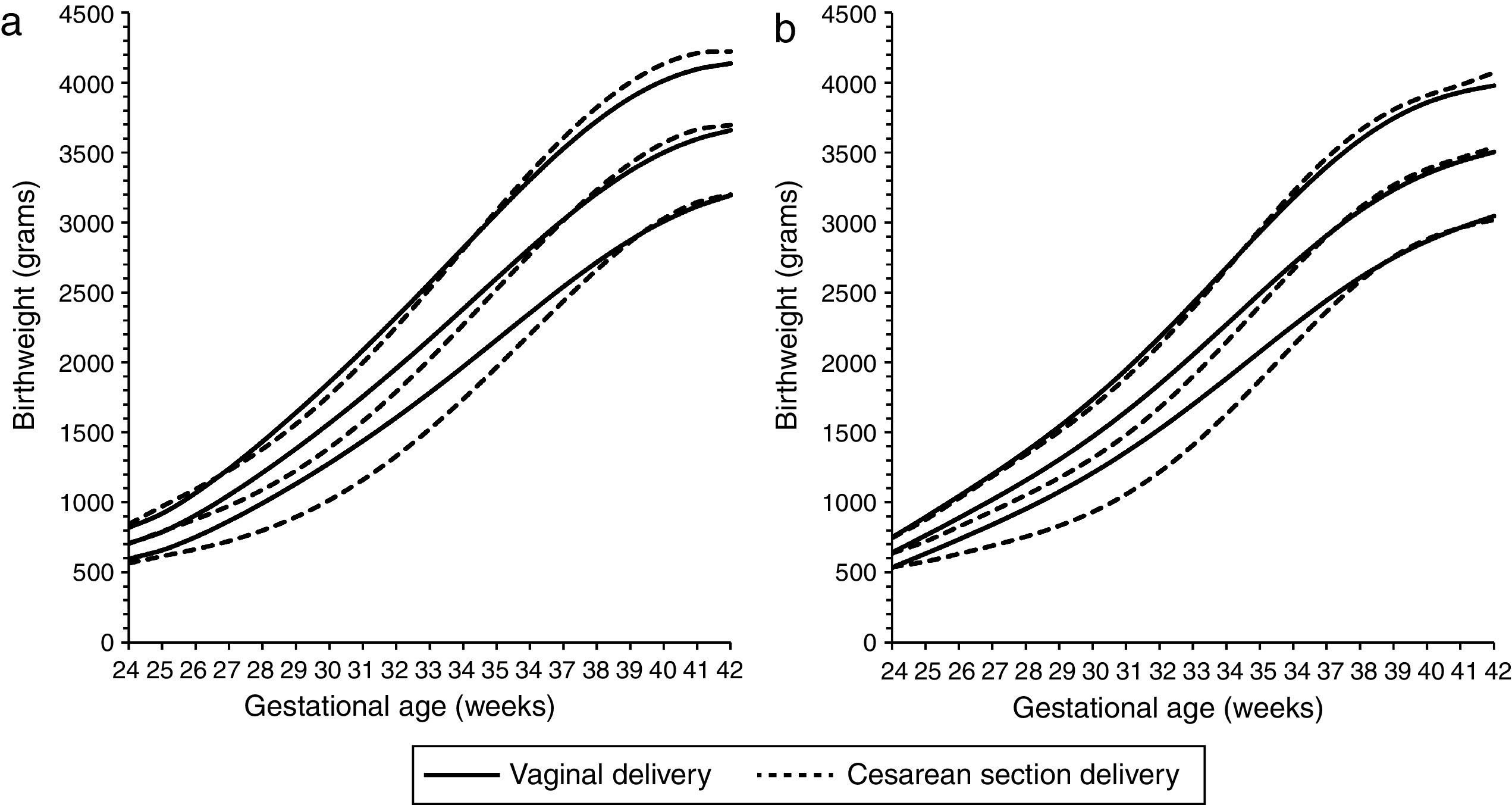
Likewise, Figures 4 and 5 show the birthweight charts of newborns delivered vaginally and by Cesarean section according to parity and sex. Independently of sex and parity, mean birthweight of preterm newborns delivered by CS was significantly lower than those delivered vaginally (from 24 to 37 weeks in males, and from 25 to 37 weeks in females to primiparous mothers; and from 27 to 36 weeks in males, and from 26 to 36 weeks in females born to multiparous women: p<0.048; Tables XIII-XVI of the online Appendix). Accordingly, the prevalence of SGA was also significantly higher among newborns born at early gestational ages by CS delivery compared with those delivered vaginally, both in primiparous (from 26 to 38 weeks of gestation in both sexes: p<0.08; Tables XVII and XIX of the online Appendix) as well as in multiparous mothers (from 28 to 37 weeks of gestation in both sexes: p<0.027; Tables XXI and XXIII of the online Appendix). Conversely, Figures 4 and 5 also show that mean birthweight of term newborns delivery by Cesarean section was greater than those born vaginally (from 38 to 42 weeks in both sexes and parities: p values <0.030; Tables XIII-XVI of the online Appendix). As expected, in these gestational ages prevalence of LGA was higher in newborns born by CS delivery, again both among primiparous (from 36 to 42 weeks in males, and from 37 to 42 weeks in females: p<0.035; Tables XVIII-XX of the online Appendix) and multiparous mothers (from 37 to 42 weeks in males, and from 38 to 42 weeks in females: p<0.007; Tables XXII-XXIV of the online Appendix).

Birthweight by gestational age 10th, 50th and 90th percentiles for males (a) and females (b) to primiparous mothers by vaginal delivery (solid lines) and Cesarean section delivery (dotted lines). (Data from Spanish Birth Statistics Bulletin, single live births, Spanish mothers, 2010-2014).

Birthweight by gestational age 10th, 50th and 90th percentiles for males (a) and females (b) to multiparous mothers by vaginal delivery (solid lines) and Cesarean section delivery (dotted lines). (Data from Spanish Birth Statistics Bulletin, single live births, Spanish mothers, 2010-2014).
This paper presents the first nationally representative reference tables and charts for birthweight by gestational age and sex according to parity and type of delivery for Spanish population. These tables allow calculating the exact percentile or z-score of the newborn depending on parity, type of birth and newborn sex due to the inclusion of L, M and S values. Our results support the suggestion by Hinkle et al.28 of establishing parity-specific birthweight references. Live births of both sexes and all gestational ages born to primiparous mothers showed significantly lower birthweight than those of multiparous mothers, as Liu et al.29 have recently confirmed for Chinese population. Primiparity determines a reduction in birthweight and is a well-known risk factor for greater incidence of LBW and IUGR, when other maternal characteristics are controlled, including type of delivery.30 The main biological mechanism proposed as an explanation of the effect of parity on fetal growth is a lesser vascular uteroplacental capacity in primiparous mothers, which reduces the supply of oxygen and nutrients to the fetus.31,32 There are also structural factors for primiparous mothers (such as a less intra-uterine space in the first pregnancy than in later pregnancies) which also tend to reduce birthweight.33
Results also confirm that newborns delivered by CS showed more variation of weight at birth, depending on gestational age, than those born vaginally, as previous research has shown.34,35 CS deliveries were associated with a substantial, significant reduction in birthweight among earlier gestational ages of both sexes and all maternal parities in such a way that the distribution of the 10th percentile is skewed towards lower birthweight among preterm live births delivered by CS compared with those born vaginally. As extreme low birthweight among preterm births is associated with increased risk of neonatal death,36 the rising rates of CS deliveries at early gestational ages in developed countries have been associated with improved perinatal survival,15,37 a positive trend supported by the dramatic technological breakthroughs in Perinatology and Neonatology of last decades. However, this obstetric trend does not explain the dramatic increase in CS deliveries in Spain, given that the most of this type of delivery took place among gestations of 37 weeks or more —over 90%, in both primiparous and multiparous mothers (as can be confirmed from Table 1). Certainly, the prevalence of LGA newborns was higher in newborns born by CS delivery compared with those born vaginally, both among primiparous and multiparous mothers, although not as heavily as the previously described increase in the prevalence of SGA among preterm live births, as figures 4 and 5 clearly show; likewise, although the mean birth weight is significantly higher among term newborns born by CS delivery compared with those born vaginally, the differences are very small (Tables I-VIII of the online Appendix). In summary, the high rates of CS deliveries registered in Spain cannot be explained by a high prevalence of dystocia by macrosomia or cephalopelvic disproportion, neither for primiparous nor for multiparous mothers. As Bernis et al.17 and Redondo et al.21 consider, research on non-clinical factors affecting delivery could clarify the ever-growing rate of CS in Spain, an issue that goes beyond the objectives of this paper. Meanwhile, the utilization of neonatal charts for birthweight taking into account type of delivery is highly recommended to evaluate the effect that the increase in the rate of CS deliveries during the last two decades in Spain would have on the assessment of fetal growth if type of delivery is not considered, particularly in order to avoid both underestimating the prevalence of SGA in preterm births and overestimating the prevalence of LGA in term births among those delivered vaginally.38,39
Limitations of the studyThe percentile tables presented here are based on cross-sectional data from the Spanish Birth Statistics Bulletin. Nevertheless, the use of these percentile tables and charts are restricted to newborns from Spanish mothers, as those born from foreign mothers were excluded. Additionally, some critical considerations can be formulate on the origin and quality of the data. Gestational age is calculated on the last menstrual period (LMP) in completed weeks. Our findings may stand in contrast with those based on longitudinal or cross-sectional ultrasound measurements recorded during gestation, which improve the accuracy of gestational age assignment and allow calculating an estimated fetal weight (EFW). Compared with early ultrasound scanning estimation of gestational age, LMP date more often overestimates the true length of gestation, underestimating the prevalence of preterm birth and, consequently, increasing the rate of newborns incorrectly diagnosed as growth retarded.40 However, EFW charts do not avoid misclassification of gestational age, which results in the opposite effect of lowering birthweight percentiles among preterm births and increasing the percentile values late in gestation.41 Besides these methodological considerations, it is necessary to remember that the pattern of intrauterine growth for term births does not necessarily have to be the same as for preterm births, as spontaneous preterm birth has been significantly associated with IUGR.42 Despite these limitations and differences between methods, the reference tables and charts for birthweight by gestational age at birth are easier and cheaper to establish, allowing evaluate temporal trends in fetal growth and weight at birth (including the prevalence of SGA and LGA) associated with changes in maternal age, parity, and type of delivery, factors which have registered notable changes in Spain over the last decades, as well as in other developed countries.
ConclusionThe evaluation of fetal growth and its secular trends are important for human biologists, epidemiologists, gynaecologists and public health professionals, as birth weight is related with perinatal survival and health, with the patterns of postnatal growth, and with differential risk for metabolic and cardiovascular disease later in life. Because the main environmental factors involved in its variability (maternal profile and protocols of delivery) have been rapidly changing during the last decades in Spain as in other developed countries, there is an increasing agreement that the temporal tendencies of fetal growth and birth outcome must be based on reference tables and charts for birthweight by gestational age and sex according to parity and type of delivery. Results support this consideration, giving important clues to address the causes of the increasing rate of CS deliveries in Spain.
Parity and type of delivery are associated with birthweight and have to be considered when analysing birth outcome. Maternal profile and obstetric practices has undergone a significant change over the past decades in Spain affecting birth outcome, as described in other developed countries.
What does this study add to the literature?Based on population data, new charts of birthweight by gestational age, sex, parity and type of delivery for the Spanish population are proposed. Results support the necessity of establishing parity and type of delivery-specific birthweight references to evaluate birth outcome both at clinical and temporal-population levels.
Glòria Pérez.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsJ.M. Terán and C. Varea designed the study and proposed a first draft. J.M. Terán managed and analysed data. C. Bernis, B. Bogin and A. González-González contributed reviewing the literature, editing all versions of the paper and providing relevant contributions. All authors approved the final version.
FundingThe authors acknowledge financial financial support from the School of Sport, Exercise & Health Sciences, Loughborough University (UK), to help defray the publication charges for this article.
Conflicts of interestsNone.
Authors are very grateful to Dr. Tanis R. Fenton (Department of Community Health Sciences, Faculty of Medicine, University of Calgary, Canada) for providing constructive comments on an earlier version of the manuscript.












