



To evaluate the influence of the tenth revision of the International Statistical Classification of Diseases (ICD-10) on tendencies of annual mortality rates, corrected and uncorrected to the ICD-9.
MethodsStarting with the causes with a significant comparability ratio, we calculated the annual ageadjusted rates from 1980 to 2004. The comparability ratio was applied to the rates for 1999–2004, obtaining the corrected series for the whole period. This series was then compared with the uncorrected series using joinpoint regression.
ResultsMortality decreased between 1999 and 2004. Differences were found in blood diseases, hypertensive diseases, cancer of illdefined sites, respiratory insufficiency, and myelodysplastic syndrome.
ConclusionsThe tendency of the main causes of mortality has been largely unaffected by the revisions in the ICD-10, except in infrequent or less specific diseases.
Evaluar la influencia de la décima revisión de la Clasificación Estadística Internacional de Enfermedades (CIE-10) sobre las tendencias de las tasas anuales de mortalidad, con y sin corrección a la CIE-9.
MétodosPartiendo de las causas con razón de comparabilidad significativas, se calcularon las tasas anuales ajustadas por edad de 1980 a 2004. Se aplicaron a las tasas de 1999–2004 su razón de comparabilidad, y se obtuvo la serie corregida en todo el período, que se comparó con la serie sin corrección utilizando una regresión joinpoint.
ResultadosLa mortalidad disminuye en el período 1999–2004. Se encontraron diferencias en el grupo de enfermedades de la sangre, enfermedades hipertensivas, cáncer de sitios mal definidos, insuficiencia respiratoria y síndrome mielodisplásico.
ConclusionesLa tendencia de las principales causas de mortalidad no se afecta por el cambio de revisión, excepto en enfermedades infrecuentes o poco específicas.
In Spain the tenth revision of the International Classification of Diseases (ICD) in mortality was implemented in 1999, introducing the biggest change since the sixth revision in 1948. The modifications in its structure and rules affect the selection and codification of diseases, and it is for this reason that correspondences between ICD must be established, quantified and applied. The impact of the change of revision, has been previously analyzed in other studies1–5 using the international statistical methodology by means of comparability ratios for each group of causes2,4,5. These works suggest that the application of a new revision to the causes of death could generate changes in the tendency of population indicators for causes of death. Here we analyse the impact in the series estimated by joinpoint regression, corrected or uncorrected to the same ICD, of the annual mortality rates in the period 1980–2004.
Material and methodsThe COMPARA-Spain Project1 evaluated the impact of the revision change from ICD-10 to ICD-9. The underlying causes of 88048 deaths doubled coded in ICD-10 and ICD-9, were tabulated by short lists to obtain cause-specific comparability ratios (number of deaths in ICD-10 to deaths in ICD-9 by equivalent codification)2. The Spanish National Statistics Institute (119 items) and the Murcia variants (which adds 7 different items) were the short lists used. The short lists groups of causes with a statistically significant comparability ratio (95%CI did not contain the one) and an absolute differential between ICD greater than 20, were selected. The above criterion maximizes the efficiency of the estimated rates. For the selected causes, we calculated the annual rates for Murcia adjusted for age to the European Standard Population by the direct method. Thus we obtained, for each group of causes, the uncorrected series. As is suggested in others works1–5, each of these series is corrected in the period of ICD-10 (1999-2004) by applying the specific comparability ratio to homogenize the whole period of ICD-9, obtaining the corrected series for each group of causes and the whole period. More concretely, for each group of causes, the uncorrected series consist of the annual rates adjusted for age to the European Standard Population by the direct method, using ICD-9 until 1998 and ICD-10 from 1999 until 2004. The corrected series is obtained, for each group of causes, as follows: until 1998 the corrected series coincides with the uncorrected series, and from 1999 it is obtained multiplying the adjusted rates of the uncorrected series by the specific comparability ratio.
To compare both series, we estimated the annual percentage of change (APC) and the changes in the tendency for the two series, corrected and uncorrected to ICD-9, applying joinpoint log lineal regression. The comparison is based in the behaviour of the two series: the significant changepoints and increases or decreases.
The Joinpoint software version 3.06 was used for the analysis. This technique permitted us to identify the years in which changes in the tendency occurred, as well as to estimate the APC in each of the periods delimited by the points of change. The necessary data for the analysis were the rates and their standard errors. The analysis started with the minimum number of joinpoints and tested if the inclusion of one or more joinpoints were statistically significant7. In the final model, each joinpoint indicated a significant change in the tendency, and the APC was obtained in each of the segments delimited by the joinpoints, by means of the technique of weighted least squares. The significance level to test the number of joinpoints as well as for the APC was 0.05.
ResultsFor the general mortality, the number of total deaths was 56775 in the period 1999-2004 in the Region of Murcia, and the age-adjusted rates decreased (APC=−2.67%; 95%CI: −4.18 to −1.13).
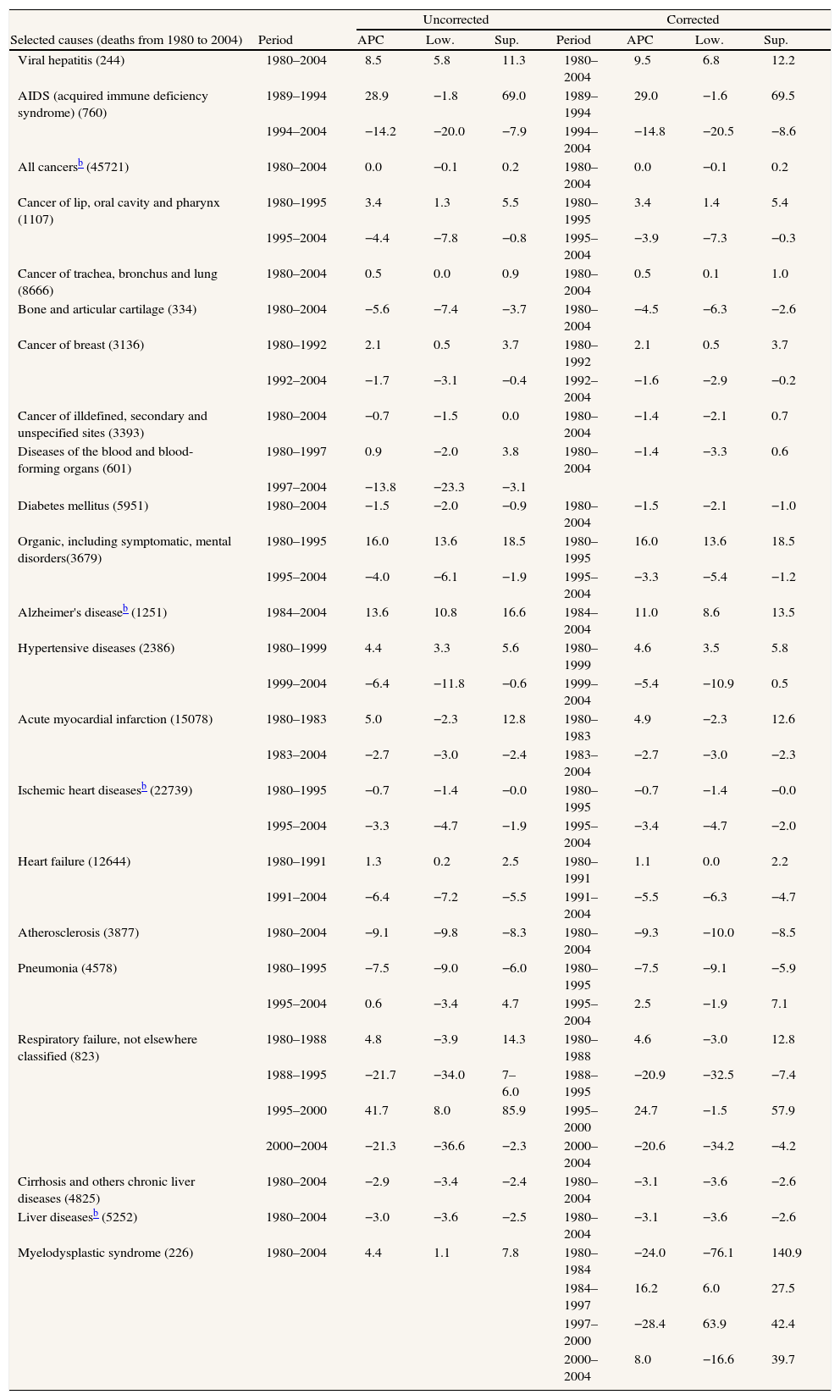
In many causes (Table 1), the change of revision did not influence on the tendency. Both in the corrected series as well as in the uncorrected series, we observed a fall in the period 1980–2004 in bone-cartilage cancer, diabetes mellitus, atherosclerosis and hepatic cirrhosis. Breast cancer showed an increase up to 1992, after which it started to fall, and we can say the same for mental disorders in 1995, cardiac insufficiency in 1991, and lip cancer in 1995. The tendency was ascendant for the whole period for Alzheimer's disease, viral hepatitis and lung cancer, both corrected and uncorrected. The acute myocardial infarction has experienced a fall since 1983. Pneumonia fell until 1995, after which the tendency was ascendant although not significantly and more pronouncedly for the corrected series; and AIDS has fallen since 1994.
Joinpoint estimation of causes of deatha corrected and uncorrected to the ICD-9 (1980–2004)
| Uncorrected | Corrected | |||||||
| Selected causes (deaths from 1980 to 2004) | Period | APC | Low. | Sup. | Period | APC | Low. | Sup. |
| Viral hepatitis (244) | 1980–2004 | 8.5 | 5.8 | 11.3 | 1980–2004 | 9.5 | 6.8 | 12.2 |
| AIDS (acquired immune deficiency syndrome) (760) | 1989–1994 | 28.9 | −1.8 | 69.0 | 1989–1994 | 29.0 | −1.6 | 69.5 |
| 1994–2004 | −14.2 | −20.0 | −7.9 | 1994–2004 | −14.8 | −20.5 | −8.6 | |
| All cancersb (45721) | 1980–2004 | 0.0 | −0.1 | 0.2 | 1980–2004 | 0.0 | −0.1 | 0.2 |
| Cancer of lip, oral cavity and pharynx (1107) | 1980–1995 | 3.4 | 1.3 | 5.5 | 1980–1995 | 3.4 | 1.4 | 5.4 |
| 1995–2004 | −4.4 | −7.8 | −0.8 | 1995–2004 | −3.9 | −7.3 | −0.3 | |
| Cancer of trachea, bronchus and lung (8666) | 1980–2004 | 0.5 | 0.0 | 0.9 | 1980–2004 | 0.5 | 0.1 | 1.0 |
| Bone and articular cartilage (334) | 1980–2004 | −5.6 | −7.4 | −3.7 | 1980–2004 | −4.5 | −6.3 | −2.6 |
| Cancer of breast (3136) | 1980–1992 | 2.1 | 0.5 | 3.7 | 1980–1992 | 2.1 | 0.5 | 3.7 |
| 1992–2004 | −1.7 | −3.1 | −0.4 | 1992–2004 | −1.6 | −2.9 | −0.2 | |
| Cancer of illdefined, secondary and unspecified sites (3393) | 1980–2004 | −0.7 | −1.5 | 0.0 | 1980–2004 | −1.4 | −2.1 | 0.7 |
| Diseases of the blood and blood-forming organs (601) | 1980–1997 | 0.9 | −2.0 | 3.8 | 1980–2004 | −1.4 | −3.3 | 0.6 |
| 1997–2004 | −13.8 | −23.3 | −3.1 | |||||
| Diabetes mellitus (5951) | 1980–2004 | −1.5 | −2.0 | −0.9 | 1980–2004 | −1.5 | −2.1 | −1.0 |
| Organic, including symptomatic, mental disorders(3679) | 1980–1995 | 16.0 | 13.6 | 18.5 | 1980–1995 | 16.0 | 13.6 | 18.5 |
| 1995–2004 | −4.0 | −6.1 | −1.9 | 1995–2004 | −3.3 | −5.4 | −1.2 | |
| Alzheimer's diseaseb (1251) | 1984–2004 | 13.6 | 10.8 | 16.6 | 1984–2004 | 11.0 | 8.6 | 13.5 |
| Hypertensive diseases (2386) | 1980–1999 | 4.4 | 3.3 | 5.6 | 1980–1999 | 4.6 | 3.5 | 5.8 |
| 1999–2004 | −6.4 | −11.8 | −0.6 | 1999–2004 | −5.4 | −10.9 | 0.5 | |
| Acute myocardial infarction (15078) | 1980–1983 | 5.0 | −2.3 | 12.8 | 1980–1983 | 4.9 | −2.3 | 12.6 |
| 1983–2004 | −2.7 | −3.0 | −2.4 | 1983–2004 | −2.7 | −3.0 | −2.3 | |
| Ischemic heart diseasesb (22739) | 1980–1995 | −0.7 | −1.4 | −0.0 | 1980–1995 | −0.7 | −1.4 | −0.0 |
| 1995–2004 | −3.3 | −4.7 | −1.9 | 1995–2004 | −3.4 | −4.7 | −2.0 | |
| Heart failure (12644) | 1980–1991 | 1.3 | 0.2 | 2.5 | 1980–1991 | 1.1 | 0.0 | 2.2 |
| 1991–2004 | −6.4 | −7.2 | −5.5 | 1991–2004 | −5.5 | −6.3 | −4.7 | |
| Atherosclerosis (3877) | 1980–2004 | −9.1 | −9.8 | −8.3 | 1980–2004 | −9.3 | −10.0 | −8.5 |
| Pneumonia (4578) | 1980–1995 | −7.5 | −9.0 | −6.0 | 1980–1995 | −7.5 | −9.1 | −5.9 |
| 1995–2004 | 0.6 | −3.4 | 4.7 | 1995–2004 | 2.5 | −1.9 | 7.1 | |
| Respiratory failure, not elsewhere classified (823) | 1980–1988 | 4.8 | −3.9 | 14.3 | 1980–1988 | 4.6 | −3.0 | 12.8 |
| 1988–1995 | −21.7 | −34.0 | 7–6.0 | 1988–1995 | −20.9 | −32.5 | −7.4 | |
| 1995–2000 | 41.7 | 8.0 | 85.9 | 1995–2000 | 24.7 | −1.5 | 57.9 | |
| 2000−2004 | −21.3 | −36.6 | −2.3 | 2000–2004 | −20.6 | −34.2 | −4.2 | |
| Cirrhosis and others chronic liver diseases (4825) | 1980–2004 | −2.9 | −3.4 | −2.4 | 1980–2004 | −3.1 | −3.6 | −2.6 |
| Liver diseasesb (5252) | 1980–2004 | −3.0 | −3.6 | −2.5 | 1980–2004 | −3.1 | −3.6 | −2.6 |
| Myelodysplastic syndrome (226) | 1980–2004 | 4.4 | 1.1 | 7.8 | 1980–1984 | −24.0 | −76.1 | 140.9 |
| 1984–1997 | 16.2 | 6.0 | 27.5 | |||||
| 1997–2000 | −28.4 | 63.9 | 42.4 | |||||
| 2000–2004 | 8.0 | −16.6 | 39.7 | |||||
APC: annual percentage of change; Low./Sup.: limits of the 95% confidence interval.
The differences with relation to the evolution of both series appear in the diseases of the blood, hypertensive diseases, cancer in ill-defined sites, respiratory insufficiency and myelodysplastic syndrome. For diseases of the blood, the corrected series was descendant over the whole period (−1.4%) although not significantly, while if we did not correct for ICD-9, we found a point of change in 1997, after which the tendency was descendent (−13.8%). In hypertensive diseases there was an inflexion in 1999 according to both series; however the descent after said year was significant only for the uncorrected series. For cancer of ill-defined sites, the tendency was descendent although only significantly if corrected to ICD-9. The tendency for respiratory insufficiency showed three points of change, and the difference appeared in the period 1995–2000. In said period there was a significant increase in the uncorrected series. Finally, myelodysplastic syndrome presented several points of inflexion if we applied the correction, whilst the tendency was ascendant in the whole period 1980–2004 if we did not apply the correction.
DiscussionThe evolution of the tendencies for the majority groups of causes of mortality lists were not affected by the correction upon applying the specific comparability ratio. The change of revision of the ICD had an influence on the diseases of the blood, hypertensive diseases, cancer of ill-defined-secondary and unspecified sites, respiratory insufficiency and the myelodysplastic syndrome.
In our work the analysis has been restricted to the groups of causes with statistically significant comparability ratios, since should differences appear in the tendency after correcting to ICD-9, it was in these groups that they would occur. Both sexes have been considered together8, although the same methodology is applicable to a stratified analysis.
We did not set out to analyse tendencies, but more to answer the question: what happens if we analyse the tendency of mortality correcting the series by the specific comparability ratio of each group of causes? If we compare the corrected series with the uncorrected series only in the period of ICD-10, the estimated APC for said period does not vary, whatever the comparability ratio may be, as can be checked mathematically. If, on the other hand, we restrict the analysis of both series to an arbitrary period between 1980 and 2004, we can find different estimations of the total APC, depending on the said period. Thus, to objectively compare both series, we have followed a procedure in which the periods in which the tendency to be analysed were not preset, and, therefore, the number of points of change and their position were not imposed but unknown parameters that have to be estimated from the data. The models of joinpoint permit one to infer the most plausible moments in which the tendency changed significantly and estimate the APC in each segment delimited by said points. For each cause, both series have been analysed choosing the same options that the Joinpoint program permits, such as for example the significance level (0.05) for the permutations test, and the maximum number of points of change (3).
The joinpoint regression models are widely used nowadays to analyse changes in the tendency, both for series of mortality as well as for series of cancer incidence. Their application is supported by the publication of the reports on tendencies of the National Cancer Institute of the USA. Finally, as we can find in the literature9, incidental country changes in coding rules could be more important than ICD coding changes.
The studies of comparability carried out for the Office for National Statistics to England and Wales10, that implemented for the National Vital Statistics System-Centers for Disease Control and Prevention of the USA11, the Health Statistics Division of Statistics of Canada5, or that developed in the COMPARA project in Spain, were important since they allow the identification of changes between revisions and to evaluate their impact by means of obtaining comparability ratios between ICD for pathological entities. One of the outstanding contributions of the COMPARASpain project was to have valued the influence of the comparability ratios in the time series of mortality by causes.
To Emilia Madrigal, Consuelo Martínez, Miguel Ruiz, Fran Viciana, and the COMPARA research group, for their comments, suggestions and collaboration.











