



In the working population, poor mental health is a significant problem whose prevalence rates and associated factors could differ by gender, especially in a period of socioeconomic changes. The aims of this study were: a) to determine the prevalence of poor mental health in the working population of Spain in 2011; b) to identify the association of this prevalence with socioeconomic and work-related variables for men and women separately; c) to determine if the patterns differ by gender.
MethodsA cross-sectional study was conducted with data from the National Health Survey of Spain (2011). Of the 21,007 participants in the survey, we selected 7396 whose employment status was described as “working” The General Health Questionnaire (GHQ-12) was used as a screening tool to detect poor mental health. Prevalences were calculated and bivariate and multivariate logistic regression models were fitted to verify the association between variables.
ResultsThe prevalence of poor mental health was higher among women (19.9%) than men (13.9%), the overall prevalence being 16.8%. The variables associated with a higher prevalence were type of contract and work-related variables in men, and age and socioeconomic variables in women.
ConclusionsThis study shows that, in the working population of Spain, the prevalence of poor mental health and its related factors differ by gender. Poor mental health is mainly related to socioeconomic variables in women but is mostly associated with work-related variables in men.
En población trabajadora, los problemas de salud mental son un problema significativo cuya prevalencia y factores asociados pueden diferir según el sexo, en especial durante un periodo de cambios socioeconómicos. Los objetivos de este estudio son: a) conocer la prevalencia de problemas de salud mental en población trabajadora de España en 2011; b) evaluar la asociación de esta prevalencia con variables socioeconómicas y laborales para hombres y mujeres por separado; c) determinar si los patrones difieren por sexos.
MétodosEstudio transversal con datos de la Encuesta Nacional de Salud de España (2011). De los 21.007 participantes en la encuesta, se seleccionaron 7396 cuya situación laboral era «trabajando». Se utilizó el General Health Questionnaire (GHQ-12) como herramienta de cribado para detectar problemas de salud mental. Se calcularon las prevalencias y se realizaron modelos bivariados y multivariados de regresión logística para comprobar la asociación entre variables.
ResultadosLa prevalencia de problemas de salud mental fue mayor entre las mujeres (19,9%) que entre los hombres (13,9%), con una prevalencia global del 16,8%. Las variables asociadas a una mayor prevalencia fueron el tipo de contrato y las relacionadas con el empleo remunerado entre hombres, y la edad y las variables socioeconómicas en las mujeres.
ConclusionesEn población trabajadora de España, la prevalencia de problemas de salud mental y sus factores relacionados difieren en función del sexo. Mientras en las mujeres la prevalencia podría estar más relacionada con factores socioeconómicos, en los hombres podría estarlo más con variables relacionadas con el empleo remunerado.
Mental health problems are currently considered a major public health issue worldwide, constituting an important source of disability, dependency and decreased quality of life, as well as high economic costs for health systems.1–3
Several studies have been previously conducted to estimate the prevalence of mental health problems and the related factors in the European and Spanish general population,4–10 finding in them differences over time and depending on the country under study. These facts show the need of both a specific assessment for each country or geographic area, and periodic assessment of it. Regarding the temporal evolution of this prevalence in Spain, is important consider the economic crisis that began in 2009, especially the first years of this period, due to the socioeconomic and labor changes that occurred. As proposed by Barbaglia et al.11 negative socioeconomic changes, especially those that happen in a short time lapse such as the beginning of this period, could significantly increase the incidence of mental health problems.
Besides, it has been observed in general population, a lower prevalence of mental health problems among men than among women regardless of their employment status. The same results have been found among people that are working, so gender and employment status could be considered as key factors when determining the prevalence of mental health problems in a population,12–14 in line with the intersectionality concept15,16 which considers these factors as axes of social inequalities that in addition to interact between them, could influence mental health inequalities.
Regarding the prevalence of mental health problems among working population, there have been several studies to try to determine it both in Europe and in Spain,17–20 being some of them focused on a specific pathology and not in mental health problems in general, and finding among those focused in general mental health, differences in the results obtained possibly due, among other factors, to population differences and the instruments used to determine the prevalence.
Moreover, some studies about the relationship between work and mental health have focused on examining the effect that variables such as the working day length, type of contract or job stress among others. Relative to this,19,21–23 different results have been shown for men and women, highlighting the significant effect that these factors have on the workers mental health, omitting some of these studies variables that might be relevant to explain these differences. Also, there has been carried out several studies that show the relationship between factors such as job insecurity and unemployment and possible mental health problems.18,19 These factors, were increased abruptly during the beginning of the current period of economic recession and could have increased the inequalities between men and women in mental health, being convenient the assessment during these years of the mental health status in order to determine if these inequalities are higher than the previous period.
In addition to this, there have been studies focused on explaining gender differences in health across different variables such as social class and family roles,13,20,24–26 its results point to a possible sexual division of work, showing that socioeconomic and related to domestic and family environment variables might have more weight on women's mental health, and those variables related to paid work of men's mental health. Therefore, taking into account the diversity of these factors from an integrative perspective would provide a wider vision of gender differences in mental health among the working population.
In the described framework, the objectives of this study are: a) determining the prevalence of poor mental health in the working population of Spain in 2011, both total as for men and women separately, and b) determining the relationship between mental health problems and job and socioeconomic variables, c) in order to examine if the patterns differ depending on gender.
MethodsStudy population and designA cross-sectional design based on data from the 2011 Spanish National Health Survey (ENSE-2011) has been used.27 The participants in the ENSE-2011 were 21,007 people representative of the non-institutionalized Spanish population, from which has been selected the 7396 aged between 16 and 65, and whose employment status was working. The sample of the ENSE-2011 was selected using a stratified multi-stage sampling being representative at national level.28 The effective total sample represents the 89% of the theoretical sample, of which 61% are headline households and the remaining 28% reserve households to replace incidents in the headlines. Afterwards, from the total effective sample the people who were working have been selected, constituting the final sample to make the analyses, excluding those individuals under 16 and over 65 years.
Data from the Adults and Home questionnaires of the ENSE-2011 has been used because its content incorporate different socioeconomic and occupational variables, including mental health, that has been assessed using the General Health Questionnaire (GHQ-12), included for the first time in the 2006 edition of the Spanish National Health Survey (ENSE-2006). Data was collected by trained interviewers in the participant households between July 2011 and June 2012.
Variables- 1)
Main outcome
- •
Mental health: it has been measured with the General Health Questionnaire (GHQ-12), a screening instrument for mental health, used to identify possible cases of mental disorder in non-psychiatric patients and in general population, adapted and validated for the Spanish population.29 It is formed by 12 Likert-type items with a score scale of 4 points, and a 2-point scoring method has been used, assigning 0 points to answers 0 and 1, and 1 point to answers 2 and 3, and then adding the points of the 12 items obtaining a total score between 0 and 12. It has been considered poor mental health or positive in the screening, a score 3 or greater.
- •
- 2)
Socioeconomic variables
- •
Marital status: single, married, widowed, divorced or legally separated.
- •
Education and training: no education, primary school, secondary school or high school; university studies.
- •
Occupational social class: obtained from the current or past occupation of the reference person, and based on the nine categories proposed by the Determinants Working Group of Spanish Society of Epidemiology (SEE). These categories have been classified into six groups for the ENSE-2011: Class I (Directors and managers of establishments with 10 or more employees and university degrees), Class II (Directors and managers of establishments with fewer than 10 employees and university diplomas), Class III (Intermediate occupations and self-employed people), Class IV (Supervisors and workers in skilled technical occupations), Class V (Skilled workers in the primary sector and other semi-skilled workers) and Class VI (Unskilled workers).30
- •
Age: in years, taken as a quantitative variable.
These variables have been used as explanatory variables, and also as adjustment variables.
- •
- 3)
Work related variables
- •
Type of contract: civil servant or permanent, self-employment, temporary or without contract.
- •
Job stress: assessed by a Likert-type item, from 1 (anything stressful) to 7 (very stressful), considering: low job stress (1 and 2), medium job stress (3, 4 and 5) and high job stress (6 and 7).
- •
Job satisfaction: evaluated by a Likert scale from 1 (not satisfactory) to 7 (very satisfying) and categorized as: high job satisfaction (6 and 7), medium job satisfaction (3, 4 and 5) and low job satisfaction (1 and 2).
- •
It was carried out a descriptive analysis of the prevalence of mental health problems both overall as according to different variables that have been selected. Bivariate and multivariate logistic regression models were fitted to analyze the relationship between the dependent variable and each of the independent variables selected. The multivariate models were adjusted for age and all socioeconomic variables. Odds ratio (OR), adjusted odds ratio (aOR) and their 95% confidence intervals (95%CI) were obtained. All analyses have been stratified by sex.
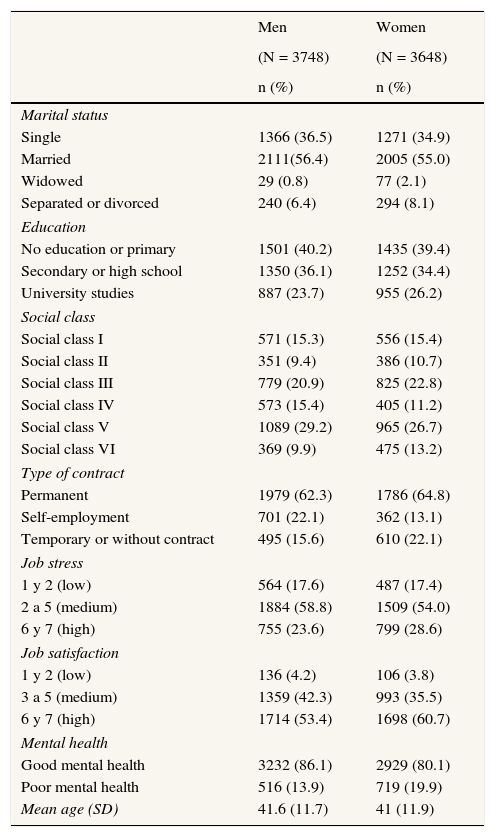
ResultsTable 1 shows the characteristics of the studied sample, showing the distribution of the study participants along the categories of the selected variables. Of the total sample of 7396 participants, 3748 (50.7%) were men with a mean age (SD) of 41.6 (11.7) years; and 3648 (49.3%) were women with a mean age (SD) of 41 (11.9) years. A higher prevalence of poor mental health among women (19.9%) than men (13.9%) was observed.
General description of the sample by sex. Spanish National Health Survey 2011-2012.
| Men | Women | |
|---|---|---|
| (N = 3748) | (N = 3648) | |
| n (%) | n (%) | |
| Marital status | ||
| Single | 1366 (36.5) | 1271 (34.9) |
| Married | 2111(56.4) | 2005 (55.0) |
| Widowed | 29 (0.8) | 77 (2.1) |
| Separated or divorced | 240 (6.4) | 294 (8.1) |
| Education | ||
| No education or primary | 1501 (40.2) | 1435 (39.4) |
| Secondary or high school | 1350 (36.1) | 1252 (34.4) |
| University studies | 887 (23.7) | 955 (26.2) |
| Social class | ||
| Social class I | 571 (15.3) | 556 (15.4) |
| Social class II | 351 (9.4) | 386 (10.7) |
| Social class III | 779 (20.9) | 825 (22.8) |
| Social class IV | 573 (15.4) | 405 (11.2) |
| Social class V | 1089 (29.2) | 965 (26.7) |
| Social class VI | 369 (9.9) | 475 (13.2) |
| Type of contract | ||
| Permanent | 1979 (62.3) | 1786 (64.8) |
| Self-employment | 701 (22.1) | 362 (13.1) |
| Temporary or without contract | 495 (15.6) | 610 (22.1) |
| Job stress | ||
| 1 y 2 (low) | 564 (17.6) | 487 (17.4) |
| 2 a 5 (medium) | 1884 (58.8) | 1509 (54.0) |
| 6 y 7 (high) | 755 (23.6) | 799 (28.6) |
| Job satisfaction | ||
| 1 y 2 (low) | 136 (4.2) | 106 (3.8) |
| 3 a 5 (medium) | 1359 (42.3) | 993 (35.5) |
| 6 y 7 (high) | 1714 (53.4) | 1698 (60.7) |
| Mental health | ||
| Good mental health | 3232 (86.1) | 2929 (80.1) |
| Poor mental health | 516 (13.9) | 719 (19.9) |
| Mean age (SD) | 41.6 (11.7) | 41 (11.9) |
SD: standard deviation.
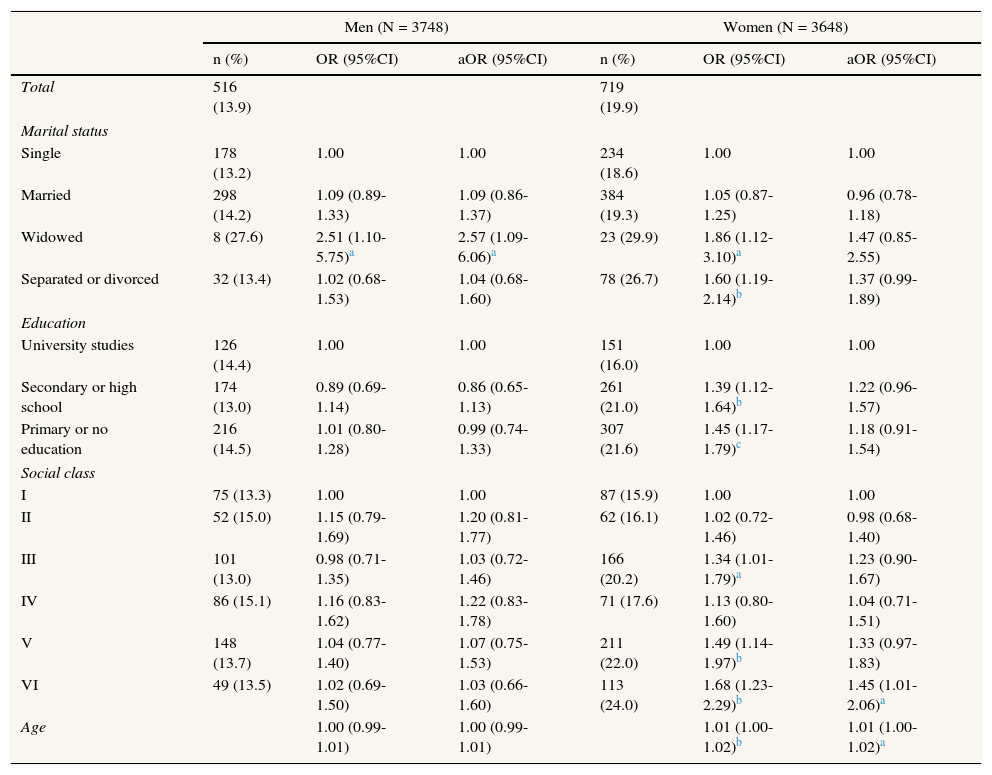
Regarding the poor mental health in working population of Spain, the overall prevalence is 16.8% and it is distributed differently according to gender and socioeconomic variables as shown in Table 2. In relation to age and socioeconomic variables, it has been found from the bivariate analysis among women, a higher prevalence as age increases, among widowed, separated or divorced individuals (26.7%), among those with secondary education and those who have primary education or who do not have any studies, as well as among those self-employed women or others with intermediate occupations; even those that belong to disadvantaged social classes (Social class V: 22% and Social class VI: 24%%). Furthermore, it has been found out that once the models were adjusted, the differences in relation to the reference categories do not remain statistically significant in all cases except among the women that belong to the most disadvantaged social class, or social class VI (aOR = 1.45), and age-related differences.
Association between poor mental health prevalence (%), socioeconomic variables and age stratified by sex. Spanish National Health Survey 2011/2012.
| Men (N = 3748) | Women (N = 3648) | |||||
|---|---|---|---|---|---|---|
| n (%) | OR (95%CI) | aOR (95%CI) | n (%) | OR (95%CI) | aOR (95%CI) | |
| Total | 516 (13.9) | 719 (19.9) | ||||
| Marital status | ||||||
| Single | 178 (13.2) | 1.00 | 1.00 | 234 (18.6) | 1.00 | 1.00 |
| Married | 298 (14.2) | 1.09 (0.89-1.33) | 1.09 (0.86-1.37) | 384 (19.3) | 1.05 (0.87-1.25) | 0.96 (0.78-1.18) |
| Widowed | 8 (27.6) | 2.51 (1.10-5.75)a | 2.57 (1.09-6.06)a | 23 (29.9) | 1.86 (1.12-3.10)a | 1.47 (0.85-2.55) |
| Separated or divorced | 32 (13.4) | 1.02 (0.68-1.53) | 1.04 (0.68-1.60) | 78 (26.7) | 1.60 (1.19-2.14)b | 1.37 (0.99-1.89) |
| Education | ||||||
| University studies | 126 (14.4) | 1.00 | 1.00 | 151 (16.0) | 1.00 | 1.00 |
| Secondary or high school | 174 (13.0) | 0.89 (0.69-1.14) | 0.86 (0.65-1.13) | 261 (21.0) | 1.39 (1.12-1.64)b | 1.22 (0.96-1.57) |
| Primary or no education | 216 (14.5) | 1.01 (0.80-1.28) | 0.99 (0.74-1.33) | 307 (21.6) | 1.45 (1.17-1.79)c | 1.18 (0.91-1.54) |
| Social class | ||||||
| I | 75 (13.3) | 1.00 | 1.00 | 87 (15.9) | 1.00 | 1.00 |
| II | 52 (15.0) | 1.15 (0.79-1.69) | 1.20 (0.81-1.77) | 62 (16.1) | 1.02 (0.72-1.46) | 0.98 (0.68-1.40) |
| III | 101 (13.0) | 0.98 (0.71-1.35) | 1.03 (0.72-1.46) | 166 (20.2) | 1.34 (1.01-1.79)a | 1.23 (0.90-1.67) |
| IV | 86 (15.1) | 1.16 (0.83-1.62) | 1.22 (0.83-1.78) | 71 (17.6) | 1.13 (0.80-1.60) | 1.04 (0.71-1.51) |
| V | 148 (13.7) | 1.04 (0.77-1.40) | 1.07 (0.75-1.53) | 211 (22.0) | 1.49 (1.14-1.97)b | 1.33 (0.97-1.83) |
| VI | 49 (13.5) | 1.02 (0.69-1.50) | 1.03 (0.66-1.60) | 113 (24.0) | 1.68 (1.23-2.29)b | 1.45 (1.01-2.06)a |
| Age | 1.00 (0.99-1.01) | 1.00 (0.99-1.01) | 1.01 (1.00-1.02)b | 1.01 (1.00-1.02)a | ||
OR: odds ratio; aOR: odds ratio adjusted by all socioeconomic variables and age; 95%CI: 95% confidence intervals.
n: number of persons with a score in GHQ-12 ≥ 3.
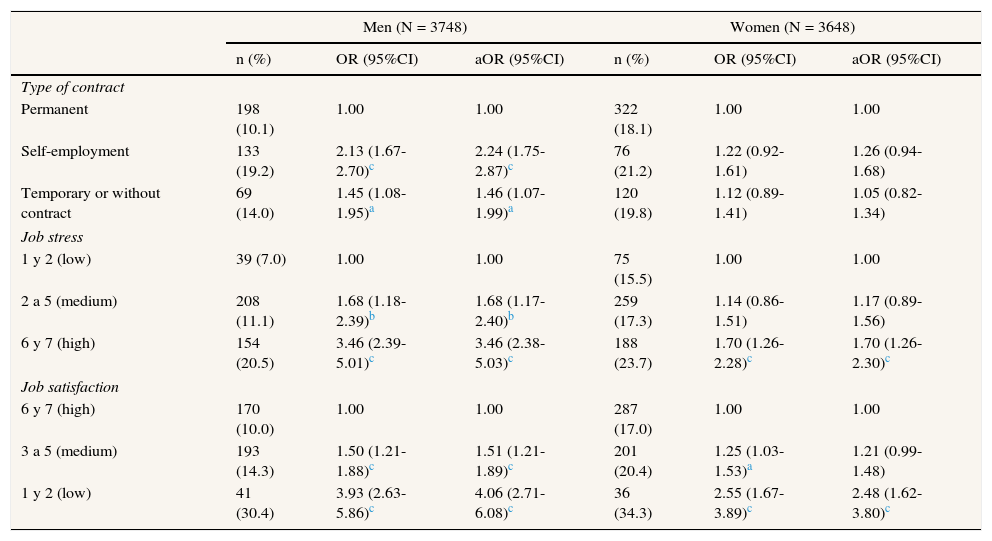
Taking into account work related variables (Table 3), it has been observed a higher prevalence of poor mental health among self-employed men (19.2%), those that have a temporary job or those without contract (14%) and among those with medium stress levels and job satisfaction, being higher the prevalence in both sexes in those with high job stress levels (men: 20.5%; women: 23.7%) and low job satisfaction (men: 30.4%; women: 34.3%). Moreover, from the results of the multivariate analysis, it was observed among men association between self-employment (aOR = 2.24), temporary work or without contract and poor mental health, being also observed among them a gradient of increasing poor mental health when the job stress is higher or job satisfaction is lower, being found among women higher prevalence associated with high job stress levels (aOR = 1.70) but not with middle levels, and with low job satisfaction but not middle.
Association between poor mental health prevalence (%) and work related variables stratified by gender. Spanish National Health Survey 2011/2012.
| Men (N = 3748) | Women (N = 3648) | |||||
|---|---|---|---|---|---|---|
| n (%) | OR (95%CI) | aOR (95%CI) | n (%) | OR (95%CI) | aOR (95%CI) | |
| Type of contract | ||||||
| Permanent | 198 (10.1) | 1.00 | 1.00 | 322 (18.1) | 1.00 | 1.00 |
| Self-employment | 133 (19.2) | 2.13 (1.67-2.70)c | 2.24 (1.75-2.87)c | 76 (21.2) | 1.22 (0.92-1.61) | 1.26 (0.94-1.68) |
| Temporary or without contract | 69 (14.0) | 1.45 (1.08-1.95)a | 1.46 (1.07-1.99)a | 120 (19.8) | 1.12 (0.89-1.41) | 1.05 (0.82-1.34) |
| Job stress | ||||||
| 1 y 2 (low) | 39 (7.0) | 1.00 | 1.00 | 75 (15.5) | 1.00 | 1.00 |
| 2 a 5 (medium) | 208 (11.1) | 1.68 (1.18-2.39)b | 1.68 (1.17-2.40)b | 259 (17.3) | 1.14 (0.86-1.51) | 1.17 (0.89-1.56) |
| 6 y 7 (high) | 154 (20.5) | 3.46 (2.39-5.01)c | 3.46 (2.38-5.03)c | 188 (23.7) | 1.70 (1.26-2.28)c | 1.70 (1.26-2.30)c |
| Job satisfaction | ||||||
| 6 y 7 (high) | 170 (10.0) | 1.00 | 1.00 | 287 (17.0) | 1.00 | 1.00 |
| 3 a 5 (medium) | 193 (14.3) | 1.50 (1.21-1.88)c | 1.51 (1.21-1.89)c | 201 (20.4) | 1.25 (1.03-1.53)a | 1.21 (0.99-1.48) |
| 1 y 2 (low) | 41 (30.4) | 3.93 (2.63-5.86)c | 4.06 (2.71-6.08)c | 36 (34.3) | 2.55 (1.67-3.89)c | 2.48 (1.62-3.80)c |
OR: odds ratio; aOR: odds ratio adjusted by all socioeconomic variables and age; 95%CI: 95% confidence intervals.
n: number of persons with a score in GHQ-12 ≥ 3.
This study shows that the prevalence of poor mental health among working population of Spain in 2011 was 16.8%, being slightly lower than the one observed in previous studies based on general population.8,9 It also shows that this prevalence is not distributed evenly, being higher in women than in men, and being related to different variables according to gender being, with some exceptions, mental health more related to socioeconomic variables among women, and with work related variables among men.
The prevalence of poor mental health found in this study for men (13.9%) and women (19.9%) is slightly higher than that one observed in previous studies with working population,17,23 and it is different from that one seen in another study,14 in which instead of using the data of the edition of 2011, the data from the ENSE-2006 were used, being observed in this study a lower prevalence of poor mental health in men that were working (11.5%) and a higher prevalence in women in the same situation (21.4%). This difference of the results among studies confirms the findings by Bartoll et al.10 in a trends study based on data from the ENSE-2006 and the ENSE-2011, in which the same pattern was found for the general population, suggesting that the pattern of increase of mental health problems in men and slight decrease in women could also be fulfilled for the working population besides for the general population. Further, the difference of results with regard to those obtained with ENSE-2006 data, could be related to the year in which the survey was made. The previous edition of the ENSE was carried out earlier on the current economic recession. Additionally, these results suggest the possible existence of gender differences in the impact that socioeconomic changes can have over the mental health in counties with a traditional familiar policies like Spain.24 Those changes could affect a greater extent to men than women, and could be related to the role of family breadwinner attributed to men in countries with these familiar policies types.
Besides, and also related to the different temporal moment between the last two editions of the survey, the differences found in poor mental health related factors with those obtained with ENSE-2006 data, could be also due to the socioeconomic differences between 2006 and 2011. In the present study a strong relationship between self-employment and poor mental health has been found. In the Bones-Rocha et al.14 study, despite differences in population, this association was not found. This fact, could be related both to the higher job insecurity in 2011 than 2006, as well as to the higher instability and low social protection by the state to the workers in this situation and the impact that this could have, being convenient in subsequent studies take into account these factors when making comparisons on mental health in working population over time.
Regarding the working population mental health, the obtained results reveal gender differences, and confirm the results found in previous studies relative to a higher prevalence of poor mental health among women both in working population,13 and in general population,7,9 being also consistent with the results published in other study,26 in which it was showed that among women, it predicts in a better way the health status the domestic and home sphere, whereas among men it predicts better the paid work. These gender differences, according to the findings of previous studies, could be related to different factors of which Arcas et al.13 highlights the exigencies related with the family roles, and Cortès et al.17 the influence of social class, also proposing that has relevance as associated factor to poor mental health especially among women belonging to the most disadvantaged social classes, finding in the present study results that support the proposals of these authors.
Moreover, it has been found in both sexes a higher prevalence of poor mental health related to high levels of job stress and low levels of job satisfaction. These results are in line with the results of a previous study that shows the relationship between job stress and depression,31 and confirming the results of another study,22 in which it was shown that among the different work related variables that were taken into account, those that could have a higher impact on the mental health in both sexes were the job stress and the imbalance between effort and obtained reward. This imbalance could be related both to job satisfaction, and to domestic work, which is usually made without earning a salary or another reward except for those derived directly of the work.
About the poor mental health related variables among men, the results show the importance of the paid employment related variables, showing only among them a gradient of increasing of the poor mental health prevalence when the job stress is higher or the job satisfaction is lower. Also, and only among men, relationship between poor mental health and self-employment, temporary work or work without contract was found. These results could be explained according to the proposal of Arcas et al.13 regard to the possible association among men between the poor mental health with the family role of main breadwinner and the stress associated to this role, insomuch that self-employment and the work without contract and temporary are the types of contract that could have a higher instability, previously associated to poor mental health,32,33 as well as to a higher economic vulnerability. Given the beginning moment of the current financial crisis in which were collected the data used for the present study, this instability and vulnerability could have a especial relevance, so among the people with these contract types, the paper of family breadwinner could be menaced with the consequent increase of stress related with this role, as well as of the job stress to maintain the job, and the consequences that this increase has over the mental health such as it has been Indicated in previous studies.11,34
Regarding to the factors associated with poor mental health among women, it has been observed from the bivariate analysis that the studied socioeconomic variables are associated with the prevalence of poor mental health in line with what was found in previous studies,14,15 being these results consistent in the hypothesis that among the working women the socioeconomic variables and the family related variables could have a higher relation with the health than among men. These results, also could be related to that pointed by a previous study relative to the traditional model of family policy,24 which is still maintained in Spain and that attributes the responsibility of the domestic work and the role of family carer to women, and that could suppose a work overload when it is added to the paid employment with important consequences for health, as shown in previous studies.25,35,36 Furthermore, it has been observed that after having adjusted the analysis by the other socioeconomic variables and age, the relationship between these variables and the mental health lose his statistical relevance, excepting the age related differences and the differences found among women that work in unskilled jobs. This fact confirms the proposal of Cortès et al.17 about that the social class could be a factor specially related to mental health among women of the disadvantaged social classes, and it also shows the importance of making an adjustment of the analysis by these variables in order to obtain an adequate representation of the factors which could influence the mental health of the working population, especially for women.
Regarding the limitations of the present study, one of them is the type of design used in it. It is a cross-sectional design that does not allow for establishing causal relationships between the studied variables. Moreover, in relation to the assessment of the poor mental health, it has been used a screening instrument, the GHQ-12, whose sensitivity is higher than its specificity, being more sensitive to anxiety and depression than to the rest of the mental disorders. This could lead to an overestimation of the poor mental health prevalence, and an underestimation of the mental disorders that differ from anxiety or depression. Another possible limitation is the one related to the design of the questionnaires of the ENSE-2011, which are designed for the general population and not entirely for the working population, reason why some work related variables have been omitted. Analysing this variables, could be interesting in order to obtain a more adjusted description of the related factors to poor mental health in the working population of Spain as it has been proved in previous studies.23,37
In addition, the survey data belong to 2011, year in which the employment situation in the country was very different than the current. However, worth noting that the results of this study could serve as a reference point, once the new edition of the ENSE be available, to assess how it has evolved the mental health of the working population during the economic recession, and check whether gender differences in this area have increased, decreased or have been changes in the patterns of evolution or associated factors.
In conclusion, the obtained results show that the prevalence of poor mental health in working population of Spain in 2011 was closely related to gender, being higher among women than among men. They also provide further evidence in favour of the hypothesis that support that the socioeconomic variables could have a higher weight in the mental health of women and those related to the paid work in men, being necessary further studies to try to obtain a better explanation of the specific factors related to this difference, and showing the need to adopt political and social measures to try to promote equality and reduce the gender differences in mental health.
Editor in chargeClara Bermúdez-Tamayo.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Several studies has been made to try to determine the poor mental health prevalence, showing gender differences and the possibility that the socioeconomic and family related variables could have a higher impact on mental health among women, and the paid work related variables among men.
What does this study add to the literature?In the working population of Spain in 2011, we found gender differences in poor mental health prevalence, being higher among women than among men, and being related according to gender with different variables. While among women the poor mental health are more associated with social class and the other socioeconomic variables, among men are more associated with type of contract and the other work related variables.
All authors were involved in the conception and design of the study. V. Martin, L. Artazcoz and A.J. Molina supervised all aspects of job performance. J. Arias-de la Torre carried out the data analysis. T. Fernández-Villa and J. Arias-de la Torre interpreted the data and wrote the manuscript. All authors have critically reviewed and approved the final version of the manuscript.
FundingNone.
Conflicts of interestNone.











