



To determine trends in the incidence of type 1 diabetes in Navarre (Spain) between 1975 and 2012 by age and sex.
Patients and methodsThe study population comprised residents of Navarre under 15 years of age. A Poisson regression model was fitted to analyze changes in the incidence over time, adjusted by year of diagnosis, age group and sex.
ResultsA total of 494 patients were registered, representing an adjusted incidence rate of 13.2/100,000 person-years. The annual relative increase in the incidence rate was 3.7%. The highest incidence was found in the group aged 10–14 years. The incidence among boys aged 10–14 tended to be higher than that in girls of the same age.
ConclusionsSince the year 2000, the incidence of type 1 diabetes among persons younger than 15 years in Navarre has been very high and has quadrupled over the last four decades.
Determinar la tendencia en la incidencia de diabetes tipo 1 en Navarra entre 1975 y 2012 por edad y sexo.
Pacientes y métodosLa población objeto de estudio comprende a los residentes en Navarra menores de 15 años de edad. Para analizar la evolución de la incidencia a lo largo del tiempo, se ha utilizado un modelo de regresión de Poisson ajustado por año de diagnóstico, grupo de edad y sexo.
ResultadosSe han diagnosticado 494 pacientes, lo que supone una incidencia ajustada de 13,2/100.000 personas-año. El incremento relativo anual en la tasa de incidencia ha sido del 3,7%. El grupo de edad con mayor incidencia fue el de 10 a 14 años. En este mismo grupo, la incidencia en niños tiende a ser mayor que en niñas.
ConclusionesDesde el año 2000, la incidencia de diabetes tipo 1 en menores de 15 años, en Navarra, es muy alta y se ha cuadriplicado en las últimas cuatro décadas.
The incidence of type 1 diabetes (T1D) in children under 15 ranges from 0.1/100,000 person-years in Venezuela to 57.6/100,000 in Finland.1 This variation could reflect differences in genetic susceptibility between populations, different exposure to environmental risk factors2 or differences in features and quality registers.3 In Spain, the incidence is very high (20.6)1 and, between Autonomous Communities, the highest incidence rate is twice that of the lowest.3
The highest incidence appears in the 10–14 age group, coinciding with puberty.4 In some populations, however, the 5–9 age group has the highest incidence.5 Furthermore, a shift to younger age of onset has been described6 and, in some countries, such as Sweden,7 Germany8 and Belgium,9 it has been debated whether there has truly been an increase in incidence in recent years, or just an earlier onset of the disease.
Regarding the differences in incidence between the sexes before the age of 15, it appears that in countries with a high overall incidence of T1D, it is more common in boys, whereas in low-incidence countries, it is higher among girls.10 In some registers, no difference is found between the sexes9 or, where these differences appear, they start at the age of ten.11
In order to determine whether there has been an increase in the incidence and/or a change in the age of onset in Navarre, this paper describes the changes over the past four decades in the incidence in children under 15 years, including characteristics in terms of age group and sex.
Subjects and methodsThe study population comprises the residents of Navarre under 15 years of age. Information on patients diagnosed between 01/01/1975 and 31/12/1991 was obtained as described in the first study conducted in Navarra.12 Between 01/01/1992 and 31/12/2008; we used the same methods, using Primary Care computerized information systems as main secondary source since 2001. Information on patients diagnosed from 01/01/2009 to 31/12/2012 was obtained as described in our last publication.13
Statistical analysisIncidence rates expressed per 100,000 person-years at risk during the study period, by age group, sex and time period were calculated using data from censuses and records of Navarre (Source: Spanish National Institute of Statistics). Incidence rates were adjusted to a standard population consisting of equal number of children in each of six subgroups defined by age group (0–4, 5–9 and 10–14 years) and sex. Four-year time periods were considered for calculations, except for the first and the last one, which were of five years. Incidence rates were adjusted to a standard population consisting of equal number of children in each of six subgroups defined by age group (0–4, 5–9 and 10–14 years) and sex.
Confidence intervals were estimated at 95%, assuming an underlying Poisson distribution. A Chi-square test was used to compare incidence between groups (independence test), A Poisson regression model was used to analyze changes in incidence since 1975, adjusted for year of diagnosis, age group and sex, from which rate ratios were obtained, together with their 95% confidence intervals. Interaction terms were also included to assess whether time trend differed among age groups or sex, and removed if not significant. For statistical analysis, IBM SPSS Statistics 20 and R 2.13.1 were used.
This study has been reviewed and approved by the Navarre Research Ethics Committee.
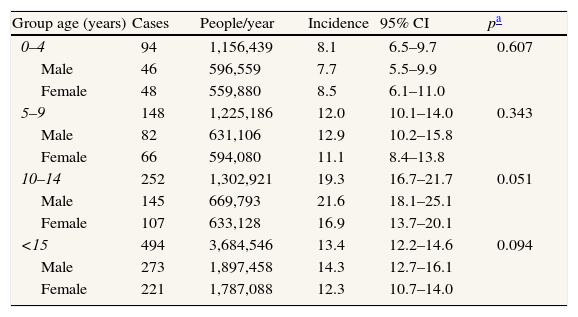
ResultsA total of 494 new cases of T1D aged under 15 (273 boys and 221 girls) were recorded, equivalent to a crude incidence rate of 13.4 per 100,000 inhabitants per year (95% CI: 12.2–14.6) and an adjusted incidence rate of 13.2 (95% CI: 12.0–14.3) (Table 1). The age group with the highest incidence was the 10–14 year-olds (p<0.001). The incidence in boys, 14.3 (95% CI: 12.7–16.1), was higher than in girls, 12.3 (95% CI: 10.7–14.0), but no significant differences (p=0.094) were observed except the trend in the 10–14 age group, for which the statistical significance was marginal (p=0.051) (Table 1).
Incidence of type 1 diabetes (number of cases per 100,000, per year) by age and sex. Navarre 1975–2012.
| Group age (years) | Cases | People/year | Incidence | 95% CI | pa |
| 0–4 | 94 | 1,156,439 | 8.1 | 6.5–9.7 | 0.607 |
| Male | 46 | 596,559 | 7.7 | 5.5–9.9 | |
| Female | 48 | 559,880 | 8.5 | 6.1–11.0 | |
| 5–9 | 148 | 1,225,186 | 12.0 | 10.1–14.0 | 0.343 |
| Male | 82 | 631,106 | 12.9 | 10.2–15.8 | |
| Female | 66 | 594,080 | 11.1 | 8.4–13.8 | |
| 10–14 | 252 | 1,302,921 | 19.3 | 16.7–21.7 | 0.051 |
| Male | 145 | 669,793 | 21.6 | 18.1–25.1 | |
| Female | 107 | 633,128 | 16.9 | 13.7–20.1 | |
| <15 | 494 | 3,684,546 | 13.4 | 12.2–14.6 | 0.094 |
| Male | 273 | 1,897,458 | 14.3 | 12.7–16.1 | |
| Female | 221 | 1,787,088 | 12.3 | 10.7–14.0 |
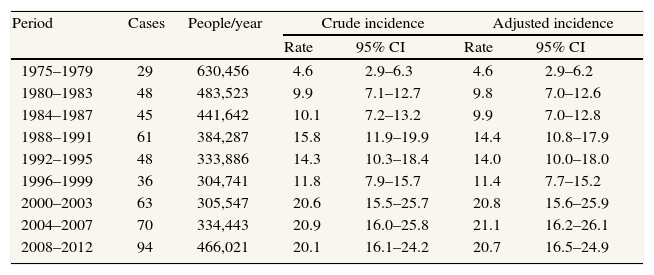
Adjusted incidences for four or five-year periods are shown in Table 2. The highest incidence was recorded in 2004–2007 (21.1; 95% CI: 16.2–26.1) and the lowest, between 1975 and 1979 (4.6; 95% CI: 2.9–6.2) (Table 2). The overall rate of diagnosis increases markedly up to the period 2000–2003, before stabilizing between 20 and 21 cases per 100,000 until the end of the study period.
Crude and adjusted incidence rate of type 1 diabetes (number of cases per 100,000 person-years) by time period. Navarre 1975–2012.
| Period | Cases | People/year | Crude incidence | Adjusted incidence | ||
| Rate | 95% CI | Rate | 95% CI | |||
| 1975–1979 | 29 | 630,456 | 4.6 | 2.9–6.3 | 4.6 | 2.9–6.2 |
| 1980–1983 | 48 | 483,523 | 9.9 | 7.1–12.7 | 9.8 | 7.0–12.6 |
| 1984–1987 | 45 | 441,642 | 10.1 | 7.2–13.2 | 9.9 | 7.0–12.8 |
| 1988–1991 | 61 | 384,287 | 15.8 | 11.9–19.9 | 14.4 | 10.8–17.9 |
| 1992–1995 | 48 | 333,886 | 14.3 | 10.3–18.4 | 14.0 | 10.0–18.0 |
| 1996–1999 | 36 | 304,741 | 11.8 | 7.9–15.7 | 11.4 | 7.7–15.2 |
| 2000–2003 | 63 | 305,547 | 20.6 | 15.5–25.7 | 20.8 | 15.6–25.9 |
| 2004–2007 | 70 | 334,443 | 20.9 | 16.0–25.8 | 21.1 | 16.2–26.1 |
| 2008–2012 | 94 | 466,021 | 20.1 | 16.1–24.2 | 20.7 | 16.5–24.9 |
Note: 1975–1979 and 2008–2012 span five years while the remaining periods span four years.
The results of the Poisson regression model show an annual relative increase of 3.7% (95% CI: 2.9–4.5%) in the incidence rate (p<0.001). Compared to the group under 5 years, the incidence rate in children aged 5–9 is 1.53 (95% CI: 1.18–1.99), and that of children aged 10–14 is 2.50 (95% CI: 1.98–3.18). The rate ratio for boys versus girls is 1.16 (95% CI: 0.97–1.39). We did not find the time trend to be different between age groups (interaction term p-value=0.912) or sex (interaction term p-value=0.745).
DiscussionThe incidence of T1D in children in Navarre increased over time, from 1975 to 2012, in the three age groups studied. The age group with the highest incidence was 10–14 years among all the study period, with an incidence rate over these years of more than twice that of children under five.
The strength of this study lies in its incidence data record of 38 years, a longer period than can be found in most published papers. In addition, the methods for collecting patients have been comprehensive from the start. Limitations include the fact that, for the size of the population of Navarre, the annual rates are not stable, showing large relative changes in magnitude. Moreover, there is always the possibility that the method has not succeeded in recording 100% of patients. Such an underestimation would be more likely in the early years of the study. However, even the data from the initial period, which is less complete (94.6%), is complete enough to be reliable and be included in the incidence study.
The increase is not linear, but does not suggest any cyclical pattern as described by other authors.6 The annual relative mean increase in the incidence rate is 3.7%, which is very close to the average for the EURODIAB data.4 although in our case, rates did not increase in the final decade of the study period, in line with the reported data from Oxford (UK), which are included in the EURODIAB group.
Some authors7–9 have questioned the increased incidence theory, suggesting that the data simply reveal an earlier age of onset. The present study reports increased incidence in all three age groups. Therefore, although it cannot be ruled out that there has been a shift in the age of diagnosis to childhood at the expense of adult patients, the authors are inclined to think that there has in fact been a real increase in the incidence of T1D and not a mere shift. This opinion is in line with Harjutsalo et al. in Finland.11 Moreover, in 2011, the same Swedish group that questioned the increase in incidence,7 published a paper again reporting that, since 2000, the age group with the highest incidence in children is the 10–14 year-olds.14
The incidence among boys tends to be higher than among girls in the 10–14 age group. This trend is consistent with results published from some European countries,11 It has been suggested that physiological changes due to puberty act as triggers for diabetes,13 which could explain the increased incidence in boys aged 10–14, since they reach puberty later than girls. However, in contrast to findings from other groups,15 no peak in incidence was observed in girls in the 5–9 age group. On the contrary, the incidence is still lower than in boys, suggesting that the difference in the timing of the onset of puberty does not explain the higher incidence observed in males aged 10–14.
In conclusion, the incidence of T1D in children under 15 in Navarre has quadrupled in the last four decades, with an annual relative increase in the incidence rate similar to that of neighbouring countries.
Most of National Diabetes Registries agree that the incidence of type 1 diabetes in children is increasing. But, on the other hand, a shift to younger age of onset has been described. So, its being debated whether there is truly an increase in incidence or just an earlier onset of the disease.
What this study adds to the literature?In this study we show that the incidence of type 1 diabetes in children, in Navarre, has quadrupled over the last four decades. The age group with the highest incidence has not changed. So, the public health systems should be aware of this increase in order to prepare the necessary resources to confront this important health problem and prevent its personal and social consequences
Alberto Ruano.
Contribution to authorshipLuis Forga has written the article, especially: Introduction, Discussion and References. He has approved the final version. María José Goñi has thought up this study. She has collaborated redacting the whole text, and she has approved the final version. Koldo Cambra and Berta Ibáñez have designed the study methodology and they have made the statistical analysis of the data. They have also approved the final text. María Chueca and Sara Berrade have been collecting the data. They have also made the tables and they have checked and discussed the article, especially the results in order to approve the final version.
FundingThis study has been supported by a grant from the Carlos III Institute of Health (PI10/02715) and a grant from the Government of Navarre (53/2008).
Conflicts of interestsThe authors declare no conflict of interest.
The authors thank to the other members of “Grupo de Estudio de Diabetes tipo 1 de Navarra”, their collaboration in this study:
- -
Servicio de Endocrinología, Complejo Hospitalario de Navarra. Pamplona: Emma Anda, Marta García-Mouriz, Ana Iriarte, Javier Lafita, Juan Pablo Martínez, María Dolores Ollero, Rosa Rodríguez-Erdozain, Amaya Sainz de los Terreros y David Mozas Ruiz.
- -
Sección de Endocrinología Pediátrica. Complejo Hospitalario de Navarra. Pamplona: Miren Oyarzábal.
- -
Endocrinología. Hospital García Orcoyen. Estella: Javier Pineda, Marta Toni
- -
Endocrinología. Hospital Reina Sofía. Tudela: Francisco Javier Basterra, Patricia Munárriz.
- -
Clínica Universidad de Navarra: Javier Escalada San Martín.











