



This study aimed to analyze the incidence of colorectal cancer in 15 European countries in recent decades and the relationship between the incidence found and changes in dietary habits.
MethodsPearson's or Spearman's correlation coefficients were calculated by comparing incidence rates obtained from the International Agency for Research on Cancer for 1971-2002 with data on per capita consumption obtained from the Food and Agriculture Organization of the United Nations using 10-year delay intervals.
ResultsIncidence rates increased in all countries except France in men and except Austria, Denmark, England and France in women. Of the dietary variables considered, there were marked increasing trends (linear regression coefficient, R ≥0.5) in red meat consumption in Germany (R = 0.9), Austria (R = 0.7), Finland (R = 0.8), Italy (R = 0.9), Poland (R = 0.5), Spain (R = 2.1), Sweden (R = 0.6), and the Netherlands (R = 0.7).
ConclusionsChanges in dietary habits may be consistent with the observed trends in the incidence of colorectal cancer in the distinct European countries.
Este estudio analiza la incidencia de cáncer colorrectal en 15 países europeos en las últimas décadas y su relación con cambios en los hábitos alimenticios.
MétodosCoeficientes de correlación de Pearson/Spearman calculados comparando las tasas de incidencia obtenidas de International Agency for Research on Cancer durante 1971-2002 con los consumos per cápita obtenidos de Food and Agriculture Organization con intervalos de retardo de 10 años.
ResultadosLas tasas de incidencia aumentan en todos los países, excepto en Francia, en los hombres, y en Austria, Dinamarca, Inglaterra y Francia en las mujeres. De las variables de la dieta estudiadas, hay marcadas tendencias crecientes (coeficiente de regresión lineal, R ≥0,5) para carne roja en Alemania (R = 0,9), Austria (R = 0,7), España (R = 2,1), Finlandia (R = 0,8), Italia (R = 0,9), Países Bajos (R = 0,7), Polonia (R = 0,5) y Suecia (R = 0,6).
ConclusionesLos cambios en los hábitos dietéticos pueden ser concordantes con las tendencias de la incidencia de cáncer colorrectal observadas en diferentes países.
The latest available data from the cancer registries supervised by the International Agency for Research on Cancer (IARC) in Europe show that, globally, colorectal cancer is the second most incident tumor in men in Iceland, Norway and Sweden and the third in Austria, Denmark, England, Finland, France, Germany, Italy, Poland, Scotland, Spain, Switzerland and the Netherlands. In women, this tumor has the second highest incidence in Austria, Finland, France, Germany, Italy, Norway, Poland, Spain, Sweden, Switzerland and the Netherlands and the third in Denmark, England, Iceland and Scotland1.
There is still considerable variation among the incidences of colorectal cancer in these 15 European countries. In 2002, the absolute difference in colorectal cancer incidence rates in men adjusted to the worldwide population between Finland (lowest incidence) and Germany (highest incidence) was 27.6 cases per 100,000 inhabitants, representing a relative difference of 107.4%. The same comparison in women showed a difference of 13.5 cases per 100,000 inhabitants between Poland and Germany (lowest and highest incidences, respectively), representing a relative difference of 69.6%.
This major variation in the incidence of colorectal cancer in distinct geographical regions is probably due to distinct levels of exposure to risk and protective factors2.
The aim of this study was to analyze the trends in the incidence of colorectal cancer in 15 European countries in the last few decades and to determine how these trends correlate with changes in the dietary habits of these populations during this period.
MethodsAnnual colorectal cancer incidence rates adjusted to the worldwide population per 100,000 inhabitants (codes C18-C21, 10th revision of the International Classification of Diseases) in men and women were obtained from the International Agency for Research on Cancer for 1971-2002. Rates were gathered by beginning with the first year with accessible data in the cancer registries of each country until 2002 (except Spain, until 2000), which was the last year for which data were available at the time of this study. Annual colorectal cancer incidence rates in both genders were plotted on a linear scale.
Data from the IARC correspond to distinct types of cancer registries. Local cancer registries cover specific areas in each country: Austria, Germany and the Netherlands. Central cancer registries gather and homogenize the information from several local cancer registries: England, France, Italy, Poland, Spain and Switzerland. Finally, national cancer registries cover the whole population of the country: Denmark, Finland, Iceland, Norway, Scotland and Sweden1.
Annual per capita data on alcohol consumption (liters), cereals, fruit, vegetables, legumes, poultry, red meat and fish (kilograms) for 1961-1992 were obtained from the Food and Agriculture Organization of the United Nations (FAO)3.
Pearson's or Spearman's correlation coefficients (depending on the underlying distribution of the variable) were calculated by gender using 10-year delay intervals4,5, i.e. annual colorectal cancer incidence rates adjusted to the worldwide population per 100,000 inhabitants in men and women were correlated with annual per capita consumption data in the previous 10 years, according to the available period in each country studied. The statistical analyses were performed using Stata 10.0 StataCorp LP, Texas, USA.
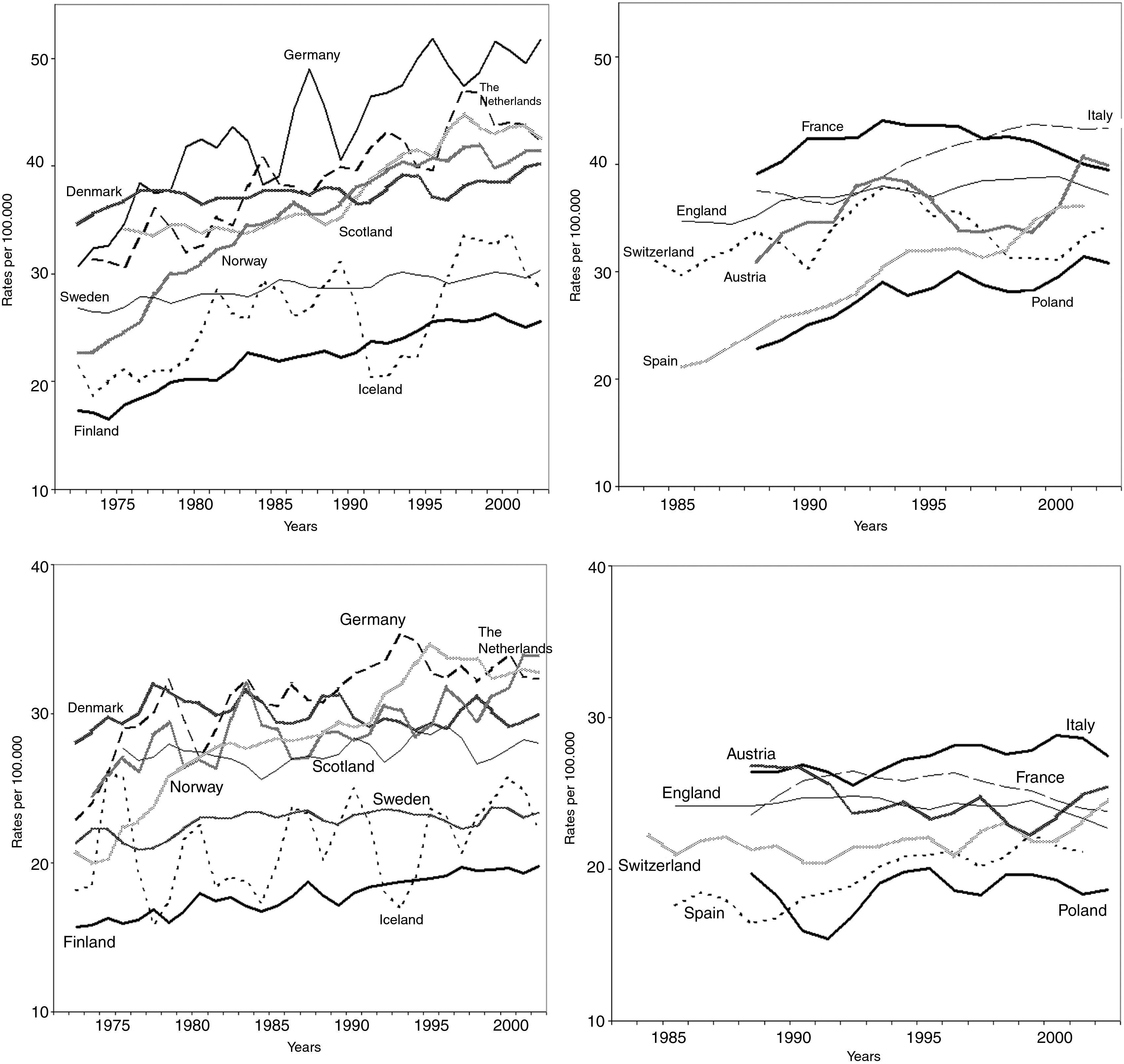
ResultsAnnual colorectal cancer incidence rates were plotted for men and women (fig. 1), according to the available time period in each country studied. The incidence rates were higher in men than in women throughout the period in all countries except the Netherlands (for 1 year) and Iceland (for 8 years).

Annual colorectal cancer incidence rates adjusted to the worldwide population per 100,000 inhabitants, men (above) and women (below). Austria (1988-2002), Denmark (1971-2002), England (1985-2002), Finland (1971-2002), France (1988-2002), Germany (1971-2002), Iceland (1971-2002), Italy (1988-2002), Norway (1971-2002), Poland (1988-2002), Scotland (1975-2002), Spain (1985-2000), Sweden (1971-2002), Switzerland (1983-2002), and the Netherlands (1973-2002).
Throughout the study, incidence rates followed an increasing linear trend in all countries except France in men and except Austria, Denmark, England and France in women.
In Finland, Germany, Iceland, Italy, Norway, Poland, Scotland, Spain, Sweden, Switzerland and the Netherlands, incidence rates in both genders showed an increasing trend with a greater slope in men than in women.
During the study periods for the distinct dietary variables (corresponding to the 10 years prior to the period of the available incidence rates), the prominent dietary trends considered in this study were those that showed a linear regression coefficient (R) ≥|0.5|.
Among food of vegetable origin, fruit consumption increased markedly in all countries except Denmark (R = 0.3). For vegetable consumption, Norway, Switzerland and the Netherlands were the only countries with an R <|0.5|, with R-values of 0.1, 0.4, and -0.2, respectively. Cereal consumption showed considerable variations in Finland (R = -0.8), France (R = 0.7), Italy (R = -1.9), Norway (R = 0.6), Poland (R = -2.2) and the Netherlands (R = -0.5). None of the countries studied showed an R ≥|0.5| in legume consumption.
Among food of animal origin, substantial increasing trends were found in red meat consumption in Austria (R = 0.7), Finland (R = 0.8), Germany (R = 0.9), Italy (R = 0.9), Poland (R = 0.5), Spain (R = 2.1), Sweden (R = 0.6), and the Netherlands (R = 0.7). The countries with the most prominent increases in poultry consumption were England (R = 0.5), France (R = 0.5) and the Netherlands (R = 0.5). There were notable increasing trends in fish consumption in Finland (R = 0.5), France (R = 0.6), Iceland (R = 1.1) and Italy (R = 0.8).
Alcohol consumption showed no marked trends in any of the countries studied.
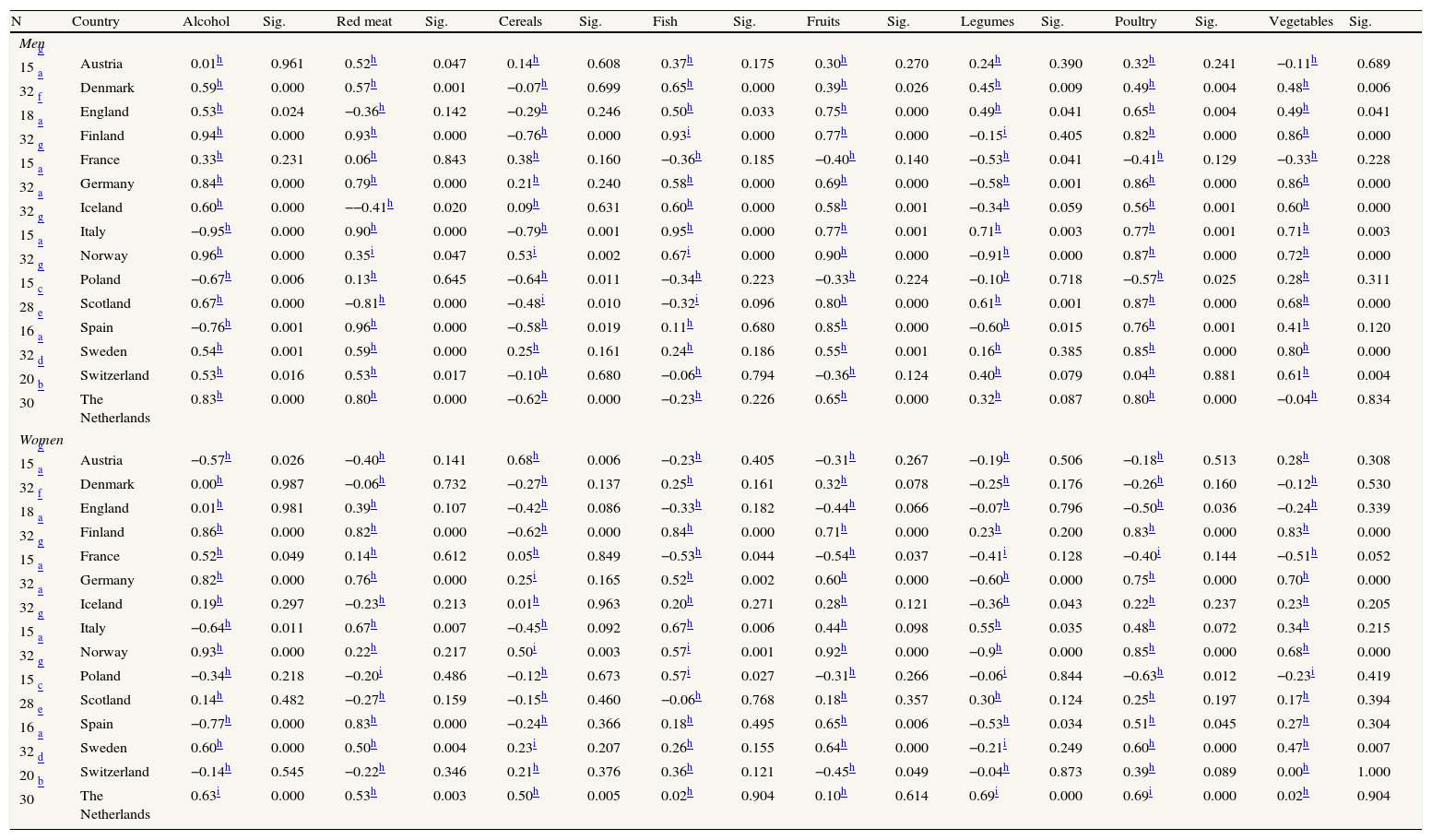
Table 1 shows Pearson's/Spearman's correlation coefficients between trends for the distinct dietary variables and the incidence of colorectal cancer according to gender. In general, the absolute value of the correlation coefficients was greater in men than in women. In men, 34 of the 120 correlations were both strong correlations (correlation coefficient ≥|0.75|) and statistically significant, representing 28.3% of the correlations calculated in men compared with 14 of 120 correlations (11.7%) in women.
Pearson/Spearman's correlation coefficients of dietary variables compared with annual colorectal cancer incidence rates.
| N | Country | Alcohol | Sig. | Red meat | Sig. | Cereals | Sig. | Fish | Sig. | Fruits | Sig. | Legumes | Sig. | Poultry | Sig. | Vegetables | Sig. |
| Men | |||||||||||||||||
| g 15 | Austria | 0.01h | 0.961 | 0.52h | 0.047 | 0.14h | 0.608 | 0.37h | 0.175 | 0.30h | 0.270 | 0.24h | 0.390 | 0.32h | 0.241 | −0.11h | 0.689 |
| a 32 | Denmark | 0.59h | 0.000 | 0.57h | 0.001 | −0.07h | 0.699 | 0.65h | 0.000 | 0.39h | 0.026 | 0.45h | 0.009 | 0.49h | 0.004 | 0.48h | 0.006 |
| f 18 | England | 0.53h | 0.024 | −0.36h | 0.142 | −0.29h | 0.246 | 0.50h | 0.033 | 0.75h | 0.000 | 0.49h | 0.041 | 0.65h | 0.004 | 0.49h | 0.041 |
| a 32 | Finland | 0.94h | 0.000 | 0.93h | 0.000 | −0.76h | 0.000 | 0.93i | 0.000 | 0.77h | 0.000 | −0.15i | 0.405 | 0.82h | 0.000 | 0.86h | 0.000 |
| g 15 | France | 0.33h | 0.231 | 0.06h | 0.843 | 0.38h | 0.160 | −0.36h | 0.185 | −0.40h | 0.140 | −0.53h | 0.041 | −0.41h | 0.129 | −0.33h | 0.228 |
| a 32 | Germany | 0.84h | 0.000 | 0.79h | 0.000 | 0.21h | 0.240 | 0.58h | 0.000 | 0.69h | 0.000 | −0.58h | 0.001 | 0.86h | 0.000 | 0.86h | 0.000 |
| a 32 | Iceland | 0.60h | 0.000 | −−0.41h | 0.020 | 0.09h | 0.631 | 0.60h | 0.000 | 0.58h | 0.001 | −0.34h | 0.059 | 0.56h | 0.001 | 0.60h | 0.000 |
| g 15 | Italy | −0.95h | 0.000 | 0.90h | 0.000 | −0.79h | 0.001 | 0.95h | 0.000 | 0.77h | 0.001 | 0.71h | 0.003 | 0.77h | 0.001 | 0.71h | 0.003 |
| a 32 | Norway | 0.96h | 0.000 | 0.35i | 0.047 | 0.53i | 0.002 | 0.67i | 0.000 | 0.90h | 0.000 | −0.91h | 0.000 | 0.87h | 0.000 | 0.72h | 0.000 |
| g 15 | Poland | −0.67h | 0.006 | 0.13h | 0.645 | −0.64h | 0.011 | −0.34h | 0.223 | −0.33h | 0.224 | −0.10h | 0.718 | −0.57h | 0.025 | 0.28h | 0.311 |
| c 28 | Scotland | 0.67h | 0.000 | −0.81h | 0.000 | −0.48i | 0.010 | −0.32i | 0.096 | 0.80h | 0.000 | 0.61h | 0.001 | 0.87h | 0.000 | 0.68h | 0.000 |
| e 16 | Spain | −0.76h | 0.001 | 0.96h | 0.000 | −0.58h | 0.019 | 0.11h | 0.680 | 0.85h | 0.000 | −0.60h | 0.015 | 0.76h | 0.001 | 0.41h | 0.120 |
| a 32 | Sweden | 0.54h | 0.001 | 0.59h | 0.000 | 0.25h | 0.161 | 0.24h | 0.186 | 0.55h | 0.001 | 0.16h | 0.385 | 0.85h | 0.000 | 0.80h | 0.000 |
| d 20 | Switzerland | 0.53h | 0.016 | 0.53h | 0.017 | −0.10h | 0.680 | −0.06h | 0.794 | −0.36h | 0.124 | 0.40h | 0.079 | 0.04h | 0.881 | 0.61h | 0.004 |
| b 30 | The Netherlands | 0.83h | 0.000 | 0.80h | 0.000 | −0.62h | 0.000 | −0.23h | 0.226 | 0.65h | 0.000 | 0.32h | 0.087 | 0.80h | 0.000 | −0.04h | 0.834 |
| Women | |||||||||||||||||
| g 15 | Austria | −0.57h | 0.026 | −0.40h | 0.141 | 0.68h | 0.006 | −0.23h | 0.405 | −0.31h | 0.267 | −0.19h | 0.506 | −0.18h | 0.513 | 0.28h | 0.308 |
| a 32 | Denmark | 0.00h | 0.987 | −0.06h | 0.732 | −0.27h | 0.137 | 0.25h | 0.161 | 0.32h | 0.078 | −0.25h | 0.176 | −0.26h | 0.160 | −0.12h | 0.530 |
| f 18 | England | 0.01h | 0.981 | 0.39h | 0.107 | −0.42h | 0.086 | −0.33h | 0.182 | −0.44h | 0.066 | −0.07h | 0.796 | −0.50h | 0.036 | −0.24h | 0.339 |
| a 32 | Finland | 0.86h | 0.000 | 0.82h | 0.000 | −0.62h | 0.000 | 0.84h | 0.000 | 0.71h | 0.000 | 0.23h | 0.200 | 0.83h | 0.000 | 0.83h | 0.000 |
| g 15 | France | 0.52h | 0.049 | 0.14h | 0.612 | 0.05h | 0.849 | −0.53h | 0.044 | −0.54h | 0.037 | −0.41i | 0.128 | −0.40i | 0.144 | −0.51h | 0.052 |
| a 32 | Germany | 0.82h | 0.000 | 0.76h | 0.000 | 0.25i | 0.165 | 0.52h | 0.002 | 0.60h | 0.000 | −0.60h | 0.000 | 0.75h | 0.000 | 0.70h | 0.000 |
| a 32 | Iceland | 0.19h | 0.297 | −0.23h | 0.213 | 0.01h | 0.963 | 0.20h | 0.271 | 0.28h | 0.121 | −0.36h | 0.043 | 0.22h | 0.237 | 0.23h | 0.205 |
| g 15 | Italy | −0.64h | 0.011 | 0.67h | 0.007 | −0.45h | 0.092 | 0.67h | 0.006 | 0.44h | 0.098 | 0.55h | 0.035 | 0.48h | 0.072 | 0.34h | 0.215 |
| a 32 | Norway | 0.93h | 0.000 | 0.22h | 0.217 | 0.50i | 0.003 | 0.57i | 0.001 | 0.92h | 0.000 | −0.9h | 0.000 | 0.85h | 0.000 | 0.68h | 0.000 |
| g 15 | Poland | −0.34h | 0.218 | −0.20i | 0.486 | −0.12h | 0.673 | 0.57i | 0.027 | −0.31h | 0.266 | −0.06i | 0.844 | −0.63h | 0.012 | −0.23i | 0.419 |
| c 28 | Scotland | 0.14h | 0.482 | −0.27h | 0.159 | −0.15h | 0.460 | −0.06h | 0.768 | 0.18h | 0.357 | 0.30h | 0.124 | 0.25h | 0.197 | 0.17h | 0.394 |
| e 16 | Spain | −0.77h | 0.000 | 0.83h | 0.000 | −0.24h | 0.366 | 0.18h | 0.495 | 0.65h | 0.006 | −0.53h | 0.034 | 0.51h | 0.045 | 0.27h | 0.304 |
| a 32 | Sweden | 0.60h | 0.000 | 0.50h | 0.004 | 0.23i | 0.207 | 0.26h | 0.155 | 0.64h | 0.000 | −0.21i | 0.249 | 0.60h | 0.000 | 0.47h | 0.007 |
| d 20 | Switzerland | −0.14h | 0.545 | −0.22h | 0.346 | 0.21h | 0.376 | 0.36h | 0.121 | −0.45h | 0.049 | −0.04h | 0.873 | 0.39h | 0.089 | 0.00h | 1.000 |
| b 30 | The Netherlands | 0.63i | 0.000 | 0.53h | 0.003 | 0.50h | 0.005 | 0.02h | 0.904 | 0.10h | 0.614 | 0.69i | 0.000 | 0.69i | 0.000 | 0.02h | 0.904 |
Note: Pearson's or Spearman's correlation coefficients (depending on the underlying distribution of the variable) of dietary variables compared with annual colorectal cancer incidence rates adjusted to the worldwide population per 100,000 inhabitants with a 10-year delay in men and women per country. Alcohol (pure) (L/person/year). Cereals, fruits, vegetables, legumes, poultry, red meat, fish (kg/person/year).
This study has some potential limitations, primarily those due to its ecological design6. These limitations include the inability to control for confounding variables, the use of aggregate per capita consumption data and the ecological fallacy, which prevents conclusions on causation. Additionally, potential sources of error are the accuracy of the data on food consumption provided by the FAO database, differences in cancer registration, and the inability to account for other important factors unrelated to diet.
In 2003, the European Union extended the recommendation of implanting colorectal cancer screening using the fecal occult blood test in the population aged between 50 and 74 years of age7,8. There were few colorectal cancer screening programs in Europe from 1971-2002.
In the analysis of the results, only correlation coefficients ≥|0.75| that were found to be statistically significant and which were calculated with respect to the more prominent food consumption trends (R ≥|0.5|) were considered in order to determine which dietary elements may have influenced the incidence of colorectal cancer.
Excess consumption of red meat9–12 and insufficient consumption of food of vegetable origin13–15 are known to be major risk factors for colorectal cancer. In all of the countries analyzed, positive correlations were established between the incidence of colorectal cancer and red meat consumption, along with negative correlations with cereal consumption. Finland, Germany, Italy, Spain and the Netherlands showed positive correlations between the incidence of colorectal cancer and red meat consumption among men. Among women, positive correlations with red meat were observed in Finland, Germany, Italy, Spain and Sweden. Cereal consumption was negatively correlated with the incidence of colorectal cancer in Finland and Italy in men.
Poultry consumption is considered a protective factor for colorectal cancer11. Among men in the Netherlands, poultry consumption showed a positive correlation with the incidence of colorectal cancer; however, red meat consumption increased more than that of poultry in the same time period (R = 0.7, red meat; R = 0.5, poultry).
Fish consumption is considered a protective factor for colorectal cancer11,12. Fish consumption in both Finland (men and women) and Italy (men only) showed positive correlations with the incidence of colorectal cancer. However, as observed with poultry, red meat consumption increased faster than did fish consumption in the same period (Finland: R = 0.8 red meat, R = 0.5 fish; Italy: R = 0.9 red meat, R = 0.8 fish).
As discussed previously, inadequate consumption of food of vegetable origin is considered a risk factor for colorectal cancer13–15. In all countries with significant correlations, the correlation between the incidence of colorectal cancer and consumption of fruits and vegetables was positive. For fruit consumption, there were positive correlations in England, Finland, Italy, Norway, Scotland and Spain in men and in Norway in women. Vegetable consumption was positively correlated with the incidence of colorectal cancer in Finland, Germany and Sweden in men, and in Finland in women. Only in England, Norway and Scotland was increased consumption of fruits and vegetables not accompanied by a substantial increase in red meat consumption during the same period (red meat: R = 0.8 Finland, R = 0.9 Germany, R = 0.9 Italy, R = 2.1 Spain, R = 0.6 Sweden).
In Europe, the primary source of protein has progressively changed from legumes to red meat in the last few decades, which could be a contributing factor in the increase of colorectal cancer in both genders in this region in recent years. In contrast, poultry and fish consumption have slightly increased compared with red meat consumption, most notably fish consumption.
Substantial differences in incidence rates according to gender, with higher values normally found in men, may be the result of greater exposure to lifestyle-related risk factors, such as dietary habits, smoking, sedentariness, overweight, obesity and diabetes.
In conclusion, the changes in dietary habits may potentially be consistent with the observed trends in the incidence of colorectal cancer in distinct European countries.
A great number of investigations studying colorectal cancer have helped to identify the principal risk and protection factors for this disease. Included among these are certain behaviors that increase the risk of suffering colorectal cancer, especially those which involve unhealthy eating habits. This study analyzes the evolution of the incidence of colorectal cancer in fifteen European countries, and the correlation between recent changes in these rates and changes in dietary habits.
¿Qué añade el estudio realizado a la literatura?The results of this investigation show that there is a tendency toward an increase in the incidence of colorectal cancer in Europe, in both genders, though more pronounced in men, and analyzes the potential contribution that changes in dietary habits have had in these tendencies. We highly recommend the application of legislative and educative measures at the European level in order to promote healthy eating habits, measures that will serve not as a substitution of, but in addition to the screening programs, as well as any advances in the treatment of this disease.
L.M. Béjar participated in the literature search, the design and methodology of the study, the statistical analysis of the results, and the final drafting of the manuscript. M. Gili participated in the study design, the analysis of the results, and the final drafting of the manuscript. B. Infantes participated in the literature search, data collection, the analysis and final presentation of the results, including the design of the tables and figures, and in the final drafting of the manuscript. P.F. Marcott participated in data collection, the statistical analysis of the results, and the final drafting of the manuscript.
FundingNone.
Conflicts of interestNone.











