




To analyze patient's reported elements of relational, informational and managerial (dis)continuity between primary and outpatient secondary care and to identify associated factors.
MethodsCross-sectional study by means of a survey of a random sample of 1500 patients attended in primary and secondary care for the same condition. The study settings consisted of three health areas of the Catalan health system. Data were collected in 2010 using the CCAENA© questionnaire, which identifies patients’ experiences of continuity of care. Descriptive analyses and multivariable logistic regression models were carried out.
ResultsElements of continuity of care were experienced by most patients. However, elements of discontinuity were also identified: 20% and 15% were seen by more than one primary or secondary care physician, respectively. Their secondary care physician or both professionals were identified as responsible for their care by 40% and 45% of users, respectively. Approximately 20% reported a lack of information transfer. Finally, 72% of secondary care consultations were due to primary care referral, whilst only 36% reported a referral back to primary care. Associated factors were healthcare setting, age, sex, perceived health status and disease duration.
ConclusionUsers generally reported continuity of care, although elements of discontinuity were also identified, which can be partially explained by the healthcare setting and some individual factors. Elements of discontinuity should be addressed to better adapt care to patients’ needs.
Analizar los elementos de (dis)continuidad de relación, información y gestión, entre atención primaria y secundaria ambulatoria, reportada por los pacientes e identificar los factores asociados.
MétodosEstudio transversal, mediante encuesta a usuarios de los servicios de salud atendidos en atención primaria y secundaria por un mismo motivo. Se realizó en tres áreas del sistema de salud de Cataluña. Se seleccionó una muestra aleatoria de 1500 pacientes. Los datos fueron recogidos en 2010 aplicando el cuestionario CCAENA©, que mide la experiencia y la percepción de la continuidad asistencial. Se realizaron análisis descriptivos y modelos de regresión logística múltiple.
ResultadosLos usuarios percibieron mayoritariamente elementos de continuidad asistencial. Sin embargo, también identificaron elementos de discontinuidad: un 20% y un 15%, respectivamente, fueron atendidos por más de un médico de atención primaria o secundaria. Un 40% identificó como responsable de su atención al médico de atención secundaria y un 45% a ambos profesionales. Aproximadamente el 20% percibió una falta de transferencia de información. Finalmente, el 72% de las consultas a médicos de atención secundaria fue por derivación de atención primaria, y sólo el 36% señaló una contraderivación a la atención primaria. Los factores asociados fueron el área de salud, las características sociodemográficas, el estado de salud percibida y la duración de la enfermedad.
ConclusiónLos usuarios perciben una continuidad asistencial, aunque identifican elementos de discontinuidad, explicados parcialmente por el área de salud y por algunos factores individuales. Su abordaje contribuiría a adecuar la atención a las necesidades de los pacientes.
The achievement of continuity of care (CC) poses one of the greatest challenges for all healthcare systems due to rapid technological advances, new treatments, high specialisation, and shifts in care from institutional to outpatient and home settings. Patients therefore see an ever-expanding array of different providers in a variety of places, which makes the coordination of their care difficult and jeopardizes care continuity.1–3 Following Reid et al.,1 CC is here defined as the degree to which patients experience care over time as coherent and linked1. Three types of continuity are identified1,4:
- •
Relational: the patients’ perceptions of an ongoing, therapeutic relationship with one or more providers.
- •
Informational: patients’ perceptions of the availability, use and interpretation of information on past events in order to provide care which is appropriate to their current circumstances.
- •
Managerial: the patients’ perceptions that they are receiving the different services in a coordinated, complementary and unduplicated way.
Only few studies have so far analysed patients’ experiences of CC in a comprehensive manner, i.e. taking into account the three types of CC, a wide range of medical conditions or different care levels1; studies have generally focused on a single pathology,5,6 or one care level,7,8 or encompassed a small sample size.5,6 Regarding associated factors, only one study has associated patients’ CC reports with healthcare elements: the existence of specific care coordination mechanisms between organizations (healthcare protocols and mechanisms to facilitate referral or sharing of information).9 Most available studies have concentrated on the influence of individual factors, with diverse results: while sex does not seem to be related to CC perceptions,5,6,10,11 the influence of age is inconclusive5,6,10,11 and there appears to be an inverse relationship with educational level.10,12 Ethnic minorities give a worse assessment of primary care (PC) elements related to relational continuity13-15; but the influence of immigrant status on relational continuity remains unexplored, and the impact of morbidity is inconclusive.16,17 Patients with increased morbidity seem to be more likely to experience low levels of informational and managerial continuity.16,18
CC has also become a priority of the Catalan National Health System, in which primary care is the gatekeeper, and secondary care (SC) is responsible for the treatment of severe conditions.19 In order to ensure CC, citizens are assigned to a PC team that coordinates their care along the care continuum.20,21 This means that access to outpatient SC requires referral from PC.21 In the Catalonian health system, care is provided by a number of contracted providers: on the one hand, a public company, the Catalan Health Institute (ICS), and on the other, consortia, municipal foundations and private foundations (mainly non-profit but also for-profit).22 This diversity has given rise to various management models under both public and private law, including the independent or joint management of both PC and SC in the different healthcare areas into which the system is divided.23 How these different management models may influence CC has so far not been explored. The aim of this article, part of a wider study,24,25 is to analyse patient-reported elements of relational, informational and managerial (dis)continuity between PC and outpatient SC and to identify context and individual associated factors.
MethodsStudy design and settingA cross-sectional study was carried out by means of a survey of users of the Catalan public healthcare system in three selected areas: Baix Empordà, the city of Girona and the Ciutat Vella district of Barcelona. Healthcare areas were selected to explore the potential influence of healthcare factors on CC experiences, specifically the different management models for PC and SC levels: in Baix Empordà and Girona both PC and SC are managed by a single entity, under private law in the former case and under public law in the latter. In Ciutat Vella, PC and SC are managed by independent entities under public and private law. The population served by these organizations in the study areas is 74,144 in Baix Empordà, 83,312 in Girona and 99,093 in Ciutat Vella. All three areas have introduced some coordination mechanisms between care levels, such as shared clinical guidelines and protocols. In terms of information systems, in Baix Empordà, patients have a single electronic medical record for both care levels, whilst in the other two areas electronic records are shared but different.
Study population and sampleThe study population consisted of patients of 18 years of age or over who had received PC and SC for the same condition in the three months prior to the survey and were assigned to the selected healthcare areas.
Sample size was calculated to analyse the association model between variables at 95% confidence level, to fulfil the de Moivre theorem of expected frequency greater than five as well as to express the fit and likelihood statistics as a chi-square distribution. The sample size required was approximately 400 patients per healthcare area. The final sample size was 1500 and the sample was distributed across the three areas according to the size of served population.
A simple random sample without replacement was selected from the records provided by the study area PC centres and hospitals which permitted the identification of the patients that had used both PC and SC in the three months prior to the interview for the same condition. A list of substitutes which included individuals of the same sex and age group was used to replace any refusals. Patients who had not been attended to by medical professionals or who could not understand or communicate effectively in Spanish or Catalan were excluded.
QuestionnaireThe CCAENA questionnaire was applied, which is designed to comprehensively evaluate patients’ experiences of CC between care levels. This tool, previously validated,25 is divided into two sections. The first reconstructs the care trajectory for a specific condition in the previous year for relational continuity and the last three months for informational and managerial continuity; and identifies the elements of (dis)continuity experienced in the transition between PC and outpatient, hospital and emergency SC. This paper focuses on the transitions between PC and outpatient SC (see Table I in the Appendix on the online version in this article). The second section, is for patients to evaluate CC via Likert scales.
Data collectionData were collected by face-to-face interviews conducted by trained interviewers, from January to May 2010. Interviews were carried out mainly in the patients’ PC centre (93.7%), and some in their homes (6.1%) or other locations (0.2%). Patients were contacted first by mail and then invited to participate by telephone.
Of the patients contacted, 77.5% refused to take part in the study. There were no statistically significant differences between the final sample and the population of study in terms of sex and age. The highest rate of refusals was observed in Barcelona (80.7%), followed by Baix Empordà (77.6%) and Girona (70.3%).
Variables- •
Dependent variables: elements of the three types of CC in the transition between PC and outpatient SC, as reported by patients. Regarding relational continuity, the stability of the medical team was defined as the reported number of general practitioners (GP) and SC physicians who had treated the patient for the same condition (one or more than one physicians during the last year). The transfer of medical information (informational continuity) was evaluated through the patient's reports of the health professionals’ awareness of: a) the reason for their visit (yes/no), and b) the instructions received at the other care level (yes/no). Lastly, consistency of care (managerial continuity) was evaluated by means of patients’ reports of the way they accessed SC and PC (referral from the other care level or other means, e.g. referral from the same care level or a follow-up visit).
- •
Individual and contextual independent variables: the individual variables were those that the literature indicates as potential factors influencing patients’ experiences of care5,6,9–17: socio-demographic characteristics (sex, age, education level and immigration status) and declared morbidity (perceived state of health and duration of the condition which prompted them to visit the health services). The contextual variable refers to the healthcare area in which the patient receives medical care.
A descriptive analysis was conducted of patients’ experiences of continuity in the transition from PC to outpatient SC and vice versa, calculating frequencies and 95% confidence intervals. Following this, a series of logistic regression models were generated in order to evaluate the relationship between variables. Robust covariance adjustments (employing the healthcare area variable) were used to account for correlated observations due to clustering.26 Adjusted ORs and their corresponding 95% confidence intervals were obtained. Statistical analyses were carried out using Data Analysis and Statistical Software (STATA), version 11.
Ethical considerationsThe study was conducted in accordance with the current European and Spanish legislation on ethical research. Informed consent was obtained from every interviewee participating in the survey and confidentiality of data was assured through anonymous analysis. The protocol was approved by the Ethical Committee for Clinical Research Parc Salut Mar (2009/3414/I).
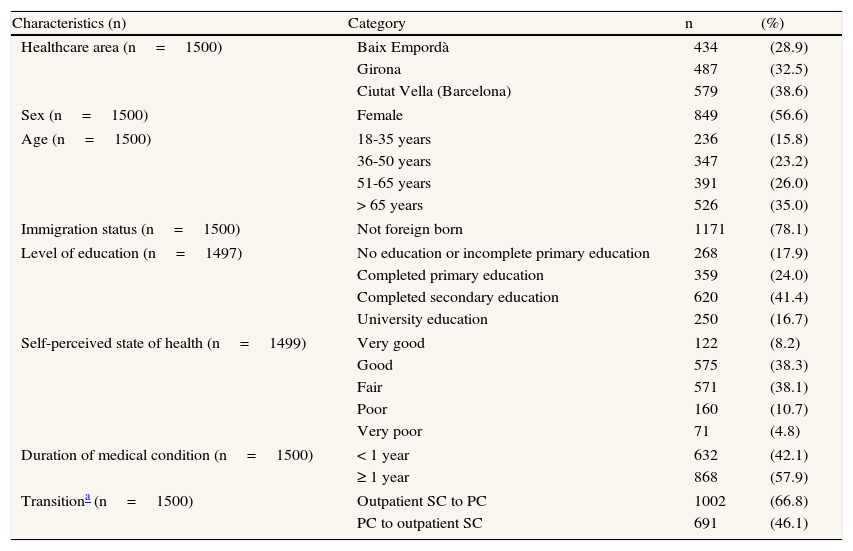
ResultsOver half of the interviewees (56.6%) were women and 78.1% were born in Spain; and the sample was homogenously distributed across the different age groups. State of health was reported as being good or very good by 46.5% of patients and 42.1% of patients reported a duration of their condition of less than one year. Within the last three months before the interview, 66.8% of interviewees (1002) had gone to PC after having received outpatient SC while only 46.1% (691) were undergoing the opposite transition (Table 1).
Characteristics of the sample and transition characteristics.
| Characteristics (n) | Category | n | (%) |
| Healthcare area (n=1500) | Baix Empordà | 434 | (28.9) |
| Girona | 487 | (32.5) | |
| Ciutat Vella (Barcelona) | 579 | (38.6) | |
| Sex (n=1500) | Female | 849 | (56.6) |
| Age (n=1500) | 18-35 years | 236 | (15.8) |
| 36-50 years | 347 | (23.2) | |
| 51-65 years | 391 | (26.0) | |
| > 65 years | 526 | (35.0) | |
| Immigration status (n=1500) | Not foreign born | 1171 | (78.1) |
| Level of education (n=1497) | No education or incomplete primary education | 268 | (17.9) |
| Completed primary education | 359 | (24.0) | |
| Completed secondary education | 620 | (41.4) | |
| University education | 250 | (16.7) | |
| Self-perceived state of health (n=1499) | Very good | 122 | (8.2) |
| Good | 575 | (38.3) | |
| Fair | 571 | (38.1) | |
| Poor | 160 | (10.7) | |
| Very poor | 71 | (4.8) | |
| Duration of medical condition (n=1500) | < 1 year | 632 | (42.1) |
| ≥ 1 year | 868 | (57.9) | |
| Transitiona (n=1500) | Outpatient SC to PC | 1002 | (66.8) |
| PC to outpatient SC | 691 | (46.1) | |
PC: primary care; SC: secondary care.
In the last year and due to the same condition, 79.7% of interviewees reported to have been seen by the same GP and 84.9% by the same SC physician (taking into consideration only one medical specialization). When asked about the main professional responsible for managing their condition, 40.7% of interviewees identified the SC physician and 45.0% identified both professionals (see Table II in the Appendix on the online version in this article).
Informational continuityMost interviewees (82.0%) reported that the SC physician was aware of the reason for their visit and 81.5% that he/she was aware of the tests carried out at PC level. Likewise, 81.3% of patients reported that the GP was aware of the instructions received at SC level and 84.7% of the treatment prescribed (see Table II in the Appendix on the online version in this article).
Managerial continuityWith regard to consistency of care, 71.6% of patients reported that outpatient SC consultations that followed a PC visit were due to a referral from that care level, whilst only 36.0% of patients reported that PC consultations that followed an outpatient SC visit were due to a referral from the SC level. Most patients (87.6%) reported that the GP resolved doubts regarding their visit to the SC professional, and 72.0% and 68.6% of interviewees considered that professionals were coordinated regarding the transitions between PC and SC. With regard to accessibility between care levels, 41.6% and 19.0% of interviewees respectively held the opinion that waiting time to be seen at the referral level, SC or PC, was long or excessive (see Table II in the Appendix on the online version in this article).
Associated factors- •
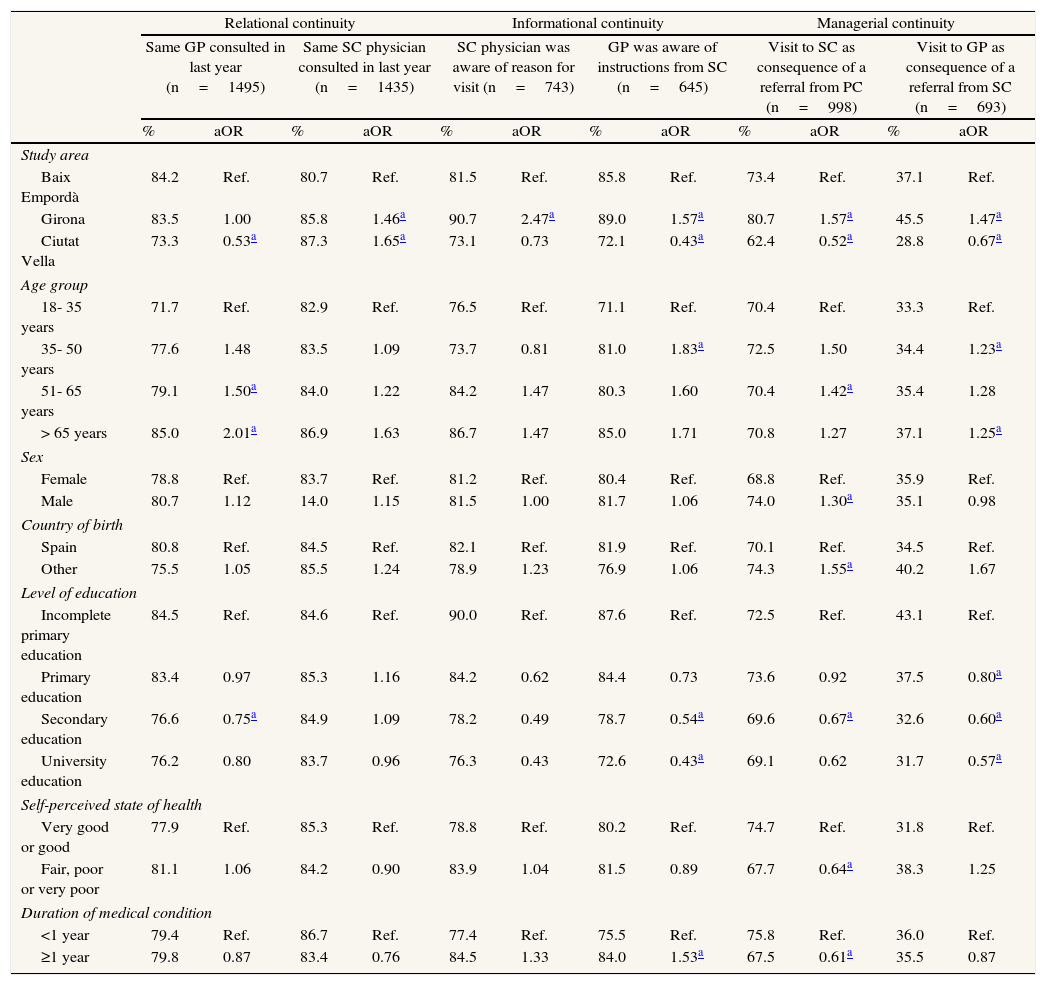
Healthcare area: the healthcare area was associated with all types of continuity. Patients from Girona were more likely to report to have been seen by the same GP in the last year, to experience informational transfer across care levels and referral to the other care level (SC and PC) than patients from the other healthcare areas; likewise patients from Baix Empordà, as compared with those from Ciutat Vella. Additionally, patients from Girona and Ciutat Vella were more likely to report to have been treated by the same SC physician than those of Baix Empordà (Table 2).
Table 2.Continuity of care perceived by patients, results of the logistic regression analysis.
Relational continuity Informational continuity Managerial continuity Same GP consulted in last year (n=1495) Same SC physician consulted in last year (n=1435) SC physician was aware of reason for visit (n=743) GP was aware of instructions from SC (n=645) Visit to SC as consequence of a referral from PC (n=998) Visit to GP as consequence of a referral from SC (n=693) % aOR % aOR % aOR % aOR % aOR % aOR Study area Baix Empordà 84.2 Ref. 80.7 Ref. 81.5 Ref. 85.8 Ref. 73.4 Ref. 37.1 Ref. Girona 83.5 1.00 85.8 1.46a 90.7 2.47a 89.0 1.57a 80.7 1.57a 45.5 1.47a Ciutat Vella 73.3 0.53a 87.3 1.65a 73.1 0.73 72.1 0.43a 62.4 0.52a 28.8 0.67a Age group 18- 35 years 71.7 Ref. 82.9 Ref. 76.5 Ref. 71.1 Ref. 70.4 Ref. 33.3 Ref. 35- 50 years 77.6 1.48 83.5 1.09 73.7 0.81 81.0 1.83a 72.5 1.50 34.4 1.23a 51- 65 years 79.1 1.50a 84.0 1.22 84.2 1.47 80.3 1.60 70.4 1.42a 35.4 1.28 > 65 years 85.0 2.01a 86.9 1.63 86.7 1.47 85.0 1.71 70.8 1.27 37.1 1.25a Sex Female 78.8 Ref. 83.7 Ref. 81.2 Ref. 80.4 Ref. 68.8 Ref. 35.9 Ref. Male 80.7 1.12 14.0 1.15 81.5 1.00 81.7 1.06 74.0 1.30a 35.1 0.98 Country of birth Spain 80.8 Ref. 84.5 Ref. 82.1 Ref. 81.9 Ref. 70.1 Ref. 34.5 Ref. Other 75.5 1.05 85.5 1.24 78.9 1.23 76.9 1.06 74.3 1.55a 40.2 1.67 Level of education Incomplete primary education 84.5 Ref. 84.6 Ref. 90.0 Ref. 87.6 Ref. 72.5 Ref. 43.1 Ref. Primary education 83.4 0.97 85.3 1.16 84.2 0.62 84.4 0.73 73.6 0.92 37.5 0.80a Secondary education 76.6 0.75a 84.9 1.09 78.2 0.49 78.7 0.54a 69.6 0.67a 32.6 0.60a University education 76.2 0.80 83.7 0.96 76.3 0.43 72.6 0.43a 69.1 0.62 31.7 0.57a Self-perceived state of health Very good or good 77.9 Ref. 85.3 Ref. 78.8 Ref. 80.2 Ref. 74.7 Ref. 31.8 Ref. Fair, poor or very poor 81.1 1.06 84.2 0.90 83.9 1.04 81.5 0.89 67.7 0.64a 38.3 1.25 Duration of medical condition <1 year 79.4 Ref. 86.7 Ref. 77.4 Ref. 75.5 Ref. 75.8 Ref. 36.0 Ref. ≥1 year 79.8 0.87 83.4 0.76 84.5 1.33 84.0 1.53a 67.5 0.61a 35.5 0.87 GP: general practitioner; PC: primary care; SC: secondary care; aOR: odds ratio adjusted for the other variables in the table; Ref., reference category.
- •
Individual factors: age was associated with all types of continuity of care, but not all continuity elements. Age was particularly associated with the probability of having been seen by the same GP in the last year, the consulted GP being aware of SC instructions, and reporting a visit to PC or SC as a consequence of a referral from the other care level; older patients were more likely to report these elements of continuity than younger ones. Sex and immigration status were associated with managerial continuity; male patients and immigrants were more likely to report a visit to SC via a referral from PC than women and the native population. Patients with lower education levels were more likely to report to have been treated by the same GP, that their GP was aware of the instructions from SC, and to have visited one care level due to referral from the other than more educated patients (Table 2).
- •
Health-related factors: patients who perceived their state of health as good or very good were more likely to report a visit to SC due to a referral from PC than patients with a fair, poor or very poor self-perceived health status. Patients with a medical condition that had lasted more than one year were more likely to report that the GP was aware of the instructions given in SC than those whose medical condition had lasted less than one year. The inverse relationship was observed regarding the probability of consulting SC as a consequence of a referral from PC (Table 2).
This study represents the first attempt to comprehensively analyse patient-reported elements of healthcare continuity in the transition between PC and outpatient SC. It adds that it analyses elements related to the three types of CC, experienced by patients with different socio-demographic characteristics and suffering from a wide range of medical conditions. The selection of three healthcare areas with different managerial models allowed establishing their potential influence on CC experiences; and the heterogeneous sample, to further analyse the contribution of individual factors to CC experiences.
However, the study presents some limitations. Firstly, 77.5% of contacted patients refused to participate. Although they were replaced by others belonging to the same age group and sex, a non-response bias cannot be excluded. This would lead to the underrepresentation of certain population groups, and consequently would limit the inference capacity of the obtained results to the study population. Secondly, conducting the interviews mostly in the PC centres could have influenced results; however, results are consistent with those from the pilot test,24 in which the majority of interviews were conducted outside the PC centres.25 Lastly, due to the scarcity of studies, it is possible that not all of the variables relevant to explaining CC were considered.
Elements of healthcare related to (dis)continuityTransitions between PC and outpatient SC were mostly reported as connected and consistent; however, some noteworthy elements of discontinuity were identified. In terms of informational continuity, the results highlighted gaps in the transfer of information. Even if the figures indicate better informational continuity than in other contexts,27,28 they should receive attention, due to the fact that lack of communication across levels is the most frequent cause of patients experiencing poor quality healthcare.29,30 In terms of managerial continuity, elements related to inaccessibility across levels and inconsistency of care arose: a significant percentage of patients considered waiting times inadequate, as described by other studies24,31; over a quarter of patients perceived that care received was not coordinated; and, they reported a low percentage of visits to PC and SC due to referrals from the other care level. Low referral rates may contribute to the perception of lack of coordination,27 and future research should examine whether this low level of referral is consequence of the patients’ lack of information or retention of patients at the SC level.
In terms of relational continuity, it is remarkable the high proportion of patients that identified the SC physician as the main professional responsible for managing their condition. This could be related to low back-referral figures from SC24 or to the patient attributing higher technical competence to SC professionals. Nevertheless, and according to other studies, this does not seem to be jeopardising the patient-GP relationship.24
Factors associated with patients’ experiences of (dis)continuityPatients attended to in organizations in which PC and SC were managed by the same entity experienced more healthcare elements related to continuity, and the most favourable of these reports was given by patients who were attended to at the services managed by a single entity under public law. The implementation of specific coordination strategies might serve to explain the differences observed.
In terms of the individual factors related to experienced CC, an inverse relationship was identified between informational and managerial CC reports and level of education. Available studies suggest that more educated patients have higher expectations,12 judge quality more critically32 and elicit more information.33 Foreign-born patients were more likely to report being referred from PC to SC, reasons for that could be: native population accesses care more often in non-conventional ways; professionals perceive a greater need for care coordination when treating foreign-born patients to reinforce their decisions; or finally, the work overload attributed to foreign-born patients34 encourages professionals to refer them more frequently. However, aspects mediating these results need to be explored.
Patients with a longer duration of medical condition experienced higher levels of informational continuity, in contrast to other studies.16,18 This different result could be due to the patients’ seeing more frequently their physicians, favouring the perception that they have the information they need about their case, or to the existence of specific programs for patients with chronic conditions
In conclusion, patients experienced in the transition between PC and outpatient SC high levels of healthcare elements related to CC, particularly relational continuity. However, identified elements of discontinuity indicate a margin for improvement in healthcare provision. This study is the first to show an association between experiences of all types of CC and healthcare setting. However, this relation needs to be further explored in order to determine which organizational elements might be contributing to enhance CC. Further research is also needed to understand reasons underlying the differences observed in CC experiences between patients. To make progress on those areas, services and professionals perspectives should also be explored. Finally, this research was conducted before two important events of the Catalan healthcare system took place: the reduction in the healthcare budget and the split of the major public provider into different public companies to manage separately PC and SC in the area of study. As such, it will provide a base-line to analyse the potential impact of these measures on healthcare provision.
Few studies have analysed patients’ experiences of continuity of care in a comprehensive manner; studies have generally focused on one type of continuity, a single pathology or one care level. Evidence regarding the association of morbidity and certain patients’ sociodemographic characteristics on their experiences of continuity of care is inconclusive. Only one study in the international literature has associated patients’ reports on continuity of care with elements of healthcare services.
What does this study add to the literature?This study has applied the CCAENA questionnaire, which is one of the few existing tools that comprehensively analyse continuity of care, and the only tool validated in the Catalan healthcare system. This is the first attempt to comprehensively analyse patient-reported healthcare elements of continuity in the transition between primary and outpatient secondary care. The study shows high levels of continuity of care in the Catalan public health care system and for the first time an association between the experiences of all types of continuity of care and healthcare setting.
M. Aller was responsible for the supervision of the fieldwork, design, implementation and interpretation of data analysis and writing of the paper. Ingrid Vargas contributed to the study conception, design and implementation and writing of the paper. I. Sánchez designed the sample and I. García collaborated in the statistical analyses. J. Coderch participated providing operational and methodological support to the field work; and together with J.R. Llopard, L. Colomés and M. Ferrán participated as experts in healthcare systems in all project phases. M.L. Vázquez was responsible for the study design and supervision of all phases of the research and writing the article. All authors participated in data interpretation, reviewed draft versions of the paper and approved the final version.
FundingThis research was partially financed by Plan de Acción Estratégica en Salud, Proyectos de investigación en salud del Instituto de Salud Carlos III (PI10/00348).
Conflicts of interestsNone.
The authors are most grateful to Silvina Berra, Maribel Pasarín, Josep María Argimon and Soledad Romea for their support to the conceptual and practical development of the study. They would also like to express their gratefulness to Francesc Cots, Lola Bosch, Josep Maria Lisbona, Isabel Serra, Juan Antonio Camús and Montserrat Figuerola, for their support that was essential for the development of the research.












