

In most European countries, facemasks use is recommended or mandatory in enclosed spaces where physical distancing is not possible. In Spain, this measure was first extended to open public spaces and later made mandatory regardless of whether or not the interpersonal safety distance can be kept. At present, there is no evidence on the effectiveness of universal masking of healthy people in the community to prevent infection with respiratory viruses, including SARS-CoV-2. The mandatory use of masks poses some ethical questions. Firstly, it entails a paternalistic action. Secondly, application of the principle of precaution becomes questionable when there is no clear benefit-risk relationship. Thirdly, compulsoriness can interfere with equity of public health actions. Fourthly, it can result in social stigma and discrimination against those who do not wear one, even though they well may have good reasons for doing so. Lastly, this measure may generate confusion in the population, along with an altered perception of the risk. The World Health Organization recommends its use in public places with a high potential risk of transmission and where other prevention measures, such as physical distancing, are not possible. Mandatory use of masks in public open spaces, regardless of the risk of transmission or of whether or not the interpersonal safety distance can be kept, is an intrusive measure that restricts individual freedoms, and would not appear to be justified on the basis of available scientific evidence. What we need are recommendations explaining where, when, how and what type of mask to wear.
En la mayoría de los países europeos, el uso de mascarillas es recomendado u obligatorio en espacios cerrados donde no es posible mantener la distancia física de seguridad. En España, la obligatoriedad se amplió primero a los espacios públicos abiertos y más tarde independientemente de la distancia de seguridad. En la actualidad no hay pruebas de la efectividad del uso universal de mascarilla para prevenir el contagio de virus respiratorios, incluido el SARS-CoV-2. El uso obligatorio de mascarilla plantea cuestiones éticas. Primero, implica una acción paternalista. Segundo, la aplicación del principio de precaución es cuestionable cuando no existe una relación clara beneficio-riesgo. Tercero, puede interferir en la equidad de las acciones de salud pública. Cuarto, puede dar lugar a un estigma social y a la discriminación de quienes no hacen uso de ella, aunque tengan buenas razones para ello. Por último, esta medida puede generar confusión en la población, junto con una percepción alterada del riesgo. La Organización Mundial de la Salud recomienda su uso en lugares públicos con un alto riesgo de transmisión y donde no sea posible aplicar otras medidas de prevención, como la distancia física. El uso obligatorio de mascarilla en espacios públicos abiertos, independientemente del riesgo de transmisión o de que se pueda o no mantener la distancia de seguridad, es una medida intrusiva que restringe las libertades individuales y no parece justificarse sobre la base de las pruebas científicas disponibles. Lo que necesitamos son recomendaciones explicando dónde, cuándo, cómo y qué tipo de mascarilla usar.
The use of face masks in public spaces has become a political issue in some countries. In the United States, the President Trump has changed his mind from rejecting the use of face masks in public1 to say that it is patriotic to wear a face mask when you can’t socially distance.2 In most European countries, face masks use is recommended or mandatory in public transport and enclosed spaces where physical distancing is not always possible.3 In Spain, this measure, first limited to public transport, was extended on May 20 to open public spaces: the use of face masks is compulsory for all persons over the age of six, whether in the street, outdoors, or in closed spaces used by or open to the public, in all cases where it would not be possible to maintain a safe interpersonal distance of at least 1.5 metres.4 Finally, in all regions of Spain the use of face masks has been made mandatory in most circumstances throughout the months of July and August, regardless of whether or not the interpersonal safety distance can be kept.5
Generalised use of face masks by the general public to reduce community transmission of COVID-19 was first justified on the principle of precaution.4 The argument put forward to extend this measure to all circumstances is extremely attractive and tempting, i.e., the compulsory wearing of masks would serve to avoid more restrictive measures affecting individual liberties.6 If it were in fact true that their use outdoors could prevent future lockdowns, nobody well aware of it would leave home without wearing one. However, we are afraid that this is not the case. Unfortunately, the evolution of the pandemic is getting worse in Spain since mid July, in spite of the generalized use of masks following the new mandatory regulations.7
In this article we analyze the scientific basis and the ethical implications of the mandatory use of face masks as it has been implemented in Spain, including settings where there is a very low risk of transmission (open, uncrowded spaces) even in situations where it is possible to maintain the safety distance.
The scientific evidenceWhat does science have to say about the use of face masks by the general healthy population? After reviewing the pertinent scientific evidence, the World Health Organization (WHO), in its interim guidance on the topic published on 6 April, reached the following conclusion: “The wide use of masks by healthy people in the community setting is not supported by current evidence and carries uncertainties and critical risks”.8 These guidelines were updated on 5 June to include new relevant scientific evidence on the use of face masks in the prevention of COVID-19 transmission.9 The conclusion reached is very similar: “At present, there is no direct evidence (from studies on COVID19 and in healthy people in the community) on the effectiveness of universal masking of healthy people in the community to prevent infection with respiratory viruses, including COVID-19”. Nonetheless, the guide advises that the following criteria be borne in mind when considering whether to recommend the use of masks to the general public:
- •
Purpose of mask use: source-control of emissions, or prevention by protecting healthy wearers against infection.
- •
Risk of exposure to the COVID-19 virus.
- •
Vulnerability of the mask wearer.
- •
Setting in which the population lives: population density (e.g., cramped living conditions, refugee camps), and settings where individuals are unable to keep a physical distance of at least 1 metre (e.g., public transportation).
- •
Feasibility: costs, availability, etc.
- •
Type of mask: medical or non-medical.
Based on these criteria, the WHO recommends the use of non-medical masks (or medical masks for people aged ≥60 years and anybody with underlying comorbidity associated with a worse COVID-19 prognosis) in the following circumstances:
- •
People living in cramped conditions, and specific settings such as refugee camps, camp-like settings, slums.
- •
Use of public transport or specific working conditions which place the employee in close contact with many people (e.g., social workers, cashiers, waiters).
- •
General population in public settings, such as grocery stores, at work, social gatherings, mass gatherings, closed settings, including schools, churches, mosques, etc. This recommendation is confined to areas with known or suspected widespread transmission and limited or no capacity to implement other containment measures, such as physical distancing, contact tracing, appropriate management (testing, isolation and care for suspected and confirmed cases).
Medical masks have demonstrated their ability to reduce detection of influenza virus RNA in respiratory droplets and coronavirus RNA in aerosols, with a trend towards reduced detection of coronavirus RNA in respiratory droplets.10 Non-medical masks, on the other hand, are as much as three time less effective in the control of emission of microorganisms.11 A recent systematic review and meta-analysis of the scientific literature, which analysed 172 observational studies conducted in 16 countries across all continents, found that a physical distance of more than one metre is highly effective in the prevention of virus transmission.12 The scientific data that support the preventive effect of wearing masks by the general population are of low quality, and come, in the majority of cases, from studies focusing on homes or case contacts. Risk of transmission depends on the intensity and duration of contact,13 two factors found in the family environment, where wearing a mask has been shown to be effective for reducing transmission.14 However, it is not clear whether mask use outdoors is related to the low COVID-19 rates in some countries, since this is just one of the many measures applied in places where there are excellent epidemiological surveillance systems with a proven capacity to control new COVID-19 outbreaks fast and effectively,15 and where good hand-hygiene practices and respiratory etiquette have long been widespread among the population,16 unlike European countries, like Spain, where efforts have only recently begun to raise public awareness about the importance of such measures. The recommendation to the general healthy population to wear a mask, reserved for settings with a high risk of transmission, is a measure that is complementary to those required for basic prevention, namely:
- •
Avoiding crowded places and situations as far as possible.
- •
Maintaining a safe interpersonal distance of at least one metre, especially in the case of people with respiratory symptoms.
- •
Washing the hands frequently.
- •
Maintaining respiratory etiquette at all times.
Unlike most countries of the European Union, in Spain is mandatory for the general public to wear a face mask in all cases where it would otherwise not be possible to maintain a physical distance of 1.5 metres,4 without drawing any distinction between situations of high potential risk of transmission, such as closed crowded spaces (bars, restaurants, workplaces, churches, musical halls, gymnasiums or health facilities) where people remain for prolonged periods of time, singing or talking loudly,15,17–21 and those in which the risk of transmission can be considered nil or negligible, such as when meeting another person while walking along the street.22 All regions of Spain have gone further, making the use of masks mandatory in most circumstances, although the safety distance can be maintained.5
A group of researchers has made an appealing to the medical community and to the relevant national and international bodies to recognize the potential for airborne spread of COVID-19,23 based on three types of evidence:
- •
Flow physics studies of exhaled droplets movements in indoor environments showing that at typical indoor air velocities, a 5μm droplet can travel more than two metres while settling from a height of 1.5 m to the floor.
- •
Studies showing that influenza viruses are released during exhalation, talking, and coughing in microdroplets small enough to remain aloft in air and pose a risk of exposure at distances beyond 2 metres from an infected individual. Furthermore, in health care settings, viral RNA associated with droplets smaller than 5μm has been detected in air.
- •
Anecdotical retrospective studies of spreading events in high transmission risk environments, like a chorale or a restaurant, where airborne appears to be a plausible explanation for SARS-CoV-2 transmission.
The WHO updated on July 9 a scientific article from March 29 on modes of transmission of SARS-CoV-2 and their implications for prevention and control recommendations, including new scientific evidence available on transmission of the virus that causes COVID-19.24 Regarding potential air transmission, the WHO reaches the following conclusions:
- •
In health care settings where symptomatic COVID-19 patients were cared for, but where aerosol generating procedures were not performed, the quantity of SARS-CoV-2 RNA detected was in extremely low numbers in large volumes of air and no studies have found viable virus (indicative of replication —and infection— competent) in air samples.
- •
Recent clinical reports of health workers found no nosocomial transmission in that context when contact and droplet precautions were appropriately used, excluding aerosol transmission.
- •
In high transmission risk environments where airborne transmission cannot be ruled out, such as during choir practice, in restaurants or in fitness classes, a detailed investigation suggest that droplet and fomite transmission could also explain human-to-human transmission within these clusters previously described.
- •
SARS-CoV-2 transmission appears to mainly be spread via droplets and close contact with infected symptomatic or pre-symptomatic cases.
Taking into account these pieces of evidence, the WHO recommends the use of face masks in public places where there is community transmission and where other prevention measures, such as physical distancing, are not possible. For more detailed advice on the use of masks in the context of COVID-19 it refers to its June 5 Interim guidance.9 In addition, the WHO encourages, at all times, to practice frequent hand hygiene, physical distancing from others when possible, and respiratory etiquette; avoid crowded places, close-contact settings and confined and enclosed spaces with poor ventilation; wear fabric masks when in closed, overcrowded spaces to protect others; and ensure good environmental ventilation in all closed settings and appropriate environmental cleaning and disinfection.
Ethical implicationsThe imposition of the mandatory use of face masks, especially in settings where there is a low risk of transmission (open, uncrowded spaces), poses some ethical questions. Firstly, it entails a paternalistic action by the authorities, which tend to treat citizens like children. It is more important, and would be more respectful, to inform them appropriately about contexts that pose a high risk of transmission where wearing a mask might be of some benefit, and the possible risks associated with incorrect fitting, use or removal. Public health measures need to enlist the full force of individual responsibility, something that is better attained with measures which are less restrictive of individual freedoms, such as persuasion and the power of conviction, than with compulsory measures and penalties.25 Moreover, clear and trustworthy public communication on the part of governments, providing transparent and convincing justifications for the decisions taken, is particularly important in helping create and maintain such trust.26 It is true that public health policies sometimes require paternalistic and mandatory measures to protect population health and prevent disease, but these measures must be considered as a last resort when no other non-mandatory measures can be applied. But they must be evidence-based and necessary to achieve the public health goals intended, which is not the case for facemasks in general population.
Secondly, the principle of precaution may justify the use of coercive measures that limit individual freedoms in order to prevent a possibly serious risk to the health of the population. However, their application becomes more questionable when measures are applied for which there is no clear benefit-risk relationship, as in the case now before us (Table 1). Additionally, the substantial financial resources required to maintain the continued use of masks by the general public could be better allocated to other public health measures of tried and tested efficacy, such as the promotion of the appropriate respiratory etiquette and hand hygiene. What is more, if it were to be shown that the benefit of compulsory use of masks in Spain was outweighed by the potential risks associated with their misuse (an apparently common phenomenon, judging by what one sees daily in TV news bulletins or on any city street), we would be confronted with a prejudicial health intervention which failed to comply with the maxim “primum non nocere” (first, do no harm), a precept that should govern all health actions.
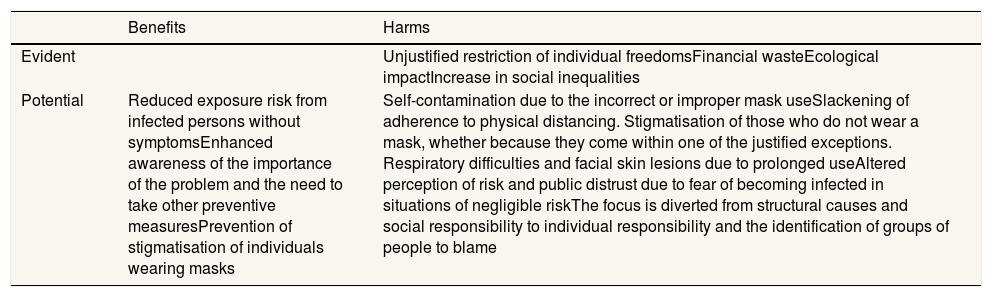
Benefits and risks of mandatory mask use in settings where there is a negligible risk of transmission (open, uncrowded spaces).
| Benefits | Harms | |
|---|---|---|
| Evident | Unjustified restriction of individual freedomsFinancial wasteEcological impactIncrease in social inequalities | |
| Potential | Reduced exposure risk from infected persons without symptomsEnhanced awareness of the importance of the problem and the need to take other preventive measuresPrevention of stigmatisation of individuals wearing masks | Self-contamination due to the incorrect or improper mask useSlackening of adherence to physical distancing. Stigmatisation of those who do not wear a mask, whether because they come within one of the justified exceptions. Respiratory difficulties and facial skin lesions due to prolonged useAltered perception of risk and public distrust due to fear of becoming infected in situations of negligible riskThe focus is diverted from structural causes and social responsibility to individual responsibility and the identification of groups of people to blame |
Source: in-house, adapted from World Health Organization. Advice on the use of masks in the context of COVID-19: interim guidance, 5 June 2020.9
Thirdly, compulsoriness can interfere with the necessary equity of public health actions, unless accompanied by complementary measures, such as government-subsidised distribution, free of charge to the end user, designed to ensure that low-income persons are able to acquire the most adequate masks in the right quantities for the goal being pursued. In addition, mandatory use of masks on a population scale should be accompanied by mass media campaigns that explain how to use the masks, what type is most suitable in each case, and the potential benefits and risks of their use by the general healthy population.
Fourthly, the obligation to use a mask may lead to those who do not wear one being socially stigmatised and, ultimately, discriminated against, even though they may have good reasons for this, whether because they take great care to maintain the required safety distance and only use masks when this is not possible, or because they come within one of the exceptions to the obligation to use a mask designated by the health authorities.
Lastly, this measure may generate confusion in the population, along with an altered perception of the risk, with the ensuing unfounded fear of becoming infected by virtue of simply meeting or passing by someone in the street who is not wearing a mask, and the mutual distrust among the public that can flow from this.
The WHO's and ECDC's (European Centre for Disease Prevention and Control) guidelines on the wearing of masks have remained largely consistent during the coronavirus pandemic and are two good examples of the prudence that is called for in these cases. While the former organisation only recommends the use of masks by healthy people in contexts of high risk of transmission when there is no capacity to implement other preventive or containment measures,9 the latter states that “the use of face masks in the community could be considered (only as a complementary measure), especially when visiting busy, closed spaces, such as grocery stores, shopping centres, or when using public transport, etc.”.27
ConclusionWith the degree of uncertainty currently surrounding the balance of potential benefits and harms of wearing masks in the general healthy population, especially in settings where there is a low risk of transmission (open, uncrowded spaces), it would seem more prudent to issue flexible recommendations than a set of compulsory measures aimed at restricting individual freedoms. While scientific evidence may support the advice to wear masks in certain circumstances, such as in public transport, closed crowded spaces or mass gatherings of any kind, where safe physical distancing cannot be continuously maintained and which should therefore be avoided if at all possible, any such recommendation should be combined with suitable information on how to use them and the potential risks of misuse. Mandatory use of masks in public spaces by the general healthy population, regardless of the potential risk of transmission or of whether or not the interpersonal safety distance can be kept, as has been implemented in Spain, is an intrusive measure that restricts individual freedoms, and would not appear to be justified on the basis of available scientific evidence regarding the potential benefits and risks associated with this practice. Moreover, the compulsoriness of wearing a mask should be accompanied by measures designed to ensure that the entire population, and the lower-income strata in particular, enjoys unrestricted access to these, while simultaneously preventing the possible risk of a shortage —present or future— of medical masks and respirators. What is needed, in contrast, are prudent measures, with soundly based recommendations, and effective communication campaigns to explain to the population where, when, how, and what type of mask it is advisable —or inadvisable— to wear. When the narrative changes because the scientific evidence changes, it is a sign that one is living in a mature society. But when the narrative changes without substantial changes in the scientific evidence which would justify this, and no other convincing reasons are given at the time for such a change of criterion, this means that something is not right.
Editor in chargeCarlos Álvarez-Dardet.
Authorship contributionsThe article was generated in Spain as result of discussions among the authors about the Government's decision to make the use of masks compulsory in open public spaces. M.A. Royo Bordonada wrote the first draft of the article. The remaining authors reviewed the draft, made relevant contributions to the text, and approved the final version.
FundingThis publication was supported by the Spanish Health Research Fund of the Institute of Health Carlos III (Project ENPY 120/18).
Conflicts of interestNone.









