




Chronic obstructive pulmonary disease (COPD) is a significant health problem in developed countries. We aimed to estimate the prevalence of COPD in a single Spanish healthcare area. We also aimed to assess if there are any differences in prevalence and spirometry use among primary care services by utilizing already registered information. We designed a cross-sectional study to determine the prevalence of COPD and the performance of spirometries in each primary care service. A total of 8,444 patients were diagnosed with COPD, with a prevalence of 2.6% for individuals older than 39 years. The prevalence increased with age and was much higher in men. Significant heterogeneity was found in the prevalence of COPD and spirometry use among primary care services. COPD was underdiagnosed and there was wide variability in spirometry use in our area. Greater efforts are needed to diagnose COPD in order to improve its clinical outcomes and to refine registries so that they can be used as reliable sources of information
La enfermedad pulmonar obstructiva crónica (EPOC) es un importante problema de salud en los países desarrollados. Se pretende estimar la prevalencia de la EPOC en un área sanitaria española para evaluar si existen diferencias en la prevalencia y en el uso de espirometrías entre los servicios de atención primaria utilizando información proveniente de registros. Se diseñó un estudio transversal para obtener la prevalencia de la EPOC y la realización de espirometrías en cada servicio de atención primaria. Hay 8444 pacientes diagnosticados de EPOC, con una prevalencia del 2,6% en mayores de 39 años. La prevalencia aumenta con la edad y es mucho más alta en los hombres que en las mujeres. Se observa una importante heterogeneidad en la prevalencia de la EPOC y en el uso de espirometrías entre servicios de primaria. La EPOC está infradiagnosticada y hay una fuerte variabilidad en el uso de espirometrías dentro de un área sanitaria. Deben hacerse más esfuerzos para diagnosticar la EPOC con el fin de mejorar los resultados clínicos, y refinar los registros para que puedan utilizarse como fuentes fiables de información sanitaria.
Chronic obstructive pulmonary disease (COPD) prevalence in Western countries is around 6-8%. In Spain, there is a prevalence of 10.2% in the population aged 40 to 80.1 Prevalence would be even higher if patients older than 80 were taken into consideration.
Healthcare organizations have enforced strategies for improving the control and follow-up of COPD patients. Information and communication technologies (ICTs) play an important role in its management. Using electronic health records a clinician can instantly have the patient¿s information and have access to his/her different tests. Furthermore, the disease prevalence can be calculated if the information is correctly registered.2
COPD prevalence information is scarce and there is a significant difference between registered prevalence and the true population prevalence. Many patients are not diagnosed because they do not have symptoms or clinicians are not aware of the value of spirometry. Spirometry is the core test for COPD, allowing the diagnosis of the disease and the assessment of its progression. At least one spirometry per year is recommended. Current guidelines recommend performing a spirometry on any smoker older than 40 who has smoked more than 10 pack-years.3 There is also a lack of information on how resources are used in primary care facilities to manage the disease. Some investigations have observed that a significant percentage of COPD patients have not had a spirometry performed in the last year and some COPD patients have even been diagnosed without this test.4
We aim to estimate COPD prevalence and the rate of spirometries performed in primary health care services using data exclusively obtained from health information systems.
Subjects and methodsThe study was performed in the Santiago de Compostela (A Coruña, Spain) health area. It has a population of 458,212 inhabitants, with 22.6% older than 64. Primary care is provided by 21 health services comprising 72 primary care facilities.
We designed a cross-sectional study to obtain COPD prevalence and the performance of spirometries during 2012 in the public health system. It covers approximately 97% of the entire Galician population. Data extraction was performed during June 2013. To retrieve COPD patients we used the code R95 of the International Classification of Primary Care-2. Health managers have access to all information systems, though it is necessary to have skills and training to retrieve specific information from the databases. We have also obtained COPD prevalence and performance of spirometries per each primary care service. We calculated non-parametric correlations (Spearman's rho) to assess the relationship between COPD prevalence and the number of spirometries per 100 COPD patients for each primary care service with SPSS v17.
ResultsIn Table 1 there is a sample description. 8,444 patients had COPD and prevalence was 1.8% (2.6% for those older than 39). COPD prevalence in individuals older than 74 was nearly twofold that of the 65-74 age group. COPD prevalence in males was double that of females. COPD prevalence for males 75 or older was 12.3% and 5.0% for females.
COPD prevalence broken down by age and gender in the Santiago de Compostela Health Area.
| Variable | n | % |
|---|---|---|
| Total populationFemales | 458,212236,630 | 10051.6 |
| COPD patients≤38 years39-64 years65-74 years≥75 years | 8,4441811,8292.0254.409 | 1.840.101.104.437.79 |
| Female COPD patients≤38 years39-64 years65-74 years≥75 years | 3,012775845931,758 | 1.270.080.72.445.01 |
| Male COPD patients≤38 years39-64 years65-74 years≥75 years | 5,4321041,2451,4322,651 | 2.450.111.506.6912.31 |
In 2012, a total of 7,071 spirometries were performed on COPD patients in the healthcare area. 14.9% of COPD patients had a spirometry registered in primary or specialized care. 71.2% of all spirometries were performed at a hospital and the remaining in family practices (n=1,986).
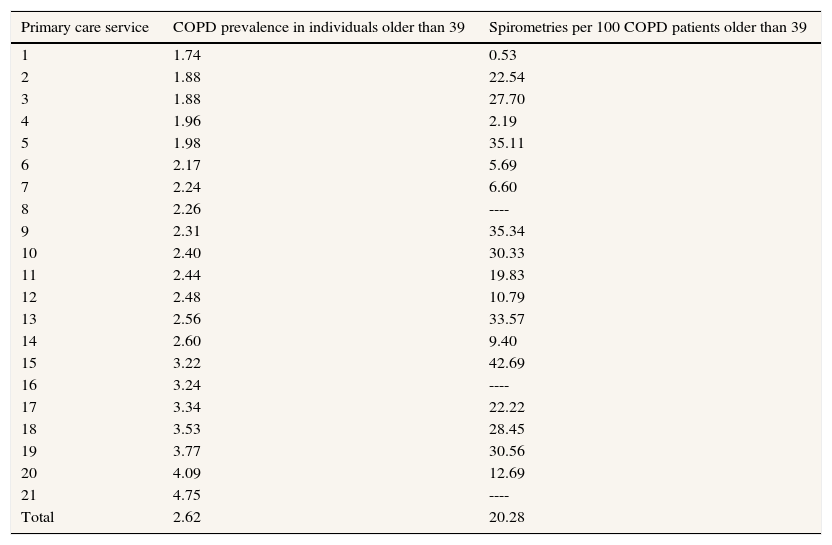
Table 2 shows the prevalence of COPD per each primary care service with the corresponding number of spirometries performed per 100 COPD patients. The primary service with the highest prevalence is three times that of the service with the lowest prevalence (1.74% vs. 4.75%), with a similar age distribution. There was no correlation between COPD prevalence and the number of spirometries performed in each primary care service (Spearman's ρ=0.31; p=0.21). Three primary care services did not perform any spirometries in 2012. 27% of COPD patients had at least one hospital admission during 2012.
COPD prevalence for primary care services and spirometries performed per 100 COPD patients during 2012.
| Primary care service | COPD prevalence in individuals older than 39 | Spirometries per 100 COPD patients older than 39 |
|---|---|---|
| 1 | 1.74 | 0.53 |
| 2 | 1.88 | 22.54 |
| 3 | 1.88 | 27.70 |
| 4 | 1.96 | 2.19 |
| 5 | 1.98 | 35.11 |
| 6 | 2.17 | 5.69 |
| 7 | 2.24 | 6.60 |
| 8 | 2.26 | ---- |
| 9 | 2.31 | 35.34 |
| 10 | 2.40 | 30.33 |
| 11 | 2.44 | 19.83 |
| 12 | 2.48 | 10.79 |
| 13 | 2.56 | 33.57 |
| 14 | 2.60 | 9.40 |
| 15 | 3.22 | 42.69 |
| 16 | 3.24 | ---- |
| 17 | 3.34 | 22.22 |
| 18 | 3.53 | 28.45 |
| 19 | 3.77 | 30.56 |
| 20 | 4.09 | 12.69 |
| 21 | 4.75 | ---- |
| Total | 2.62 | 20.28 |
To our knowledge, this is the first study performed in Spain using only registry-based information to calculate COPD prevalence. It is also the first to compare if there are differences in the prevalence and the ratio of spirometries performed per patient among primary care services. Using health information systems we have observed that COPD is clearly underdiagnosed in our area and also that spirometry is clearly underused in COPD patients. Furthermore, there is a great heterogeneity in its use among primary care facilities, but this heterogeneity does not depend on COPD prevalence. Low COPD prevalence in our area denotes underdiagnosis, in line with other studies. The EPI-SCAN study found 70% of unknown disease in the general population.1 Other studies have shown 3.5% COPD prevalence based on clinical registries5 while ours finds a 2.6% prevalence, which is lower than expected.
The exhaustiveness and reliability of disease registration in clinical databases is a critical aspect when using health information systems to obtain epidemiological information. If this information is appropriately registered it could provide important information for health managers and it would be unnecessary to carry out studies specifically directed to estimate the prevalence of many diseases. Clinicians should be aware of the importance of this registration and health administration should facilitate it.
We have found significant differences between primary care facilities. In some cases, despite the availability of spirometers, they are not used in family practices. It has not been until recently that spirometry results have been included in electronic health records. In the area of study all hospital-based spirometries are registered but this might not be the case for spirometries performed in family practices. If spirometries are performed during a medical visit, they can be registered or not, and therefore spirometries performed in primary care might be underestimated in the present study. It is quite common that COPD patients do not have spirometric values in their clinical history. The AUDIPOC study, a clinical audit including more than 5,000 COPD patients, followed up for three months to assess hospital readmissions and mortality, and observed that there were significant differences in the availability of spirometric data.6 Spirometry was registered only in 41%,7 59%8 and 30%9 of patients diagnosed with COPD in other investigations.
The main advantage of this study is that we have not used a sample but rather the entire population of the Santiago de Compostela health area, and therefore a possible selection bias should not be present. The main shortcoming is that this research is based on registered information and registration strongly depends on the physician¿s interest or responsibility. This is reflected by the high variability in COPD prevalence considering different primary care services.
COPD prevalence is underdiagnosed and the number of spirometries performed in primary care must be significantly increased in our area. It is very important to diagnose and treat occult COPD. The present study also demonstrates that health information systems can be used for multiple purposes, from knowing the prevalence of many diseases to having information regarding disease management. These registries might also be useful in the surveillance and monitoring of different health problems.10 The usefulness of this information resides in the physicians registration of medical data and health administration should allocate resources to strengthen registration.
Chronic obstructive pulmonary disease (COPD) is one of the most significant chronic diseases. Spirometry is the core test for COPD. Health information systems could be used to estimate the frequencies of many diseases and in the present paper we use them to estimate COPD prevalence and spirometry use within a healthcare area.
What does this study add to the literature?COPD is underdiagnosed and there are significant differences in spirometry use within one healthcare area. Integrated health information systems can be successfully used to compare the performance of primary care practices and to estimate the frequency of chronic diseases.
Pere Godoy.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authors’ contributionsA. Ruano-Ravina, L. Verde-Remeseiro and E. López-Pardo designed the research and interpreted the results. R. Castro-Calvo and F. Gude-Sampedro extracted the information and merged the databases. All authors wrote the paper and analyzed the results. All authors gave important insights to the work and approved the final version of the manuscript. A. Ruano-Ravina is the guarantor of the paper.
FundingThis research has been sponsored by an unrestricted grant by Almirall. The sponsor did not have any role in the design, writing or interpretation of the present research.
Conflicts of interestNone of the authors are employees of Almirall or have a financial relationship with this Company. One of the authors (A. Ruano-Ravina) belongs to the Gaceta Sanitaria editorial committee, but was not involved in the editorial process of the manuscript.











