




To estimate differences in the economic valuation and sociodemographic and clinical factors associated with informal care between phases of the treatment in the case of blood cancer patients.
Methods139 haematological cancer patients who underwent a stem cell transplantation completed a longitudinal questionnaire according to 3 phases of the treatment: short-term (pre-transplant), medium-term (1st year post-transplant) and long-term (2nd-6th year post-transplant). Economic value of informal care was estimated using proxy good and opportunity cost methods. Ordered and binary logistic models were performed to identify factors associated with informal care.
Results123 patients reported having received informal care. A progressive reduction of the number of hours of care was observed between phases. Monetary value per patient ranged from 1,288 to 3,409; 1,045 to 2,786; and 336 to 854 €/month in the short, medium and long term, respectively. Patients with acute leukaemia and those who received an unrelated allogeneic transplantation were 22% (short-term) and 33.5% (medium-term) more likely to receive more than 8hours/day of care respect to patients diagnosed with lymphoma and autologous transplantation. In the long term, patients with multiple myeloma were more likely to receive more care. Better health status and higher educational level were associated with fewer daily hours of care.
ConclusionsInformal care varies greatly between stages of the treatment depending on the clinical and sociodemographic factors. Significant caring time and societal costs are associated with such care in blood cancer patients.
Estimar los factores sociodemográficos y clínicos asociados al cuidado informal a lo largo de las diferentes etapas del tratamiento y su valoración económica en pacientes con neoplasia hematológica.
Métodos139 pacientes oncohematológicos que recibieron un trasplante de células madre respondieron un cuestionario longitudinal basado en tres fases del tratamiento: corto, medio y largo plazo. Los cuidados informales recibidos se valoraron económicamente mediante los métodos del bien más próximo y coste de oportunidad. Se estimaron modelos de regresión logística ordenada y binaria para identificar factores asociados al cuidado informal.
Resultados123 pacientes recibieron cuidado informal, con una reducción progresiva del número de horas a lo largo del tiempo. El valor monetario del cuidado informal recibido por paciente fue de 1288-3409 €, 1045-2786 € y 336-854 €/mes en el corto, medio y largo plazo, respectivamente. Los/las pacientes con leucemia aguda y los/las que recibieron un trasplante alogénico no emparentado tuvieron un 22% (corto plazo) y un 33,5% (medio plazo) más probabilidad de recibir >8 horas al día de cuidado respecto a los/las pacientes diagnosticados/as de linfoma y trasplante autólogo. A largo plazo, los/las pacientes con mieloma múltiple fueron más proclives a recibir más atención. Un mejor estado de salud y un mayor nivel de estudios se asociaron a menos horas diarias de cuidado.
ConclusionesExiste gran variación en el tiempo, el valor monetario y los factores asociados al cuidado informal en pacientes con neoplasia hematológica a lo largo de las distintas etapas del tratamiento.
Cancer is a disease that greatly changes the life of the patients throughout their treatment. Caregiver assistance in daily activities not only limited to personal care or household care, but also as psychological support, can be crucial for many patients.1–5 In this regard, the informal caregiver has played an essential role throughout history being recognized by the World Health Organization.6
The impact on health that informal caregivers of cancer patients are exposed to have been contrasted with those of other diseases,7–9 showing that the cancer caregivers are those who reported greater levels of physical burden and psychological distress5 and significant impairment across all health outcomes.10 Therefore, to study the time spent on informal care and its economic value is significant to identify the clinical and social magnitude of a disease, its family repercussion and stablish public policies.
Fortunately, the interest in including informal care in cost of illness studies has increased on the last years due to the significance of these results as part of the economic impact of the diseases. In this regard, recent studies have evaluated economically the informal care received by cancer patients8,11–13 in diagnoses such as prostate,14 lung,15 colorectal,15–17 or breast cancer.18 Nevertheless, the demand of informal care greatly varies depending not only on the diagnosis, but also depending on the sociodemographic and clinical characteristics of the patients and caregivers as well as on the phases of the treatment.5,12,14–19 Just four studies have evaluated economically the care giving across different phases of the cancer treatment,15–18 but none of them have valued it in a longitudinal and long-term way. Neither, any study has statistically examined the main determinants and differences that influence in the time spent on informal care in each phase of the treatment.
Our previous study identified the main factors related to the use or not of informal care in blood/haematological cancer patients between phases of the treatment,20 but no further information exists. We will go in depth of those results and our two objectives here are firstly, to quantify the informal care time given to blood cancer patients in the different phases of the treatments and its monetary value; and secondly, to estimate sociodemographic and clinical determinants associated with the time of informal care provided in each phase.
MethodDataWe have focused on blood cancer patients because the phases of the treatment can be differentiated easily; the main blood cancer diseases have been estimated an increase of the incidence rate in the European region;21 stem cell transplantation is increasing in a linear trend in Europe;22 and stem cell transplanted patients are among the most vulnerable and acute ill cancer populations.23
A longitudinal retrospective observational study was performed. For that purpose, a descriptive and longitudinal questionnaire was developed to obtain sociodemographic and clinical information relative to patients and their primary informal caregiver along different phases of the treatment. Eligible patients included adults (≥16 years) diagnosed with acute leukaemia, Hodgkin lymphoma, non-Hodgkin lymphoma, multiple myeloma and others less common malignant haematological diseases, who underwent a stem cell transplantation during the years 2006 to 2011 in the University Hospitals Virgen de las Nieves in Granada and Virgen del Rocio in Seville (Spain), and who at the time of the survey had survived the disease. Both hospitals are reference in malignant haematological diseases in southeast and southwest in Spain. The Clinical Research Ethics Committee and Haematology Department of each health centre approved the study.
299 patients were contacted by telephone and invited to participate. The questionnaire was sent by mail to 230 patients who answered the telephone and were able to participate.
To analyze the process of temporal evolution when receiving informal care, three sequential phases of the treatment were differentiated according to the medical protocol.24,25 Phase 1 or short-term corresponds to the pre-transplant phase, phase 2 or medium-term correspond to the first year after the transplant and phase 3 or long-term covers the second to the sixth year after the transplant. All the patients where in any of the years corresponding to phase 3 and answered prospectively the questions referring to phase 3 but retrospectively the questions referring to phase 1 and 2, based on the recall method (see Appendix 1 online).26
Informal care time and economic valuationThe number of months (duration) and the number of hours a day (intensity) of informal care received in each of the three phases was quantified. The intensity of informal care received at each period was measured by an ordinal categorical group variable (<2, 2-4, 4-8, >8hours/day). The midpoint of each ordinal group was used as the value of time.14 In the case of the group of more than 8hours/day, the midpoint was set at 12hours/day, following the truncation that other authors give restricting the maximum to 16hours/day care.12,16,17,27 Due to the retrospective nature of our study, we could not request for disaggregated information on basic and instrumental activities of daily life. This aggregated way of asking has been used previously to value caregiver burden.5
As there is no market price for informal care, it is necessary to allocate a shadow price for the valuation of these hours. The economic valuation of this time was carried out following revealed preferences methods, i.e., the proxy good method (PGM) and the opportunity cost method (OCM).26,28 The PGM values the time spent on informal care at the labour market price of a close market substitute. We valued care giving hours using the cost of reference of Home Help Service published in the Official Bulletin of the State of Spain because care services are offered by professional and trained caregivers.29 The cost was fixed at 14 €/hour for services related to personal care and at €9 per hour for attending to domestic needs and household-related services. Since we did not have any information concerning the time of care devoted to each of the services, we created three scenarios: 1) we supposed that full-time care was dedicated to personal attention; 2) we assumed that full-time care was dedicated to domestic and household needs; 3) we supposed that the time of care was dedicated equally to both personal attention as well as domestic needs assuming an average cost of 11.5 €/hour.
On the other hand, the OCM values informal care as the informal caregiver's benefit forgone due to spending time on providing informal care. Following Peña-Longobardo and Oliva-Moreno27 we considered that caregivers to be investing their time in working or doing their own housework and we created three groups according to the information provided. Group 1 was made up of those caregivers who had to leave the labour market or retired early. Due to the fact that information distinguishing between total or part-time work was not available in our survey, we quantified a maximum of 8 working hours/day over 5 days a week. Those hours were valued based on the mean gross salary per hour by gender in 2012 of the Wage Structure Survey published by the National Institute of Statistic of Spain in 2014 (€13.10/h for women and €15.83/h for men).30 Nonworking days and the additional hours of working days were rated by the gross wage per hour of a domestic worker in Spain in 2012 (€5.02/h, it is not a professional and trained care service for people in situation of dependence).31,32 Group 2 was made up of caregivers who were employed but who had to reduce their number of hours of working time. The working time lost was valued using the mean gross salary per hour by gender, as group 1. The rest of the hours of care of working days and the hours of nonworking days were also rated as group 1. Group 3 was made up of caregivers who were not in the labour market (housewives, retirees and unemployed) and employed caregivers who did not have to reduce their working hours, take early retirement and or abandon their job. The hours of informal care of working days and nonworking days were valued to €5.02/h, as group 1.31,32 Daily, monthly and total economic value of informal care were obtained by multiplying the number of hours by its cost according to the method used. All costs are given in Euros as of 2012.
Statistical analysisA descriptive analysis of the characteristics of patients and their informal caregivers was performed. We differentiated between static variables (those that remain constant over time): age, sex, marital status, educational level, diagnosis, type of transplantation, relation to cancer patient, early retirement or abandonment of the job; and dynamic variables (those that vary over time): health status, recruitment of a formal caregiver, employment situation of the patient, reduction of the working hours of the caregiver and the number of months and hours of informal care received.
According to the second objective, three logistic regression models were calculated, given the character of the dependent variables and the interpretative power of the models.33 Specifically, two ordered logistic regression models were estimated in phase 1 and 2 due to the ordinal nature of the dependent variable (number of hours of informal care received: <2, 2-4, 4-8, >8hours/day) and a binary logistic regression was applied in phase 3 due to the reduced variability of the dependent variable (<2, >2hours/day). A description of the dependent and independent variables in the statistical models can be found in the Appendix 2 online. Marginal effects were estimated on those independent sociodemographic and clinical variables whose parameters were statistically significant. The statistical program Stata 12.0 was used.
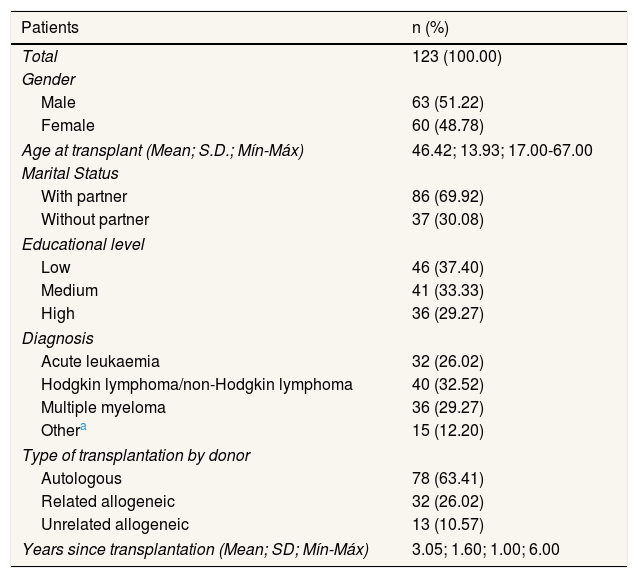
ResultsA total of 139 questionnaires were received (60.43% response rate) of which 123 patients reported having received informal care at some phase in the treatment (88.49% of survey respondents). 51.22% (n=63) of the patients were male and the average age was 46. Descriptive static and dynamic variables of patients and informal caregivers are shown in Tables 1 and 2.
Characteristics of patients and their informal caregivers.
| Patients | n (%) |
|---|---|
| Total | 123 (100.00) |
| Gender | |
| Male | 63 (51.22) |
| Female | 60 (48.78) |
| Age at transplant (Mean; S.D.; Mín-Máx) | 46.42; 13.93; 17.00-67.00 |
| Marital Status | |
| With partner | 86 (69.92) |
| Without partner | 37 (30.08) |
| Educational level | |
| Low | 46 (37.40) |
| Medium | 41 (33.33) |
| High | 36 (29.27) |
| Diagnosis | |
| Acute leukaemia | 32 (26.02) |
| Hodgkin lymphoma/non-Hodgkin lymphoma | 40 (32.52) |
| Multiple myeloma | 36 (29.27) |
| Othera | 15 (12.20) |
| Type of transplantation by donor | |
| Autologous | 78 (63.41) |
| Related allogeneic | 32 (26.02) |
| Unrelated allogeneic | 13 (10.57) |
| Years since transplantation (Mean; SD; Mín-Máx) | 3.05; 1.60; 1.00; 6.00 |
| Primary informal caregiversb | n (%) |
|---|---|
| Total | 123 (100.00) |
| Gender | |
| Male | 32 (26.02) |
| Female | 91 (73.98) |
| Employment status before the diagnosis | |
| Employed | 59 (47.97) |
| Unemployed | 13 (10.57) |
| Retired | 15 (12.20) |
| Housewife | 34 (27.64) |
| Other | 2 (1.63) |
| Relation to cancer patient | |
| Partner | 70 (56.91) |
| Not partnerc | 53 (43.09) |
| Early retirement/leave the job to provide care | |
| Yes | 14 (11.38) |
| No | 108 (87.80) |
| Missing data | 1 (0.82) |
SD: standard deviation.
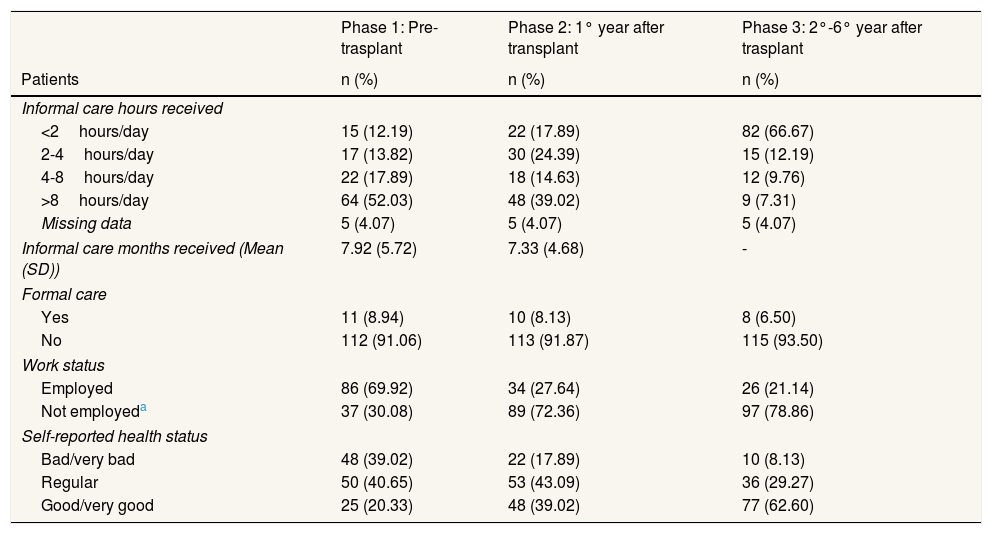
Characteristics of patients and their informal caregivers. Dynamic variables.
| Phase 1: Pre-trasplant | Phase 2: 1° year after transplant | Phase 3: 2°-6° year after trasplant | |
|---|---|---|---|
| Patients | n (%) | n (%) | n (%) |
| Informal care hours received | |||
| <2hours/day | 15 (12.19) | 22 (17.89) | 82 (66.67) |
| 2-4hours/day | 17 (13.82) | 30 (24.39) | 15 (12.19) |
| 4-8hours/day | 22 (17.89) | 18 (14.63) | 12 (9.76) |
| >8hours/day | 64 (52.03) | 48 (39.02) | 9 (7.31) |
| Missing data | 5 (4.07) | 5 (4.07) | 5 (4.07) |
| Informal care months received (Mean (SD)) | 7.92 (5.72) | 7.33 (4.68) | - |
| Formal care | |||
| Yes | 11 (8.94) | 10 (8.13) | 8 (6.50) |
| No | 112 (91.06) | 113 (91.87) | 115 (93.50) |
| Work status | |||
| Employed | 86 (69.92) | 34 (27.64) | 26 (21.14) |
| Not employeda | 37 (30.08) | 89 (72.36) | 97 (78.86) |
| Self-reported health status | |||
| Bad/very bad | 48 (39.02) | 22 (17.89) | 10 (8.13) |
| Regular | 50 (40.65) | 53 (43.09) | 36 (29.27) |
| Good/very good | 25 (20.33) | 48 (39.02) | 77 (62.60) |
| Primary informal caregiver | n | Mean (SD) | Min-Max | n | Mean (SD) | Min-Max | n | Mean (SD) | Min-Max |
|---|---|---|---|---|---|---|---|---|---|
| Reduction working days | 31 | 73.87 (90.03) | 0-365 | 34 | 39.00 (79.32) | 0-365 | 35 | 0.89 (3.24) | 0-15 |
| Reduction working hours | 36 | 123.75 (383.98) | 0-1500 | 35 | 199.32 (488.45) | 0-1825 | 36 | 0.16 (0.69) | 0-3 |
SD: standard deviation.
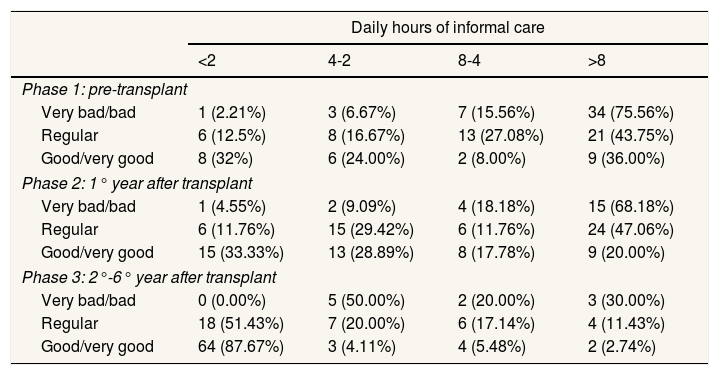
The average number of estimated months of care was around 8 during the short-term and 7 during the medium-term. More than 50% (n=64) of the patients reported receiving more than 8hours/day of informal care in the pre-transplant phase (Table 2). This may be due to the aggressiveness of the chemotherapy treatment to which the patient is subjected diminishing their health status. During the first year after the transplant, the daily hours of informal care are more than 8 in 39.02% (n=48) of cases and between 2-4hours/day in 24.39% of cases (n=30). This variation may be due to possible complications after the transplant in some patients. However, in phase 3, 66.67% (n=82) of patients reported having received less than 2hours of care per day. The progressive reduction in time of informal care is related to health status in each phase of the treatment as we will see in the logistics model, but also Table 3 reflects that patients who had a bad or very bad state of health reported receiving more than 8hours of care a day in the short and medium term. However, in the long-term, patients with very bad or bad health status received between 2-4hours of care a day. This can be justified by the physical and psychological exhaustion of the informal caregivers themselves over time given the intensity in care during the previous phases.9,34
Daily hours of informal care distribution by self-reported health status (number and percentage of patients).
| Daily hours of informal care | ||||
|---|---|---|---|---|
| <2 | 4-2 | 8-4 | >8 | |
| Phase 1: pre-transplant | ||||
| Very bad/bad | 1 (2.21%) | 3 (6.67%) | 7 (15.56%) | 34 (75.56%) |
| Regular | 6 (12.5%) | 8 (16.67%) | 13 (27.08%) | 21 (43.75%) |
| Good/very good | 8 (32%) | 6 (24.00%) | 2 (8.00%) | 9 (36.00%) |
| Phase 2: 1° year after transplant | ||||
| Very bad/bad | 1 (4.55%) | 2 (9.09%) | 4 (18.18%) | 15 (68.18%) |
| Regular | 6 (11.76%) | 15 (29.42%) | 6 (11.76%) | 24 (47.06%) |
| Good/very good | 15 (33.33%) | 13 (28.89%) | 8 (17.78%) | 9 (20.00%) |
| Phase 3: 2°-6° year after transplant | ||||
| Very bad/bad | 0 (0.00%) | 5 (50.00%) | 2 (20.00%) | 3 (30.00%) |
| Regular | 18 (51.43%) | 7 (20.00%) | 6 (17.14%) | 4 (11.43%) |
| Good/very good | 64 (87.67%) | 3 (4.11%) | 4 (5.48%) | 2 (2.74%) |
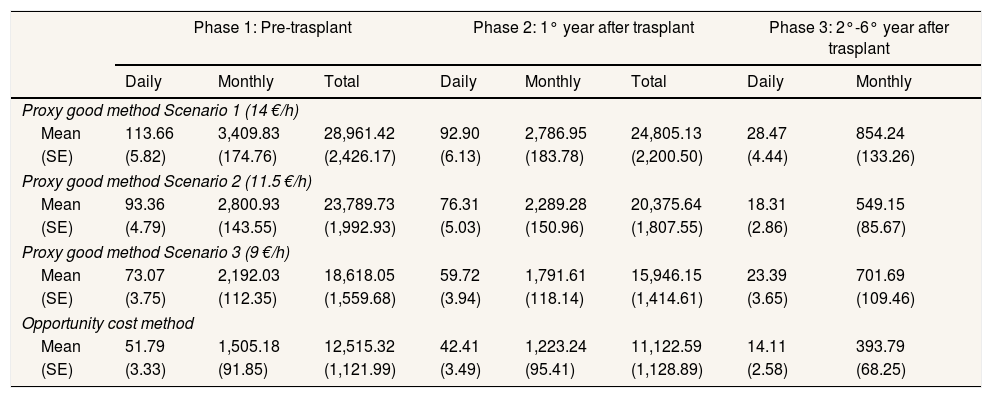
The average monetary valuation of the hours of informal care received during the pre-transplantation phase translates into a value of €3,409, €2,800 and €2,192 per month using the PGM, in cases where the hours of care received are made up entirely of personal care, domestic care and at home, or a mix of both respectively. This value is rounded up to €1,505/month using the OCM (Table 4). This monetary value drops significantly in the second and third phase as a consequence of the reduction in the number of hours of care, ranged from €854/month to €701/month using the PGM to 393 €/month by using the OCM in the third phase (Table 4).
Economic value of informal care per haematologic cancer patient and phase of the treatment.a
| Phase 1: Pre-trasplant | Phase 2: 1° year after trasplant | Phase 3: 2°-6° year after trasplant | ||||||
|---|---|---|---|---|---|---|---|---|
| Daily | Monthly | Total | Daily | Monthly | Total | Daily | Monthly | |
| Proxy good method Scenario 1 (14 €/h) | ||||||||
| Mean | 113.66 | 3,409.83 | 28,961.42 | 92.90 | 2,786.95 | 24,805.13 | 28.47 | 854.24 |
| (SE) | (5.82) | (174.76) | (2,426.17) | (6.13) | (183.78) | (2,200.50) | (4.44) | (133.26) |
| Proxy good method Scenario 2 (11.5 €/h) | ||||||||
| Mean | 93.36 | 2,800.93 | 23,789.73 | 76.31 | 2,289.28 | 20,375.64 | 18.31 | 549.15 |
| (SE) | (4.79) | (143.55) | (1,992.93) | (5.03) | (150.96) | (1,807.55) | (2.86) | (85.67) |
| Proxy good method Scenario 3 (9 €/h) | ||||||||
| Mean | 73.07 | 2,192.03 | 18,618.05 | 59.72 | 1,791.61 | 15,946.15 | 23.39 | 701.69 |
| (SE) | (3.75) | (112.35) | (1,559.68) | (3.94) | (118.14) | (1,414.61) | (3.65) | (109.46) |
| Opportunity cost method | ||||||||
| Mean | 51.79 | 1,505.18 | 12,515.32 | 42.41 | 1,223.24 | 11,122.59 | 14.11 | 393.79 |
| (SE) | (3.33) | (91.85) | (1,121.99) | (3.49) | (95.41) | (1,128.89) | (2.58) | (68.25) |
SE: standard error.
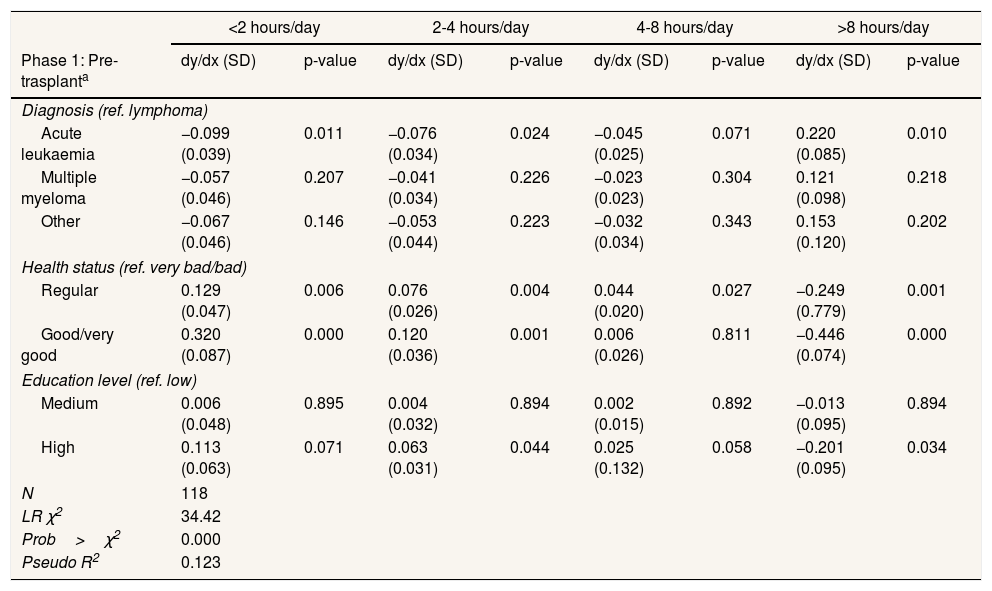
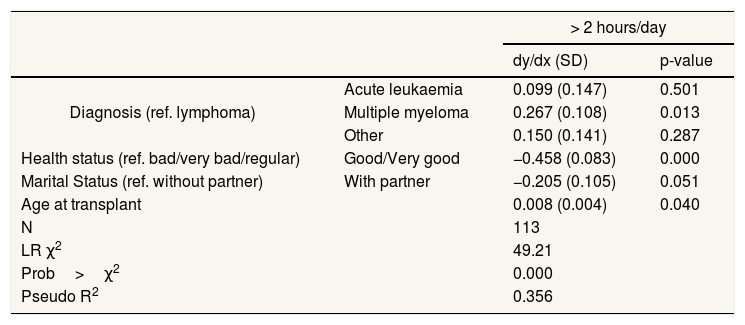
Table 5 shows the determinants associated with the number of hours of informal care received by the patients during phase 1 and 2. Variables whose estimated parameters were statistically significant were the type of diagnosis, the health status and the level of education of the patient (results of models in Appendix 3 online). The likelihood of receiving more than eight hours of informal care during the pre-transplant phase is 22% higher in patients diagnosed with acute leukaemia than in patients diagnosed with lymphoma. This is due to their chemotherapy treatment which is much more aggressive than the rest of diagnoses in this phase.1,35 No significant differences between the lymphoma and the rest of diagnoses are shown. On the contrary, during the first year, the diagnosis is not a relevant determinant, its effect being absorbed by the type of transplant, which takes centre stage in this phase. Patients who have undergone an unrelated allogeneic transplant were 33.5% more likely to receive more than 8hours of care, compared to patients who have received an autologous transplantation. This is due to the complications associated with this type of transplant, such as infections, respiratory and cardiovascular diseases or graft-versus-host disease. In the long-term (Table 6) the patients with multiple myeloma are the ones who are 26.7% more likely to receive more than 2hours compared with patients diagnosed with lymphoma. The justification is that, while their current treatment has substantially improved in recent years, the probability of relapsing into the disease 3-4 years after the transplant is 90%,35 so the long-term care need is greater. On the contrary, the majority of patients who survive acute leukaemia will get back to a satisfactory level of physical, emotional well-being and daily activity.1
Determinants associated with the number of hours of informal care during phase 1 and phase 2.
| <2 hours/day | 2-4 hours/day | 4-8 hours/day | >8 hours/day | |||||
|---|---|---|---|---|---|---|---|---|
| Phase 1: Pre-trasplanta | dy/dx (SD) | p-value | dy/dx (SD) | p-value | dy/dx (SD) | p-value | dy/dx (SD) | p-value |
| Diagnosis (ref. lymphoma) | ||||||||
| Acute leukaemia | −0.099 (0.039) | 0.011 | −0.076 (0.034) | 0.024 | −0.045 (0.025) | 0.071 | 0.220 (0.085) | 0.010 |
| Multiple myeloma | −0.057 (0.046) | 0.207 | −0.041 (0.034) | 0.226 | −0.023 (0.023) | 0.304 | 0.121 (0.098) | 0.218 |
| Other | −0.067 (0.046) | 0.146 | −0.053 (0.044) | 0.223 | −0.032 (0.034) | 0.343 | 0.153 (0.120) | 0.202 |
| Health status (ref. very bad/bad) | ||||||||
| Regular | 0.129 (0.047) | 0.006 | 0.076 (0.026) | 0.004 | 0.044 (0.020) | 0.027 | −0.249 (0.779) | 0.001 |
| Good/very good | 0.320 (0.087) | 0.000 | 0.120 (0.036) | 0.001 | 0.006 (0.026) | 0.811 | −0.446 (0.074) | 0.000 |
| Education level (ref. low) | ||||||||
| Medium | 0.006 (0.048) | 0.895 | 0.004 (0.032) | 0.894 | 0.002 (0.015) | 0.892 | −0.013 (0.095) | 0.894 |
| High | 0.113 (0.063) | 0.071 | 0.063 (0.031) | 0.044 | 0.025 (0.132) | 0.058 | −0.201 (0.095) | 0.034 |
| N | 118 | |||||||
| LR χ2 | 34.42 | |||||||
| Prob>χ2 | 0.000 | |||||||
| Pseudo R2 | 0.123 | |||||||
| Phase 2: 1° year after trasplantb | dy/dx (SD) | p-value | dy/dx (SD) | p-value | dy/dx (SD) | p-value | dy/dx (SD) | p-value |
|---|---|---|---|---|---|---|---|---|
| Transplantation (ref. autologous) | ||||||||
| Related allogeneic | 0.008 (0.069) | 0.910 | 0.004 (0.036) | 0.908 | 0.000 (0.004) | 0.917 | 0.012 (0.101) | 0.909 |
| Unrelated allogeneic | −0.149 (0.048) | 0.002 | −0.145 (0.069) | 0.034 | −0.040 (0.039) | 0.304 | 0.335 (0.143) | 0.019 |
| Health status (ref. very bad/bad) | ||||||||
| Regular | 0.079 (0.071) | 0.271 | 0.037 (0.027) | 0.180 | −0.002 (0.005) | 0.637 | −0.113 (0.096) | 0.238 |
| Good/very good | 0.259 (0.084) | 0.002 | 0.119 (0.036) | 0.001 | −0.021 (0.019) | 0.272 | −0.358 (0.091) | 0.000 |
| Education level (ref. low) | ||||||||
| Medium | 0.104 (0.063) | 0.103 | 0.045 (0.024) | 0.057 | −0.005 (0.008) | 0.483 | −0.143 (0.080) | 0.072 |
| High | 0.243 (0.081) | 0.003 | 0.081 (0.029) | 0.006 | −0.033 (0.021) | 0.111 | −0.291 (0.075) | 0.000 |
| N | 118 | |||||||
| LR χ2 | 39.97 | |||||||
| Prob>χ2 | 0.000 | |||||||
| Pseudo R2 | 0.129 | |||||||
SD: standard deviation.
Dependent variable: Number of hours of informal care per day. Independent variablesa: age at transplant, gender and marital status of the patient, and caregiver's gender and employment status. Independent variablesb: diagnosis, age at transplant, gender and marital status of the patient, and caregiver's gender and employment status.
Determinants associated with the number of hours of informal care during phase 3.
| > 2 hours/day | |||
|---|---|---|---|
| dy/dx (SD) | p-value | ||
| Diagnosis (ref. lymphoma) | Acute leukaemia | 0.099 (0.147) | 0.501 |
| Multiple myeloma | 0.267 (0.108) | 0.013 | |
| Other | 0.150 (0.141) | 0.287 | |
| Health status (ref. bad/very bad/regular) | Good/Very good | −0.458 (0.083) | 0.000 |
| Marital Status (ref. without partner) | With partner | −0.205 (0.105) | 0.051 |
| Age at transplant | 0.008 (0.004) | 0.040 | |
| N | 113 | ||
| LR χ2 | 49.21 | ||
| Prob>χ2 | 0.000 | ||
| Pseudo R2 | 0.356 | ||
SD: standard deviation.
Dependent variable: To receive more than 2hours of informal care per day. Independent variables: type of transplantation, education level and gender of the patient, and caregiver's gender and employment status.
Regarding the state of health, those patients who show a good or very good health status in the phase 1 and 2 are 32% and 25.9% more likely to receive less than 2hours of informal care in these phases compared with those patients who have a bad or very bad health status (Table 5). Data shows that there is a decreasing trend in the probability of receiving more number of hours of care for these patients. At long term, patients who show a better health status are 45.8% less likely to receive more than 2hours than those who show worse health status (Table 6).
Finally, a third relevant variable is the educational level (Table 5). In regards to this, those patients with high educational level are 11.3% more likely to receive less than 2hours of daily care during the pre-transplant than those that have a low educational level, and a minor probability of 20.1% of receiving more than 8hours/day. In the first year after the transplantation the significance of influence is maintained, however, from the first year onwards, the educational level is not statistically significant, while other determinants such as marital status and age were, as explained in a previous study.20
DiscussionWe found that primary informal care varies greatly between stages of the treatment. In our study, blood cancer patients receive more than 8hours per day during the pre-transplant period (52.03% of the patients), but there is a progressive reduction of the number of hours received between phases, being lowest in the long-term. Therefore, the economic value associated with such care varies seriously between phases. These results were expected as the first and second periods involve aggressive treatments, complications, days of hospitalization and worse health status. The figure of formal caregiver is referred to as a complement in less than 10% of patients given that both caregivers were caring at the same time, hence we follow the line of other works and highlight the relevance of the informal caregiver in cancer patients.3,10,15–17,20,34
Several limitations of this study should also be noted. Firstly, the analysis was performed in patients diagnosed with haematologic neoplasm who had undergone stem cell transplantation as a minimum in the previous year. This selection was done with the aim of analysing the informal care received not only at the phase of chemotherapy but in the transplantation phases characterized by health complications. Secondly, the recall method used in the questionnaire is not as reliable as a diary-based method given that the patients had to remember the amount of care received. Therefore, there could be a bias based on the memory. However, it is the best method given our study design.26 In order to reduce the possible bias, intervals in the hours of care questions were established. A third limitation refers to the response bias which reduces the sample. Further studies with larger samples and different types of cancer are expected in order to expand and compare the results described.
This is the first study which analyses the longitudinal and dynamic way the informal care provided in the long-term to cancer patients, specifically on blood cancer patients. Few studies have explored the impact of informal care to cancer patients applying two alternative valuation approaches to value the time cost, hence our results could be used in economic evaluations on health technology assessment on haematological cancer (data hitherto unknown). Furthermore, these results can be relevant worldwide for the design of private insurances of cancer and the design of programs by public decision-makers to establish economic forecasts in the case of a non-availability of informal caregivers.
Informal care varies greatly between phases of the treatment, mostly in cancer patients. However, few information exits according to the progress of the informal care over the time, none regarding cancer and specifically blood cancer, maybe because of the difficulty to get primary information.
What does this study add to the literature?Significant caring time and economic value are associated with informal care in blood cancer patients mainly during the first and second phase of the treatment. Sociodemographic and clinical factors are associated with each phase of the treatment. These results will be very useful for the design of private insurances of cancer and future policies by public decision-makers.
Miguel Ángel Negrín Hernández.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsM. Ortega-Ortega was the principal researcher, took primary responsibility for the paper and collected the data. R. Montero-Granados, J.D. Jiménez-Aguilera and M. Ortega-Ortega analyzed, interpreted and discussed the results. M. Ortega-Ortega wrote the first draft of the manuscript and the rest of the authors helped in the successive reviews up to the final version. All the authors have approved the final version.
FundingNone.
Conflicts of interestNone.
This work has been done thanks to a doctoral scholarship funded by the European Regional Development Fund and the Ministry of Innovation, Science and Enterprise of the Andalusian regional government (Spain). The authors would like to thank the collaboration of the Haematological Department of the University Hospital Virgen de las Nieves (Granada, Spain) and University Hospital Virgen del Rocío (Seville, Spain), specially Antonio Romero-Aguilar, MD, and Ildefonso Espigado-Tocino, MD, for their support and the critical and medical role they played in this work. We are also grateful to Raúl del Pozo Rubio, PhD, for his support and constructive comments. The authors also would like to thank the participation of all the patients that voluntarily answered the questionnaire and have made this study possible. Also, to all of them who were too ill to response it. They inspired this research.
This work has received the award for best poster at the Spanish Annual XXXV Conference on Health Economics.














