






There is evidence on the efficiency of new direct oral anticoagulants (DOAC), mostly based on experimental efficacy data, but there is also a need to assess their cost-effectiveness in routine clinical practice using patient-level data. We designed a retrospective cohort study to assess the cost-effectiveness of DOAC compared to acenocoumarol in patients with non-valvular atrial fibrillation (NVAF) with a follow-up of up to 7 years.
MethodBasque Health Service-registered patients who started oral anticoagulant treatment between 2013 and 2016 were included in the study and followed up until the end of 2019. Data were extracted from an electronic medical record management system. Effectiveness was expressed in terms of life years gained and adjusted for health-related quality of life (i.e., quality-adjusted life years [QALY]). Propensity score techniques were used to adjust the estimates for differences between groups in baseline characteristics.
ResultsA total of 10,843 new users of oral anticoagulants with a mean follow-up of 4.1 years were included. The incremental cost-effectiveness ratio of DOAC compared to acenocoumarol ranged from €1,732 to €2,556/QALY, while the incremental net benefit for different willingness-to-pay thresholds was only negative for values below €3,000/QALY.
ConclusionsBased on the analysis of data from clinical practice and the similarity of results using several different techniques to adjust for bias associated with observational studies, we conclude that DOAC would be an efficient alternative for the treatment of patients with NVAF.
Existe evidencia de la eficacia de los nuevos anticoagulantes orales directos (ACOD), basadas sobre todo en datos experimentales, pero también es necesario evaluar su coste-efectividad en la práctica clínica habitual utilizando datos del paciente. Se diseñó un estudio de cohortes retrospectivas con el objetivo de evaluar el coste-efectividad de los ACOD en comparación con acenocumarol en pacientes con fibrilación auricular no valvular (FANV), con hasta 7 años de seguimiento.
MétodoSe incluyeron pacientes del Sistema Vasco de Salud (Osakidetza) que comenzaron un tratamiento anticoagulante entre 2013 y 2016, siendo seguidos hasta finales de 2019. Los datos se extrajeron de las historias clínicas electrónicas. La efectividad se expresa como años de vida ganados y años de vida ajustados por calidad (AVAC). Se emplearon distintas técnicas de ajuste propensity score para limitar el impacto de las covariables sobre los resultados.
ResultadosSe incluyeron 10.843 nuevos usuarios de fármacos anticoagulantes, con un seguimiento medio de 4,1 años. La ratio coste-efectividad incremental de los ACOD comparados con acenocumarol varió entre 1.732 € y 2.556 € por AVAC, mientras que el beneficio neto incremental para distintas disponibilidades a pagar solo resultó negativa para valores inferiores a 3.000 € por AVAC.
ConclusionesTeniendo en cuenta que se parte de datos provenientes de la práctica clínica habitual y la obtención de resultados consistentes empleando distintas técnicas de ajuste propias de los estudios observacionales, se concluye que los ACOD pueden ser una alternativa eficiente en el tratamiento de los pacientes con FANV.
Non-valvular atrial fibrillation (NVAF) is the most common type of chronic heart arrhythmia in adults and it has been estimated that this condition alone increases the risk of stroke and systemic embolism 4- to 5-fold.1–3 Anticoagulant treatment reduces the risk of ischemic stroke in patients with NVAF by 66%, regardless of the patient's baseline risk.4 Initiation of oral anticoagulant therapy is recommended in patients with scores ≥2 on the CHA2DS2-VASc scale.5,6 For a long time, the only treatments proven effective for the prevention of stroke in NVAF were based on vitamin K antagonists, particularly warfarin and acenocoumarol (ACN).7 Although these drugs are effective, they have a narrow therapeutic window that requires close monitoring of prothrombin time, and numerous interactions with both diet and a wide range of drugs. Seeking to overcome these limitations, several new direct oral anticoagulants (DOAC), including dabigatran, rivaroxaban and apixaban, have been approved since 2010.
Several economic assessments of the efficacy of the new DOAC have been published8–10. While the results vary considerably, in most studies, the incremental cost-effectiveness ratio (ICER) has been estimated at around €25,000-30,000/quality-adjusted life year (QALY), close to the threshold of what would be considered an efficient alternative in our health setting. A meta-analysis of 100 economic evaluation studies comparing DOAC and vitamin K antagonists indicated that all DOAC were cost-effective compared to vitamin K antagonists.11 Economic evaluations conducted in Spain have drawn similar conclusions, although with great heterogeneity in the methods used.8,12,13 As they reflect outcomes in clinical practice as opposed to clinical trials, the use of administrative and clinical data collected in routine practice (real-world data [RWD]) to assess the comparative effectiveness and cost-effectiveness of DOAC has increased in recent decades.9 However, they have not been used to evaluate the cost-effectiveness of DOAC in Spain.
The objective of this study was to assess the comparative efficacy of DOAC and ACN in NVAF through cost-effectiveness analysis adapted to the particular characteristics of real clinical practice within the Basque Health System.
MethodThe study was approved by the Ethics Committee of the Euskadi (reference number: EPA2017040) and funded by a grant from the Department of Health of the Government of the Basque Country awarded in 2016.
Design and data sourcesWe conducted a retrospective observational parallel-group study of incident naïve users of an oral anticoagulant (“new-user design”), selecting this design to reduce the bias associated with the use of secondary data sources such as health databases.14–17 See also, Supplementary Material: Appendix 1, 2 and 3.
In the Basque Health Service (Osakidetza), the electronic health record is well established and linked to patient administrative data related to patients’ contacts with the health system during their process of care at various levels: primary, outpatient specialist, emergency department, and inpatient care, as well as home care/hospital at home. These records are stored in the organisation-wide database of the Basque Health Service (Oracle Analytics Server, OAS) and allow us to determine the healthcare resource use of a target population, in our case, people diagnosed with NVAF.
Inclusion and exclusion criteriaThe study was carried out in adult patients (≥18 years old) who had previously been diagnosed with NVAF (diagnosis codes: 427.31 or 427.32 in the International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] or I48 in the ICD-10-CM, recorded in the OAS), with an initial prescription (treatment-naïve) of an oral anticoagulant treatment (ACN or DOAC) between 2013 and 2016, with follow-up until the end of the study on 31 December 2019, or until death due to any cause (longest individual follow-up of 7 years). The exclusion criteria were history of anticoagulant use (before the index date), diagnosis of mitral valve stenosis or history of heart valve replacement, need for chronic haemodialysis or peritoneal dialysis, history of kidney or liver transplantation, or history of severe bleeding. Due to the number of new users differing markedly between the ACN and DOAC cohorts, we took a random sample of 7,237 ACN-treated patients and included all 3,606 patients treated with DOAC (650 with dabigatran, 1,701 with rivaroxaban and 1,255 with apixaban).
VariablesFrom the information in the OAS, we obtained the following anonymised data: sex, date of birth, date of death, and age at death and age at index date (both calculated). Based on the diagnoses recorded in the electronic health record, for each patient, we identified the presence of coagulation disorders, ischaemic stroke, hypertension, hyperlipidaemia, and any of the 17 conditions included in the Charlson Comorbidity index18,19 and calculated the CHA2DS2-VASc6 and hypertension, abnormal renal and/or liver function, stroke, bleeding tendency or predisposition, labile International Normalized Ratio (INR), and elderly (HAS-BLED)20 scores, using the ICD-9-CM and ICD-10-CM (see Supplementary Material: Appendix 1, 2 and 3). The Charlson Comorbidity index quantifies the risk of mortality associated with 17 weighted chronic conditions. We also obtained the Anatomical Therapeutic Chemical (ATC) classification system codes of patients’ prescriptions to identify the use of antiplatelets, acetylsalicylic acid, nonsteroidal anti-inflammatory drugs, statins, antidiabetic agents, antiarrhythmic agents, and heparin.
Outcomes measuresThe primary effectiveness outcome for this study was the combined incidence of stroke and systemic embolism events; the secondary effectiveness outcomes were diagnosis of stroke, transient ischaemic attack), systemic embolism, acute myocardial infarction, and other types of embolism, and all-cause mortality (see Supplementary Material: Appendix 2 for ICD codes). The primary safety outcome was the onset of severe bleeding; and the secondary safety outcomes were intracranial haemorrhage, gastrointestinal haemorrhage, and any other severe bleeding events. Data on thromboembolic and bleeding events during the follow-up period were retrieved from the OAS.
Economic evaluationWe carried out an economic evaluation of the efficiency of DOAC versus ACN based on individual real-world data at the patient level from the perspective of the Health System (see Supplementary Material: Appendix 4 for more methods). We used life years and QALY as a measure of effectiveness. Life years were calculated as the time elapsed from index date to death or censorship, if patients were alive at the end of follow-up (31 December 2019).
For comparing the treatment options under study, we used the ICER, which is calculated as the cost of the alternative treatment relative to the comparator (incremental cost) divided by the difference in their effect (incremental effectiveness). The analysis was based on the calculation of the ICER and the incremental net benefit (INB)21,22 using the following equations:
ICER=ΔC/ΔE=(Ca−Cc)/(Ea−Ec)
INB=λ * ΔE−ΔC
where C reflects the cost of each treatment option, E the effect of each option on outcomes, and λ the willingness to pay (WTP) for an additional unit of health benefit. The WTP threshold has been set at €20,000/QALY,23 and as a sensitivity analysis, we also calculated the INB for different WTP values.24 We adopted a public health system perspective, and the analyses were carried out on an intention-to-treat basis.
Given that the analysis was based on individual follow-up data, we calculated individual ICER values, and as a measure of uncertainty, the 95% confidence intervals (95%CI) using the percentile bootstrap method25.
Measures of utilityThe baseline utility for each patient by age and sex was estimated using normative values published for Spain26 which are similar to the values for NVAF patients living in the Basque Country.27 For each of the events of interest, disutility values are then subtracted from the baseline utility, and for this, we took disutility values that have already been used in other pharmacoeconomic studies28 (stroke,−0.139; systemic embolism,−0.105; acute myocardial infarction,−0.125; intracranial haemorrhage,−0.181; and gastrointestinal haemorrhage,−0.050). Disutilities associated with baseline comorbidities were not included because they were variables prior to anticoagulation and accounted for in the propensity score. The QALY were calculated by multiplying the time between events by the utility during this period, using the trapezoidal rule.24
Measures of resource use and costsThe base year of unit cost was 2019. The following data were collected throughout patient follow-up: primary care consultations, outpatient specialist consultations, hospital emergency department attendance, hospital admissions associated with cardiovascular events, and the use of drugs from ATC classes B01A (antithrombotic agents) or B01AA, B01AF, or B01AE (oral anticoagulants).
We did not take into account activities such as the use of the laboratory, ambulance services, or other types of healthcare-related resources, patient-related costs (travel or other expenses), or administrative costs. In addition, the cost of INR monitoring has been included in the case of patients on ACN. The unit costs of resources have been obtained from the cost accounting system of the Basque Health Service. Unit costs can be reviewed in Table S1 in Supplementary Material, Appendix 5.
Statistical analysisUnivariate analysis was performed to detect any clinical variables that differed between the intervention groups and might bias the results. Continuous variables were evaluated using Student's t tests, or if data were not normally distributed, non-parametric Mann-Whitney tests. Categorical variables were analysed using Chi-squared or Fisher's exact tests, as appropriate. Differences in the distribution of the variables were considered significant for p values <0.05.
Unlike clinical trials, observational studies are prone to selection and indication bias, given that in routine clinical practice settings the probability of receiving one or another treatment option may be related to certain characteristics of individual patients; clinical trials minimise this problem through randomisation29. In our case, we used the propensity score (PS) (see Supplementary Material: Appendix 6 for more detail), which final goal is to achieve a covariate balance similar to that obtained through the process of random allocation in clinical trials, such that we are able to obtain an unbiased estimate of the effects, with comparison groups being identical except for the treatment.30 To this end, we used two techniques, namely, entropy balancing and generalised boosted regression modelling (GBM, gradient boosting machine)31,32. Both procedures are described in detail in the Supplementary Material, Appendix 6.
We conducted a combined multivariate analysis of total costs and QALY using a seemingly unrelated regression (SUR) method (see Supplementary Material: Appendix 7 for covariables), as it includes the correlation between the parameters of the two regressions (costs and QALY) in the analysis using the variance-covariance matrix.25,33 Finally, the ICER was calculated as the ratio between the β coefficients for each group in both regressions (cost and effectiveness).16,17,25
As the analysis used individual follow-up data, we calculated the individual ICER, and as a measure of uncertainty, the 95%CI by bootstrapping (2.5 and 97.5 percentiles), and the results were plotted in the cost-effectiveness plane.34 A sensitivity analysis on a range of price variations has been performed taking into account that generic DOAC will soon enter the market, leading to price reductions.
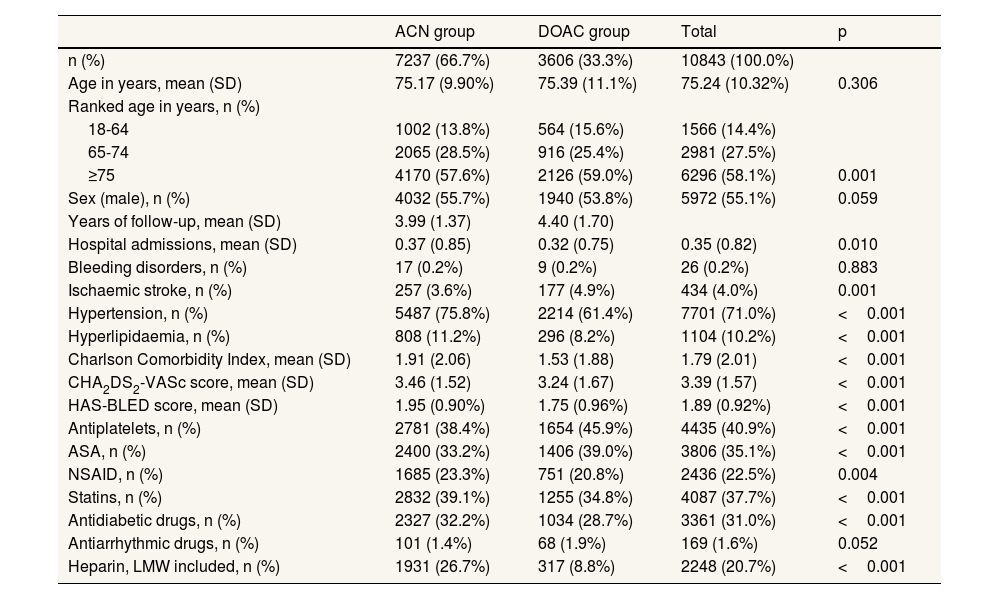
ResultsWe included 10,843 patients in this study (see Figure S1 in Supplementary Material: Appendix 8 for flowchart), the anticoagulant treatment started being ACN in 66.7% of cases and DOAC in the others (15.7% taking rivaroxaban, 11.6% apixaban, and 6.0% dabigatran) which characteristics were summarized in Table 1. The mean age in both groups was 75 years, but the ACN group had more hypertension and hyperlipidemia than DOAC (75.8% vs 61.4% and 11.2% vs 8.2%, respectively; p <0.001), but less previous ischemic stroke (3.6% vs 4.9%; p <0.001). Tables S2 and S3 in Supplementary Material show the number of events during follow-up in each group; and Supplementary Material: Appendix 10, a detailed information on resource use.
Baseline clinical features for acenocoumarol and direct oral anticoagulant cohorts.
| ACN group | DOAC group | Total | p | |
|---|---|---|---|---|
| n (%) | 7237 (66.7%) | 3606 (33.3%) | 10843 (100.0%) | |
| Age in years, mean (SD) | 75.17 (9.90%) | 75.39 (11.1%) | 75.24 (10.32%) | 0.306 |
| Ranked age in years, n (%) | ||||
| 18-64 | 1002 (13.8%) | 564 (15.6%) | 1566 (14.4%) | |
| 65-74 | 2065 (28.5%) | 916 (25.4%) | 2981 (27.5%) | |
| ≥75 | 4170 (57.6%) | 2126 (59.0%) | 6296 (58.1%) | 0.001 |
| Sex (male), n (%) | 4032 (55.7%) | 1940 (53.8%) | 5972 (55.1%) | 0.059 |
| Years of follow-up, mean (SD) | 3.99 (1.37) | 4.40 (1.70) | ||
| Hospital admissions, mean (SD) | 0.37 (0.85) | 0.32 (0.75) | 0.35 (0.82) | 0.010 |
| Bleeding disorders, n (%) | 17 (0.2%) | 9 (0.2%) | 26 (0.2%) | 0.883 |
| Ischaemic stroke, n (%) | 257 (3.6%) | 177 (4.9%) | 434 (4.0%) | 0.001 |
| Hypertension, n (%) | 5487 (75.8%) | 2214 (61.4%) | 7701 (71.0%) | <0.001 |
| Hyperlipidaemia, n (%) | 808 (11.2%) | 296 (8.2%) | 1104 (10.2%) | <0.001 |
| Charlson Comorbidity Index, mean (SD) | 1.91 (2.06) | 1.53 (1.88) | 1.79 (2.01) | <0.001 |
| CHA2DS2-VASc score, mean (SD) | 3.46 (1.52) | 3.24 (1.67) | 3.39 (1.57) | <0.001 |
| HAS-BLED score, mean (SD) | 1.95 (0.90%) | 1.75 (0.96%) | 1.89 (0.92%) | <0.001 |
| Antiplatelets, n (%) | 2781 (38.4%) | 1654 (45.9%) | 4435 (40.9%) | <0.001 |
| ASA, n (%) | 2400 (33.2%) | 1406 (39.0%) | 3806 (35.1%) | <0.001 |
| NSAID, n (%) | 1685 (23.3%) | 751 (20.8%) | 2436 (22.5%) | 0.004 |
| Statins, n (%) | 2832 (39.1%) | 1255 (34.8%) | 4087 (37.7%) | <0.001 |
| Antidiabetic drugs, n (%) | 2327 (32.2%) | 1034 (28.7%) | 3361 (31.0%) | <0.001 |
| Antiarrhythmic drugs, n (%) | 101 (1.4%) | 68 (1.9%) | 169 (1.6%) | 0.052 |
| Heparin, LMW included, n (%) | 1931 (26.7%) | 317 (8.8%) | 2248 (20.7%) | <0.001 |
ACN: acenocoumarol; ASA: acetylsalicylic acid; CHA2DS2-VASc: congestive heart failure, hypertension, age ≥75 (doubled), diabetes, stroke (doubled), vascular disease, age 65 to 74 and sex category (female); DOAC: direct oral anticoagulant; HAS-BLED: hypertension, abnormal renal and/or liver function, stroke, bleeding tendency or predisposition, labile international normalized ratio, and elderly; LMW: low molecular weight; NSAID: non-steroidal anti-inflammatory drugs; SD: standard deviation.
Table 2 lists the mean undiscounted costs, life years and QALY per patient and disaggregated by group. The group treated with DOAC had a longer follow-up (4.40±1.70 vs 3.99±1.37 years in the ACN group) and therefore higher QALY (4.08±1.10 vs 3.64±0.87), and costs (€8,915±5,503 vs €8,163±5,205).
Mean costs, life years, and quality-adjusted life years of acenocoumarol and direct oral anticoagulant cohorts (no discount applied).
| Costs,€ | Life years | QALY | ||||
|---|---|---|---|---|---|---|
| Cohort | Mean | SD | Mean | SD | Mean | SD |
| ACN | 8,163 | 5,205 | 3.99 | 1.37 | 3.64 | 0.87 |
| DOAC (overall) | 8,915 | 5,503 | 4.40 | 1.70 | 4.08 | 1.10 |
| Total | 8,413 | 5,318 | 4.13 | 1.50 | 3.79 | 0.97 |
ACN: acenocoumarol; DOAC: direct oral anticoagulant; QALY: quality-adjusted life years; SD: standard deviation.
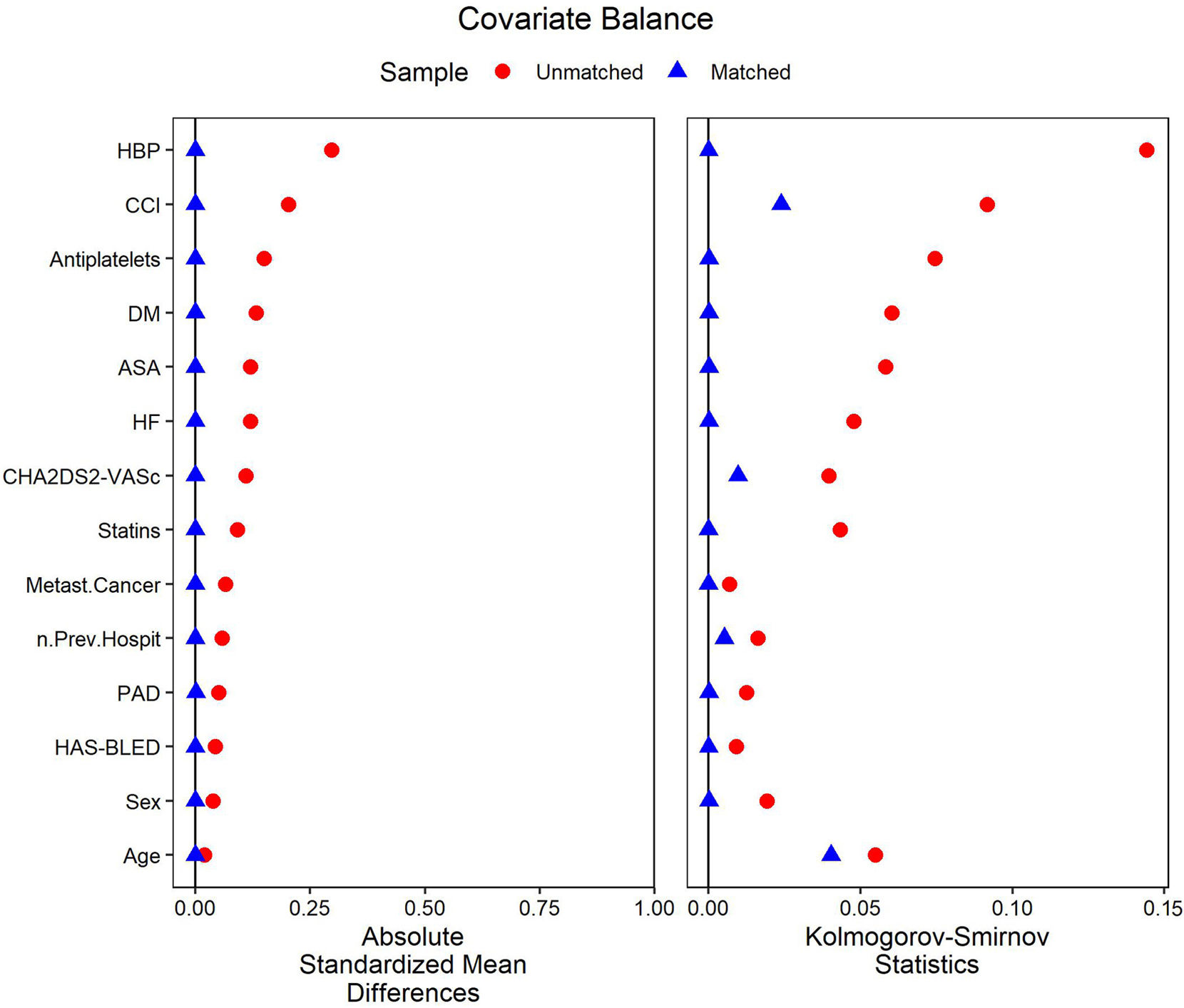
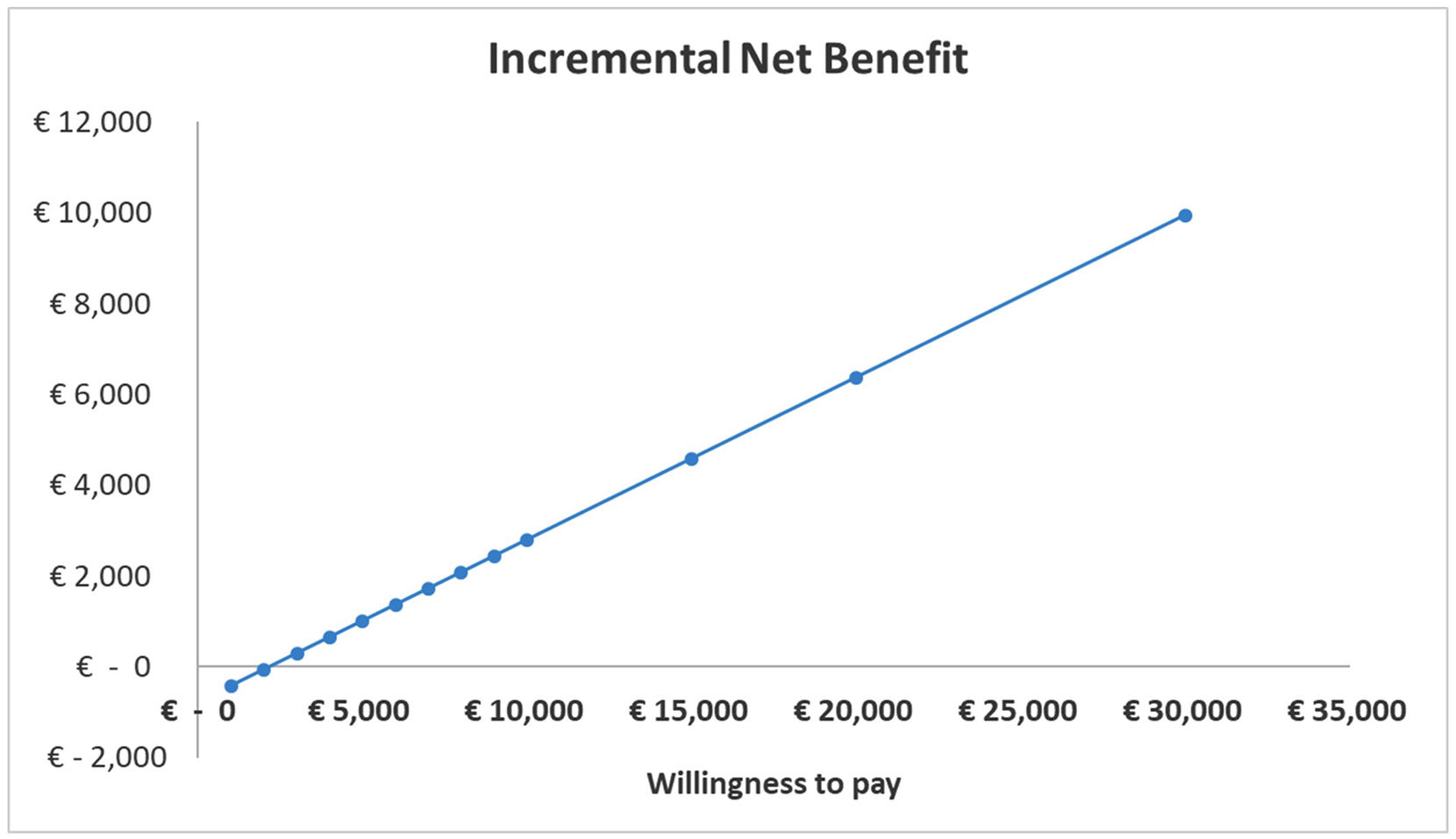
After applying PS based on entropy balancing, standardized mean difference were <0.1 for all covariates, indicating adequate covariate balance at baseline (Fig. 1). Based on these data, we calculated the ICER (for life year gained) and incremental cost-utility ratio (ICUR, for QALY gained) of DOAC compared to ACN. Along with crude estimates, Table 3 lists the ICER and ICUR obtained using SUR, entropy balancing, and GBM. The results yielded ICUR values of €1,732/QALY for crude estimates, €2,556/QALY for SUR procedure, €2,235/QALY for entropy balance procedure, and €2,278/QALY for GBM. The cost-effectiveness plane of the simulations obtained through bootstrapping is shown in Figure S4 in Supplementary Material, Appendix 11. The incremental net benefit for different WTP thresholds is only negative for values below €3,000/QALY (Fig. 2).

Covariate balance after matching using entropy balancing before the cost-effectiveness analysis. ASA: acetylsalicylic acid; CCI: Charlson Comorbidity Index; DM: diabetes mellitus; HBP: high blood pressure; HF: heart failure; Metast. Cancer: metastatic cancer; n.Prev.Hospit: number of previous hospitalizations; PAD: peripheral arterial disease.
Cost-effectiveness analysis of direct oral anticoagulants as a group compared to acenocoumarol using different methods for covariate adjustment with incremental cost-effectiveness ratios for life years gained and incremental cost-utility ratios for quality-adjusted life years.
| Method | Δ Costs,€ | Δ LYG | Δ QALY | ICER,€ | ICUR,€ |
|---|---|---|---|---|---|
| None | 752 | 0.413 | 0.434 | 1,823 | 1,732 |
| SUR | 1,109 | 0.367 | 0.434 | 3,021 | 2,556 |
| Entropy balance | 1,035 | 0.378 | 0.463 | 2,740 | 2,235 |
| GBM | 1,067 | 0.381 | 0.468 | 2,799 | 2,278 |
ACN: acenocoumarol; DOAC: direct oral anticoagulant; GBM: gradient boosting machine; ICER: incremental cost-effectiveness ratio; ICUR: incremental cost-utility ratio; LYG: life years gained; QALY: quality-adjusted life years; SUR: seemingly-unrelated regression.

The results of this study suggest that DOAC would be an effective treatment option for patients with NVAF compared to vitamin K antagonists, given that the ICUR is well below the range of €20,000 to 25,000/QALY, corresponding to WTP thresholds used in Spain.23 The results obtained using other methods of cost-effectiveness analysis were similar, reinforcing the robustness of this conclusion regarding DOAC. To our knowledge, this is the first cost-effectiveness study comparing DOAC and ACN using individual data of patients with NVAF in Spain, and for this, we have sourced data from the electronic health record of the Basque Health Service.
Most published economic evaluations on the treatment with DOAC in NVAF patients have used Markov models.11 In contrast, this study was based on real data on effectiveness and patient healthcare resource use (RWD), without requiring assumptions or parameterisation. Moreover, we should highlight that the sample size is very large, with follow-up data on the cohorts of up to 7 years, and that we have used methods for data adjustment and weighting recommended for accurately estimating the treatment effects in observational studies.14 These methods help to compensate for indication bias and balance baseline covariates to resemble randomised controlled trial designs.29,33 The good balance of 14 variables, including major comorbidities and the HAS-BLED major bleeding risk score, minimises the possibility of hidden variables biasing the results.
The results of this study are in line with recent economic evaluation studies in Spain on the treatment of NVAF patients with oral anticoagulants.11,12,35 The use of different adjustment methods yielded very similar ICER, ranging from €2,887/life years gained using SUR to €3,149/life years gained using entropy balancing. Similar results were also found for QALY, with values of €2,141/QALY using SUR and €2,556/QALY using full matching. We have not, however, found any similar pharmacoeconomic studies on anticoagulants from Spain using individual patient data and not based on modelling. The most similar study in terms of data and design is that of Escobar et al.12 concerning the updating of a previous Markov model, in which they used data from observational RWD studies conducted in other countries. In that study, dabigatran (€952/QALY) and rivaroxaban (€4,612/QALY) were found to be more effective than ACN (although this was not the case for apixaban).12 Other studies published35–38, performed from a public health perspective and using Markov modelling, have generally concluded that DOAC are an effective treatment option compared to ACN, although in some cases, they applied a WTP threshold of €30,000/QALY —a value used years ago— and have not been updated.35,36 A cost-effectiveness study using RWD is ongoing in Catalonia, but it is still at the development stage and results have yet to be published.39
In the international literature, most recently published studies have tended to show DOAC to be more efficient than warfarin, with ICER obtained decreasing as previous models are fed with real-world observational data. That is, the first economic evaluations,10,40,41 which were mainly based on pivotal randomised controlled trials, generally provided ICER that were over €20,000-30,000/QALY, values that nowadays would not be considered cost-effective,9,40,41 while economic evaluations published in recent years42–45 combining RWD and randomised controlled trials, above all those conducted in Europe, have usually found values below the €20,000/QALY threshold.42,43 The differences can be explained by the greater use of resources in clinical trials compared to clinical practice and the higher cost of healthcare in the United States of America, where the former were conducted. We could still have concerns about potential publication bias, that is, a failure to publish studies because they have obtained results that are negative or do not favour funding bodies. Nonetheless, a meta-analysis of the economic evaluations of DOAC compared to ACN11 found similar results to our study in terms of incremental net benefit per QALY (range of $6,632-7,664 vs €6,367 in our study).
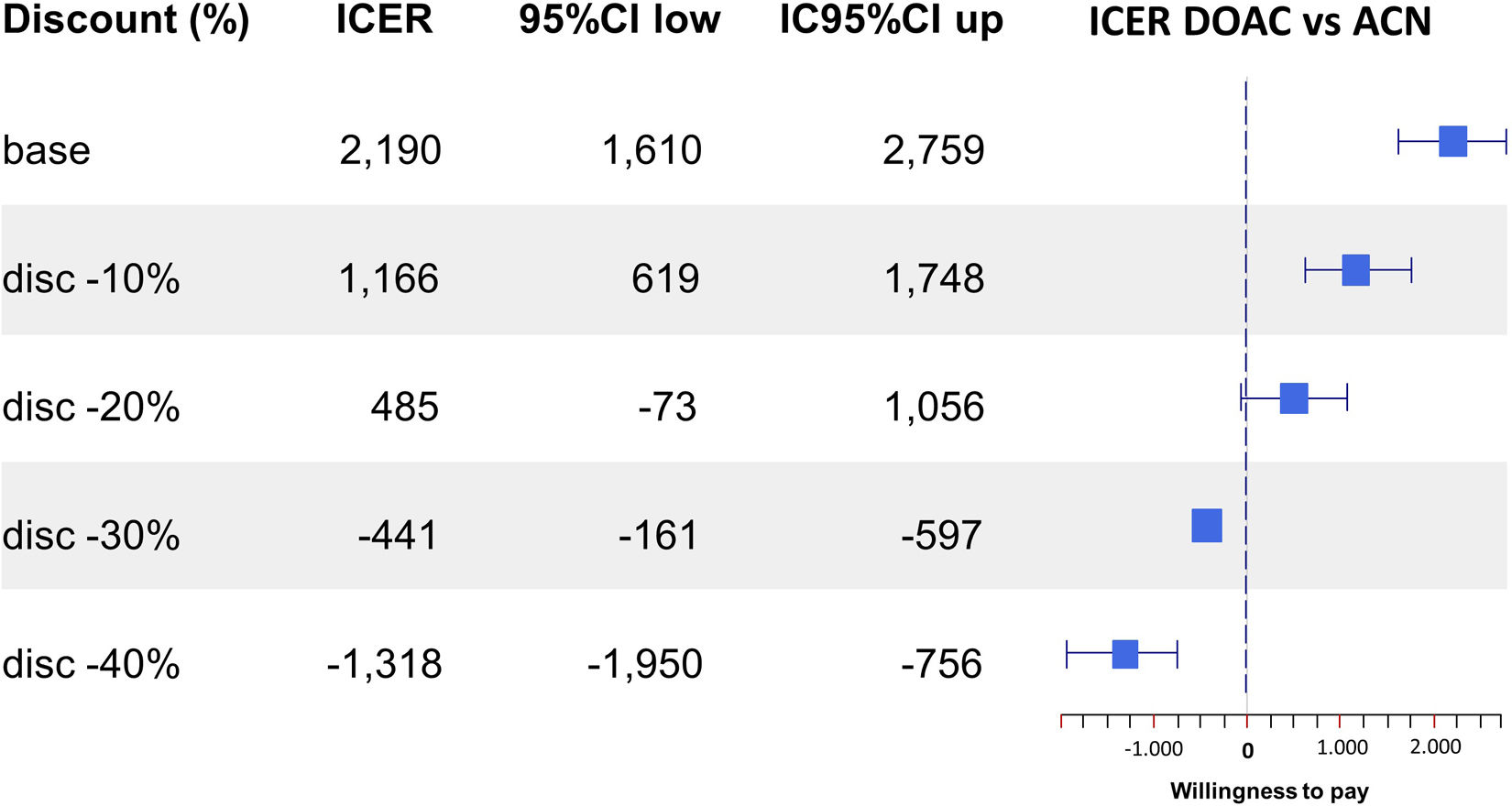
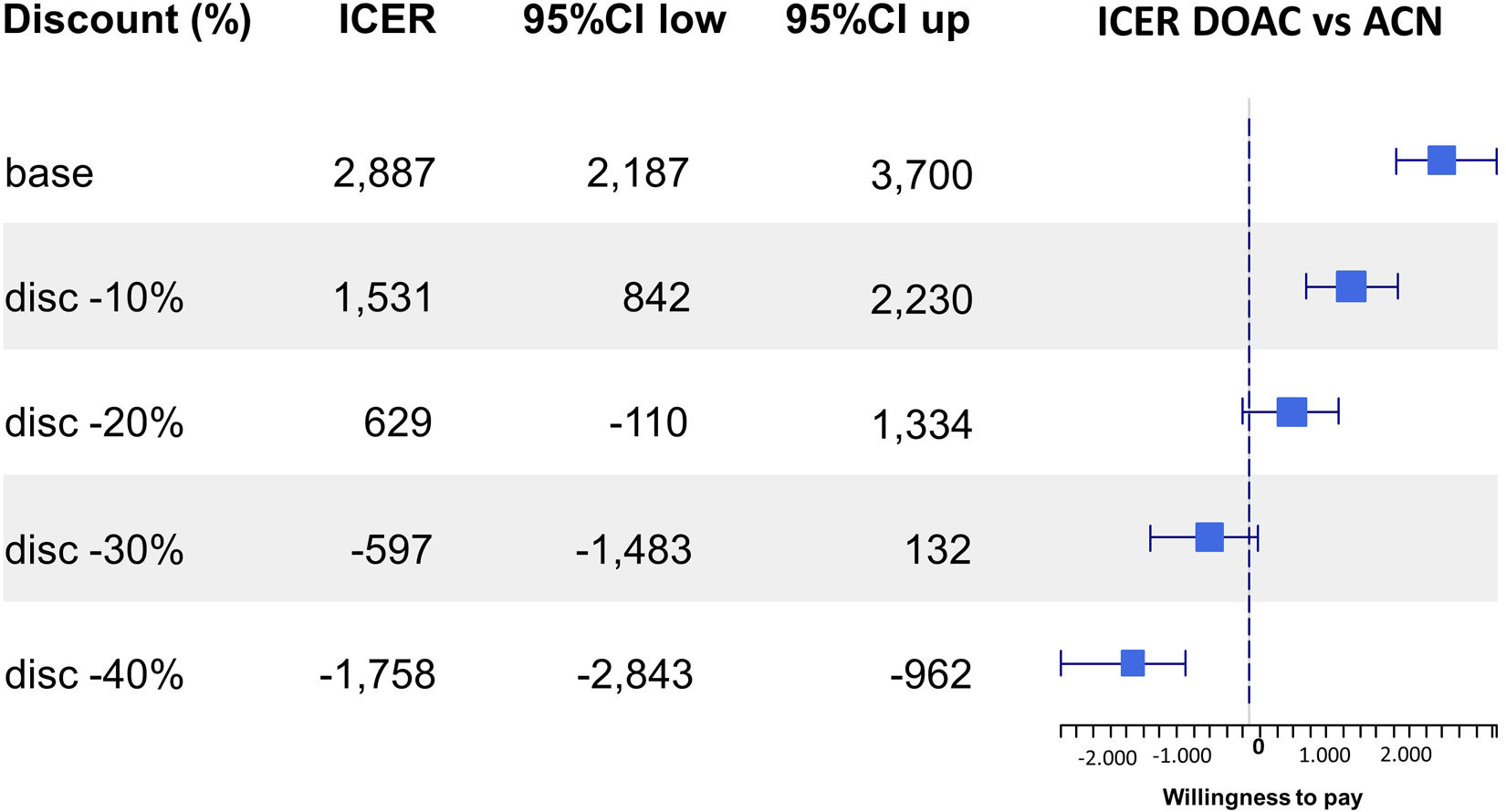
The largest cost component in the results is the cost of the drugs themselves, a unit cost that will change in the next few years. The patent for dabigatran expired in 2022 and those for the other DOAC that came onto the market later will do so over the next few years. As a consequence, the gradual entry onto the market of generic DOAC will lead to better results in economic evaluations based on the ICER and INB. The incremental cost may even become a net saving which would move the ICER to the dominant quadrant of the cost-effectiveness plane.21 As a sensitivity analysis, as shown in Figures 3 and 4, and in Figures S5 to S8 in Supplementary Material, Appendix 12, we considered the potential impact of potential price reductions for generic versions of these drugs on their cost-utility (QALY) and cost-effectiveness (life years gained); overall, discounts above 30% make DOAC dominant (not for apixaban, which shows a high variability and a very broad interval confidence range).

Sensitivity analysis on the incremental cost-effectiveness ratio of several price reductions by generic direct oral anticoagulant (DOAC) version (€/quality-adjusted life year). ACN: acenocoumarol; 95%CI: 95% confidence interval; disc: price discount rate; ICER: incremental cost-effectiveness ratio in €/QALY; QALY: quality-adjusted life years.

Sensitivity analysis on the incremental cost-effectiveness ratio of several price reductions by generic direct oral anticoagulant (DOAC) version (€/life years gained). ACN: acenocoumarol; 95%CI: 95% confidence interval; disc: price discount rate; DOAC: direct oral anticoagulant; ICER: incremental cost-effectiveness ratio in euros/life years gained.
As well as the use of real individual patient follow-up data and the large sample size, the strengths of this study lie in the application of innovative estimation techniques in the cost-effectiveness analyses and the consistency of the results obtained. In recent years, a growing number of techniques have been developed to assess the effect of treatments using RWD-based observational studies (PS adjustment, weighting methods, doubly robust estimation, and causal inference, among others).30–32,46 In many cases, their use allows us to obtain comparative effectiveness results with a similar level of rigour to that of randomised controlled trials. Nonetheless, we are not aware of studies in which these techniques have been developed to the same extent for the economic evaluation of treatments beyond basic PS-based matching techniques,47 and none regarding patients with NVAF treated with anticoagulants. In this study, we used traditional cost-effectiveness techniques as well as bias-control methods suitable for analysing observational data. In addition to a regression method, specifically, SUR, we have used entropy balancing, and a machine learning method, namely, GBM, not used in any economic evaluation studies retrieved from our literature search.
This study faced the challenge of addressing the limitations typical of retrospective observational research based on population-based healthcare administrative databases, such as issues concerning the completeness of records, accuracy of diagnostic coding, reliability of data retrieval, and the assumption that a condition is not present if it is not documented in the corresponding fields (for structured variables).48 From the economic side, a limitation of these sources is the lack of information on patient and family travel and its impact on indirect costs.49 Given the greater need for controls in the ACN treatment alternative, their inclusion would have strengthened DOAC as a cost-effective alternative.
The main conclusion of this study is that DOAC are currently a cost-effective option for the treatment of NVAF patients. Furthermore, the robustness of this conclusion is enhanced by the use of a study design based on clinical practice data and the achievement of similar cost-effectiveness results when applying several different techniques to adjust for the biases associated with observational studies.
Availability of databases and material for replicationData were provided by the Basque Health Service. Our data sharing agreement clearly stipulates that they cannot be shared with any third party.
Non-valvular atrial fibrillation (NVAF) is the most common type of chronic heart arrhythmia in adults and it has been estimated that this condition alone increases the risk of stroke and systemic embolism 4- to 5-fold. Anticoagulant treatment with acenocoumarol reduces the risk of ischemic stroke in patients with NVAF but with a narrow therapeutic window. Seeking to overcome these limitations, several new direct oral anticoagulants (DOAC), have been approved. Economic assessments of the efficacy of the new DOAC have been published but the results vary considerably.
What does this study add to the literature?The incremental cost-effectiveness ratio of DOAC compared to acenocoumarol ranged from €1732 to €2556/quality-adjusted life years (QALY), while the incremental net benefit for different willingness-to-pay thresholds was only negative for values below €3000/QALY. DOAC would be an efficient alternative for the treatment of patients with NVAF, based on real-world data and consistent results through different techniques to adjust for bias associated with observational studies.
What are the implications of the results?The results of this economic evaluation demonstrate that DOAC are highly efficient with respect to vitamin A inhibitors, being these results robust by using different techniques to adjust for the bias associated with observational studies, including machine learning ones.
The corresponding author, on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsI. Gorostiza and J. Mar conceived, designed the research and wrote the first version of introduction and discussion. A. Bilbao obtained the data, and interpreted the data, helping to write results and discussion. All authors revised the manuscript for important intellectual content and approved the final manuscript.
AcknowledgementsWe would like to acknowledge the help of INC in improving the use of English in the manuscript.
Ethics approvalThe authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. All procedures involving human subjects/patients were approved by the Clinical Research Ethics Committee of Euskadi (code number: EPA2017040).
FundingThis work is supported by the Department of Health of the Basque Government through its 2016 Call for Grants for Health Research Projects (ref. 2016111056).
Conflicts of interestI. Gorostiza and A. Bilbao declare no conflict of interests. J. Mar's institution received an unrestricted grant from Daiichi Sankyo Spain.












