



In the last few years, a striking increase in the number of cancer survivors (CS) has been observed, mainly due to the increment in the number of new cases of cancer being diagnosed and the use of more effective treatments. This fact brings new challenges for health services, since CS often experience late and long-term adverse effects of cancer and its treatments,1 including second primary cancers, cardiovascular complications, depression, pain or fatigue, which may contribute for a poorer perceived health status and a greater use of health care.2 In addition, a life event such as cancer can be a teachable moment, providing many opportunities to improve health knowledge and behaviours. However, the information needs of CS are mainly treatment-related, with a marginal interest in surveillance and health information,3 which can hamper the adoption of healthier behaviours, although CS are, in general, more likely to seek cancer information than individuals without this disease (NC).4
In this context, we compared CS and NC regarding cancer-related knowledge, health status, health care use and lifestyles. We selected CS and sex-, age- and education-matched (1:4) NC, among participants of a national population-based cross-sectional study.5 A total of 39 CS, corresponding to a prevalence of 1.4%, and 156 NC were included in this study. Data was collected through face-to-face interviews, using a structured questionnaire, and the effect of a previous diagnosis of cancer was quantified through prevalence ratios (PR), and respective 95% confidence intervals (95% CI).
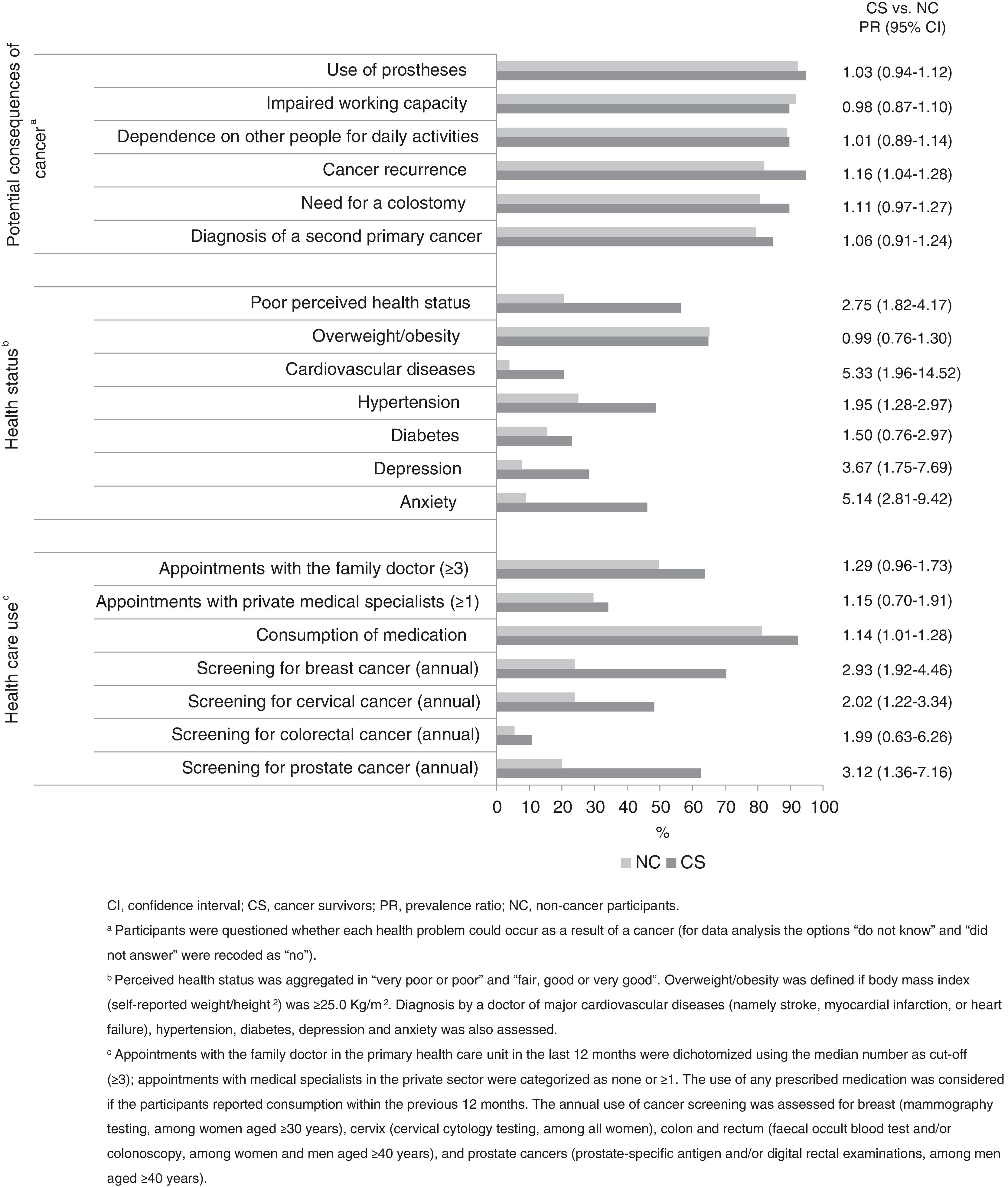
Figure 1 depicts the perception of potential consequences of cancer, health status and health care use among CS and NC. Except for “impaired working capacity”, CS tended to identify more often all health problems as potential consequences of cancer, with significant differences for “cancer recurrence” (PR=1.16; 95%CI: 1.04-1.28). They also reported a poorer health status (PR=2.75; 95%CI:1.82-4.17) and greater prevalence of cardiovascular diseases (PR=5.33; 95%CI:1.96-14.52), hypertension (PR=1.95; 95%CI: 1.28-2.97), depression (PR=3.67; 95%CI: 1.75-7.69) and anxiety (PR=5.14; 95%CI: 2.81-9.42). Consumption of medication (PR=1.14, 95%CI: 1.01-1.28), annual screening for breast (PR=2.93; 95%CI: 1.92-4.46), cervix (PR=2.02; 95%CI: 1.22-3.34) and prostate cancers (PR=3.12; 95%CI: 1.36-7.16) were more frequent among CS.

Regarding the most important behaviour for cancer prevention, CS tended to refer more frequently “regular check-ups”, “healthy diet” and “not drinking”, and less often “not smoking” and “blood analysis”, albeit these associations were not statistically significant. Additionally, no statistically significant differences were observed between CS and NC regarding smoking, alcohol intake, consumption of fruits and/or vegetables, and physical activity.
In conclusion, this exploratory investigation has shown that, among CS, there is margin for improvement of knowledge about oncological diseases, and health promotion interventions targeting this specific population are needed. It also confirmed a worse health status, and a higher use of health care resources among CS, particularly concerning the consumption of medication and cancer screening. Hence, the present work provides a benchmark to design and evaluate the effectiveness of knowledge-raising activities targeting CS, to understand the burden of cancer survivorship, and to allocate appropriate resources for national cancer survivorship care plans.
Authorship contributionsA. Rute Costa collaborated in the analysis and interpretation of the data and has written the first draft of the letter. P. Moura-Ferreira participated in the design of the survey, reviewed and revised the letter critically for important intellectual content. N. Lunet participated in the design of the survey, defined the specific objectives and strategy of data analysis for this report, collaborated in the analysis and interpretation of the data, and reviewed the letter critically for important intellectual content. All authors approved the final version of the manuscript.
FundingThis study was funded by FEDER through the Operational Programme Competitiveness and Internationalization and national funding from the Foundation for Science and Technology–FCT (Portuguese Ministry of Science, Technology and Higher Education), under the project “Health information of Portuguese population: Knowledge and perceived quality and accessibility of health information sources” (Ref. FCT: HMSP-IISE/SAU-ICT/0004/2009), and the Unidade de Investigação em Epidemiologia - Instituto de Saúde Pública da Universidade do Porto (EPIUnit) (POCI-01-0145-FEDER-006862; Ref. UID/DTP/04750/2013). Individual grant attributed to ARC (SFRH/BD/102181/2014) was funded by FCT and the “Programa Operacional Capital Humano” (POCH/FSE).
Conflicts of interestNone.











