




The main objective of this study is to analyse the role of alcohol consumption on lung cancer risk in people who have never smoked.
MethodsWe conducted a systematic review of the scientific literature following the PRISMA statement. We searched Medline, EMBASE and CINAHL using different combinations of MeSH terms and free text. We included cohort studies, pooled cohort studies and case-control studies comprising at least 25 anatomopathologically-confirmed diagnoses of lung cancer cases, a sample size larger than 100 individuals and more than five years of follow-up for cohort studies. We excluded studies that did not specifically report results for never smokers. We developed a quality score to assess the quality of the included papers and we ultimately included 14 investigations with a heterogeneous design and methodology.
ResultsResults for alcohol consumption and lung cancer risk in never smokers are inconclusive; however, several studies showed a dose-response pattern for total alcohol consumption and for spirits. Heterogeneous results were found for wine and beer.
ConclusionNo clear effect is observed for alcohol consumption. Due to the limited evidence, no conclusion can be drawn for beer or wine consumption. There is little research available on the effect of alcohol on lung cancer risk for people who have never smoked, and more studies are urgently needed on this topic.
El objetivo principal es analizar el papel que el consumo de alcohol desempeña en el riesgo de cáncer de pulmón en personas que nunca han fumado.
MétodosSe ha realizado una revisión sistemática de la literatura científica siguiendo la Declaración PRISMA. Se realizaron búsquedas en Medline, EMBASE y CINAHL utilizando diferentes combinaciones de términos MeSH y texto libre. Incluimos estudios de cohortes, cohortes agrupadas y estudios de casos y controles que cumpliesen: mínimo de 25 casos de cáncer de pulmón confirmados por anatomía patológica, muestra total de al menos 100 individuos y más de 5 años de seguimiento en estudios de cohortes. Se excluyeron aquellos trabajos que no aportasen resultados individualizados para las personas no fumadoras. Se desarrolló una escala de calidad para valorar los trabajos incluidos. Finalmente, se incluyeron 14 investigaciones, con un diseño y una metodología heterogéneos.
ResultadosLos resultados para el consumo de alcohol y el riesgo de cáncer de pulmón en personas nunca fumadoras no son concluyentes. Sin embargo, varios estudios muestran un patrón de dosis-respuesta para el consumo total y para el consumo de bebidas espirituosas. Los resultados obtenidos para vino y cerveza son heterogéneos.
ConclusiónNo se observa un efecto claro para el consumo de alcohol. Debido a la limitada evidencia, no puede obtenerse ninguna conclusión para el consumo de cerveza y vino. Hay pocas investigaciones disponibles sobre el efecto del alcohol en el riesgo de cáncer de pulmón en personas que nunca han fumado. Se necesitan, con urgencia, más estudios sobre este tema.
Lung cancer is one of the most frequent cancers in the world. 1.8 million cases were estimated in 2012 (12.9% of total cancers).1 One in five cancer deaths is due to lung cancer, with 1.59 million estimated deaths in 2012. Lung cancer is the leading cause of cancer death among men worldwide.2 Around 10-25% of lung cancer cases occur among individuals who have never smoked.3 In fact, lung cancer in people who have never smoked has been proposed as an independent entity than that occurring in ever smokers.4–6 Lung cancer in persons who have never smoked would be the seventh cause of cancer death worldwide7 if ranked separately.
The epidemiology of lung cancer in people who have never smoked is not well known. Most part of the available literature refers to ever smokers. There are many risk factors for this specific disease, such as environmental tobacco smoke exposure,8 residential radon,9 occupation,10 or previous respiratory diseases.11 Regarding the effect of alcohol consumption and its types on lung cancer appearance, most studies have included mainly ever-smokers and the role of alcohol on the aetiology of lung cancer in patients who have never smoked is not clear. Some studies have observed that alcohol consumption might be a risk factor for lung cancer, with alcohol types (wine, beer, spirits) having a different effect on the onset of the disease.12 Total alcohol consumption has been associated with lung cancer,13,14 but red wine intake seems to be protective while the effect of beer is unclear.15,16
The role of tobacco in the aetiology of lung cancer cannot be disputed,17 but the situation changes when we address the role of alcohol. Analyzing exclusively people who have never smoked would disentangle the specific role of alcohol consumption on lung cancer risk in this subgroup.
Due the lack of information on the association of alcohol consumption and lung cancer risk in people who have never smoked, our main objective is to address whether alcohol consumption, and its different types (beer, wine and spirits) has any effect on the risk of lung cancer through a systematic review of the scientific literature.
A better understanding of the topic reviewed would allow better promotion and health education policies.
MethodsWe developed a systematic review of the scientific literature following the 2009 PRISMA statement.18
Literature searchWe carried out a comprehensive literature search in MEDLINE, EMBASE and CINAHL databases, in order to obtain studies investigating the relationship between lung cancer in persons who have never smoked and alcohol consumption.
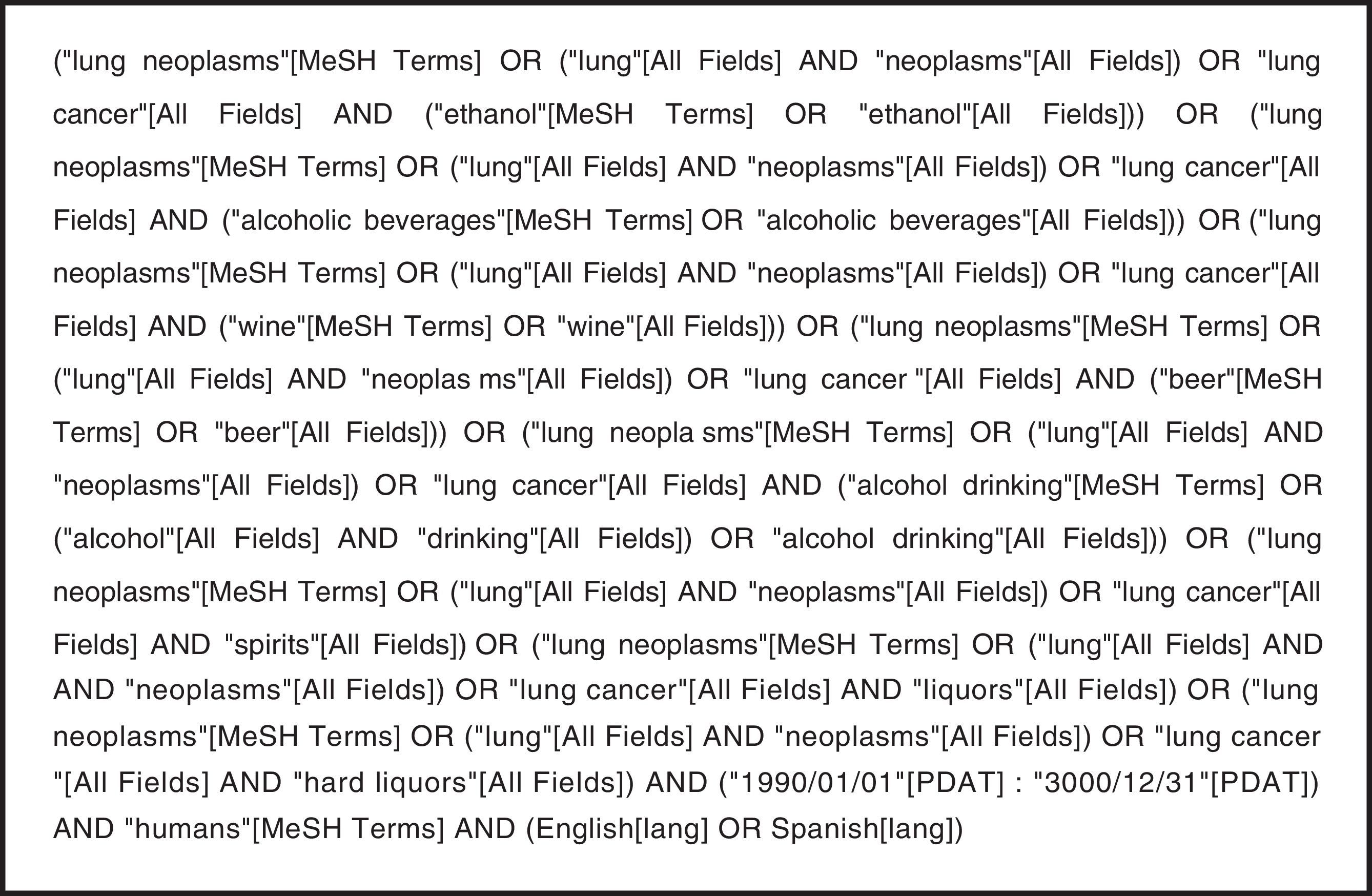
To retrieve information we used predefined search strategies. Particularly, to gather information in Pubmed database, we developed the strategy described in Figure 1 employing different combinations of MeSH terms (lung neoplasms, ethanol, wine, beer, alcoholic beverages, alcohol drinking) and free terms (lung neoplasms, lung, neoplasms, lung cancer, ethanol, wine, beer, alcoholic beverages, alcohol drinking, spirits, liquors, hard liquors). We also included additional relevant studies found after manually reviewing the references of the identified publications.

Our search covered the period comprised from the first of January 1990 to the present, and it was constantly updated until 10/03/2016. We included papers published in English and Spanish and performed in humans. We decided to cover this period trying to get accessible and scientifically current search results.
When several publications were performed on the same study, we included the most recent.
Inclusion and exclusion criteriaWe used the following criteria to include papers in the systematic review: a) regarding the study design we included: meta-analysis, pooling studies, cohort studies and case-control studies; b) regarding the sample size we included only those studies with at least 25 lung cancer cases on persons who had never smoked. The overall sample size had to be higher than 100 individuals; c) regarding lung cancer diagnosis we included only studies where anatomopathological diagnosis was confirmed; d) regarding the follow-up period for cohort studies: it should be at least five years and; e) regarding smoking: studies that did not differentiate the results for smokers and for people who had never smoked were excluded.
To be included in the category of person who has never smoked, participants in the different studies should meet at least one of the following conditions: had smoked no more than 100 cigarettes during their lifetime or less than 1 cigarette a day for a six-month period.19
Selection and data extraction process for included papersThe complete selection process was carried out by two of the authors (JAGL and ARR). The process began with a revision of the results obtained in the query of the three databases. The first screening was then performed by reading the titles and abstracts of the papers independently by both authors. Once this phase was completed, it held a sharing of initial selected studies by each, and consensus gave way to the selection of articles for full text reading. After reading them, both authors agreed in the final selected papers.
Data extraction was finally implemented by one author (JAGL). A common protocol was used to extract information homogeneously from all papers. If any difficulty arised for data interpretation during the procedure, the three authors resolved it by consensus.
Variables extractedInformation on the following variables was extracted and registered in Table I of the online Appendix of this article, from all included papers whenever available: first author and publication year; country or region where it was developed; number of never smoking cases and study design; percentage of female participants among people who have never smoked; number of covariates adjustment, mean or median age for cases and controls among people who have never smoked; relative risk for drinkers versus non-drinkers and 95% confidence intervals among people who have never smoked; lung cancer risk broken down by amount of alcohol intake and 95% confidence intervals among people who have never smoked.
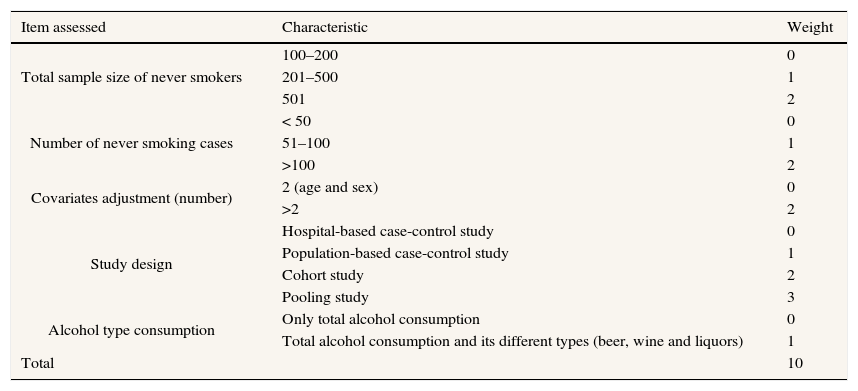
Assessment of the study qualityTo assess the quality of the included studies we designed a quality scale with five items which scored characteristics of the included studies. These items were: sample size, number of lung cancer cases in patients who had never smoked, results adjusted by covariates, study design, and alcohol types assessed. We assigned different weights to these characteristics allowing us to create a continuous scale. The scale with the different criterion and its weighting appears in Table 1. We have employed similar scales in systematic reviews in residential radon and lung cancer in never smokers20 and for residential radon and oral and pharyngeal cancers.21
Quality scale used to evaluate the included studies.
| Item assessed | Characteristic | Weight |
|---|---|---|
| Total sample size of never smokers | 100–200 | 0 |
| 201–500 | 1 | |
| 501 | 2 | |
| Number of never smoking cases | < 50 | 0 |
| 51–100 | 1 | |
| >100 | 2 | |
| Covariates adjustment (number) | 2 (age and sex) | 0 |
| >2 | 2 | |
| Study design | Hospital-based case-control study | 0 |
| Population-based case-control study | 1 | |
| Cohort study | 2 | |
| Pooling study | 3 | |
| Alcohol type consumption | Only total alcohol consumption | 0 |
| Total alcohol consumption and its different types (beer, wine and liquors) | 1 | |
| Total | 10 |
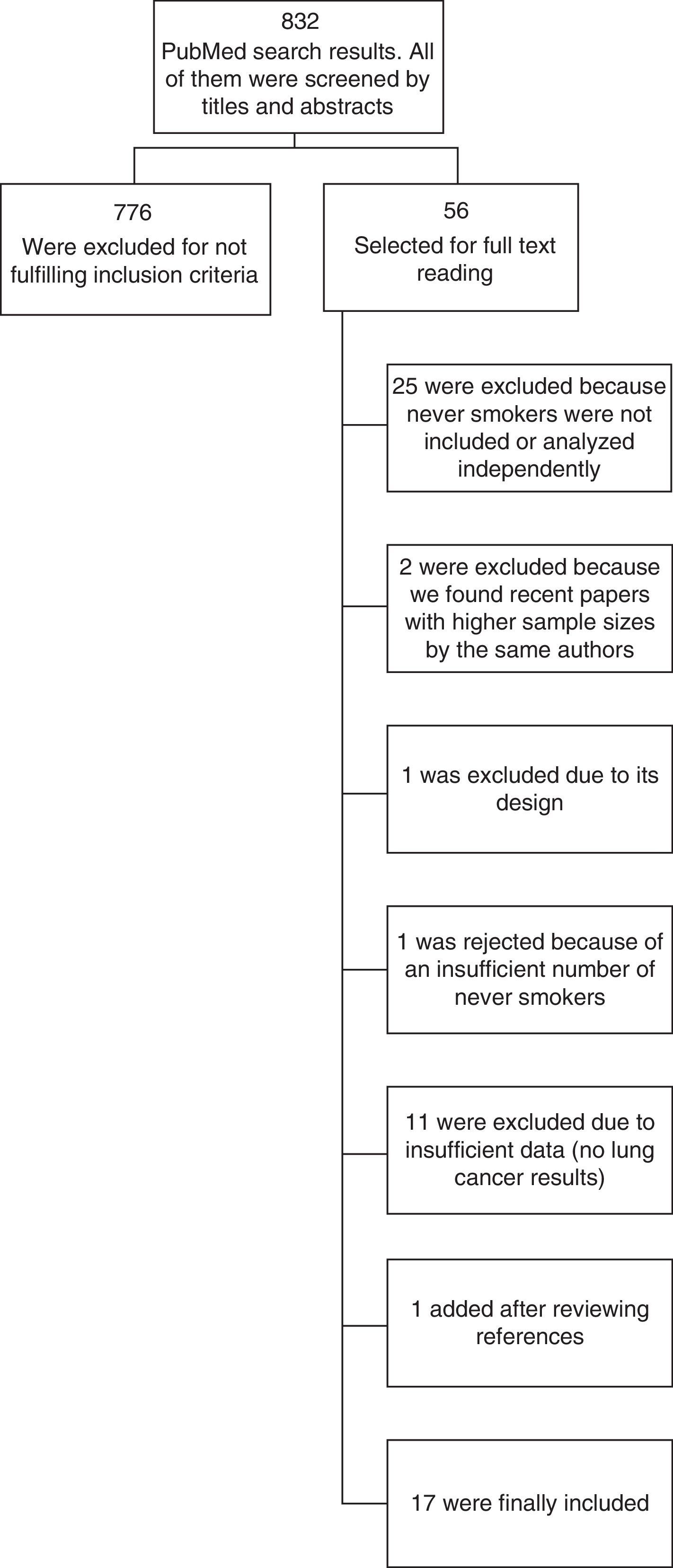
We obtained 832 papers through the literature search. After reading all the abstracts we selected 56 for full text reading. Of them, 25 were excluded because people who have never smoked were not included or analyzed separately, 2 were excluded because we found papers published later with higher sample sizes, 1 was excluded due to its design, 1 was rejected because of an insufficient number of never smoking cases, and 11 were excluded due to insufficient data (did not provide independent results for lung cancer, performed survival analysis, etc.).
We found one more study after reviewing the references in the identified papers, and finally we included 17 studies. A flowchart of the process appears in Figure 2.

Among the 17 included studies, the distribution by study design was as follows: 2 meta-analysis,13,14 1 systematic review,12 5 cohort studies,22–26 1 pooling study of cohort studies,27 4 population based case-control studies,15,28–30 3 hospital based case-control studies16,31,32 and 1 nested case-control study.33
Studies were conducted in a wide geographical distribution, covering: United States of America, Japan, Canada, China, Czech Republic, Poland, France, Italy, Spain, The Netherlands, United Kingdom, Greece, Germany, Sweden, Norway and Denmark.
The most recent study was published in 2016 and the oldest in 1996.
We only present results for case-control and cohort studies and show the results of meta-analysis or previous reviews only in tables because they include part of the studies that we are assessing individually.
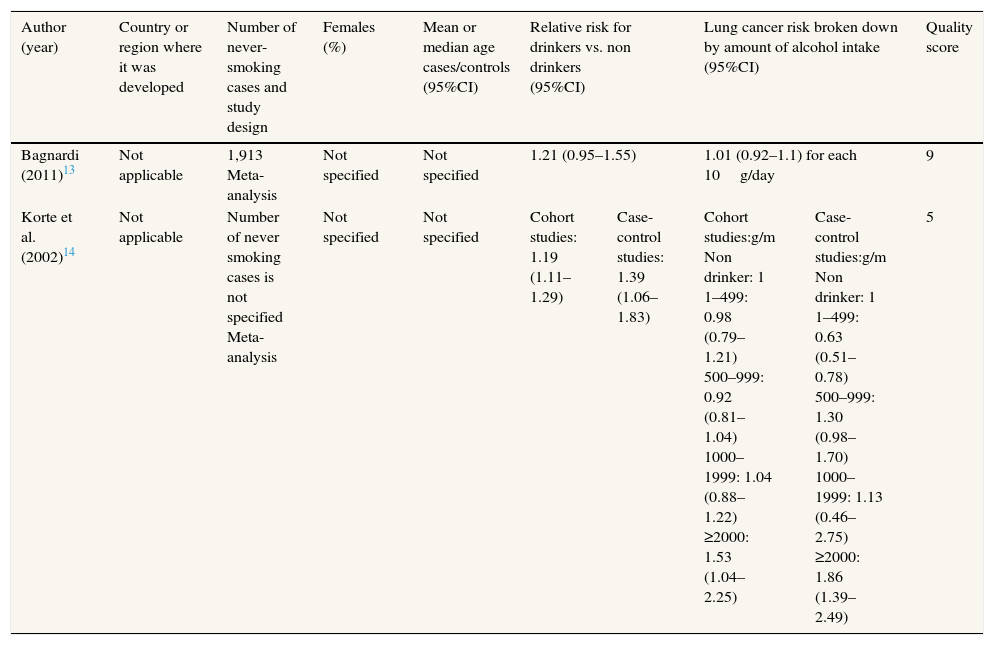
Results of the included studiesWe describe characteristics of the case-control and cohort studies included in Table I of the online Appendix of this article. On Table 2, we show the same information for meta-analysis, and in Table 3 we provide results for lung cancer risk broken down by type of alcoholic beverage.
Characteristics and data extracted from meta-analysis included.
| Author (year) | Country or region where it was developed | Number of never-smoking cases and study design | Females (%) | Mean or median age cases/controls (95%CI) | Relative risk for drinkers vs. non drinkers (95%CI) | Lung cancer risk broken down by amount of alcohol intake (95%CI) | Quality score | ||
|---|---|---|---|---|---|---|---|---|---|
| Bagnardi (2011)13 | Not applicable | 1,913 Meta-analysis | Not specified | Not specified | 1.21 (0.95–1.55) | 1.01 (0.92–1.1) for each 10g/day | 9 | ||
| Korte et al. (2002)14 | Not applicable | Number of never smoking cases is not specified Meta-analysis | Not specified | Not specified | Cohort studies: 1.19 (1.11–1.29) | Case-control studies: 1.39 (1.06–1.83) | Cohort studies:g/m Non drinker: 1 1–499: 0.98 (0.79–1.21) 500–999: 0.92 (0.81–1.04) 1000–1999: 1.04 (0.88–1.22) ≥2000: 1.53 (1.04–2.25) | Case-control studies:g/m Non drinker: 1 1–499: 0.63 (0.51–0.78) 500–999: 1.30 (0.98–1.70) 1000–1999: 1.13 (0.46–2.75) ≥2000: 1.86 (1.39–2.49) | 5 |
95%CI: 95% confidence interval.
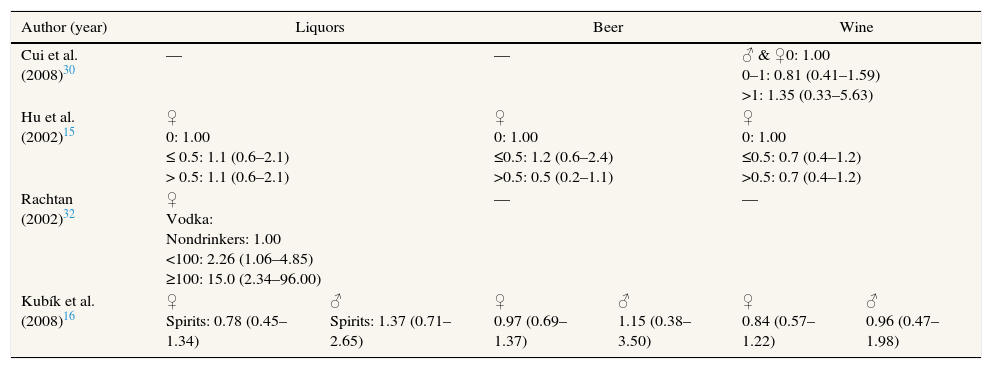
Lung cancer risk broken down by type of alcoholic beverage.
| Author (year) | Liquors | Beer | Wine | |||
|---|---|---|---|---|---|---|
| Cui et al. (2008)30 | — | — | ♂ & ♀0: 1.00 0–1: 0.81 (0.41–1.59) >1: 1.35 (0.33–5.63) | |||
| Hu et al. (2002)15 | ♀ 0: 1.00 ≤ 0.5: 1.1 (0.6–2.1) > 0.5: 1.1 (0.6–2.1) | ♀ 0: 1.00 ≤0.5: 1.2 (0.6–2.4) >0.5: 0.5 (0.2–1.1) | ♀ 0: 1.00 ≤0.5: 0.7 (0.4–1.2) >0.5: 0.7 (0.4–1.2) | |||
| Rachtan (2002)32 | ♀ Vodka: Nondrinkers: 1.00 <100: 2.26 (1.06–4.85) ≥100: 15.0 (2.34–96.00) | — | — | |||
| Kubík et al. (2008)16 | ♀ Spirits: 0.78 (0.45–1.34) | ♂ Spirits: 1.37 (0.71–2.65) | ♀ 0.97 (0.69–1.37) | ♂ 1.15 (0.38–3.50) | ♀ 0.84 (0.57–1.22) | ♂ 0.96 (0.47–1.98) |
- •
Cohort-studies and pooling studies of cohort studies: no study in this category22–27 found a positive association between overall alcohol consumption and lung cancer risk in people who have never smoked, even Troche et al.22 which analyzed the risk for total lung cancer broken down for histological types. Furthermore, one cohort study, by Rohrmann et al.25 considered two variables in relation to alcohol consumption (alcohol consumption at recruitment and mean lifelong alcohol consumption) and observed that moderate mean lifelong alcohol consumption was associated with lower lung cancer risk in comparison with low intake, HR: 0.45 (95%CI: 0.25-0.84). The pooling study of cohort studies by Freudenheim et al.27 observed a strong association for alcohol consumption (≥15g/d) in never smoking men with a relative risk of 6.38 (95%CI: 2.74-14.9). It included seven cohort studies conducted between 1980 and 1996 in different locations, with 247 never smoking cases.
- •
Case-control studies: in a population based case-control study most studies did not show a clear association between alcohol consumption and lung cancer risk in individuals who have never smoked. Tse et al.28 observed a small positive association for occasional (OR: 1.31; 95%CI: 0.80-2.14) and frequent (OR: 1.37; 95%CI: 0.80-2.32) never smoking drinkers, however statistical significance was not reached. The results observed in hospital based case-control studies are highly heterogeneous. Rachtan et al.32 described a higher lung cancer risk in lifelong consumption in persons who have never smoked with past vodka drinking with a positive dose response (RR: 2.26 and 95%CI: 1.06-4.85 for <100g/week; RR: 15.0 and 95%CI: 2.34-96 for ≥100g/week). We also included a nested case-control study33 where it was observed a positive dose response for alcohol intake and lung cancer risk in people who have never smoked (OR: 1.3 for 0.1-1 cups/day of saque and OR: 2.2 for ≥1.1 cups/day; one cup of 180mL of saque contains 27mL of ethanol).
Very few studies have analyzed the effect of different alcoholic beverages on lung cancer risk in people who have never smoked.15,16,30,32 There is no clear effect for any of them. Wine seems to have no effect and the same happens with beer consumption. No study made the difference between red wine and white wine. One study observed that spirits consumption was associated with an increased risk of lung cancer.32
Quality of the included studiesThe scoring of the included studies ranged between 1 and 10 points. The highest quality was for the pooling studies, with a sample size higher than 501 individuals and more than 100 never smoking cases. The average scoring of the included studies was 6.14.
DiscussionThis systematic review was conducted to clarify the effect of alcohol intake on lung cancer risk in people who have never smoked. There is no clear effect of alcohol consumption on lung cancer risk. While some studies do not show any effect, others show an increased risk with alcohol consumption. Few of them have even obtained a dose-response effect with the increase in alcohol consumption. Very few studies have analyzed the specific effect of different alcoholic beverages on lung cancer risk, nevertheless a low wine consumption is supposed to be protective and spirits are expected to be a risk factor. No hypothesis can be made for beer.
The quality of the included studies was moderate, with an average of 6.14 points. Most of the studies ranged between 5 and 7. Practically all studies adjusted their results by age and sex and very few had sample sizes higher than 500 participants.
The most important limitation to extrapolate results from the included studies is the extremely heterogeneity of the available investigations. Heterogeneity is present in the design, exposure measurement (grams per day, per week, per month, information retrieved or not on specific alcoholic beverages and different locations and populations). The included studies have been conducted throughout the World and represent different consumption patterns and different types of alcoholic beverages. A further limitation is the limited sample size of most available studies. Many of them have been designed to assess the effect of alcohol on lung cancer, and analysis of people who have never smoked is only a secondary result of the research. This situation conducts to obtain imprecise estimations with wide confidence intervals. In fact, there is only one observational study included with more than 1,000 participants. None of the remaining studies has more than 250 never-smoking cases.
For total alcohol consumption, six13,14,27,28,32,33 of the sixteen studies included in the review found a positive association. Four of them13,14,28,32 reported an overall relative risk for drinkers versus non-drinkers from 1.19 in a cohort study14 to 3.47 in a hospital based case-control study.32 One of them33 reported a positive dose response regarding to alcohol consumption, and the last one27 found a statistically significant association in men with alcohol consumption above 5 grams per day. Meta-analysis that we obtained through our search also achieved similar results. The most recent, published in 2011 by Bagnardi et al.,13 and the other, by Korte et al.,14 published in 2002, showed a positive association between alcohol and lung cancer, although the first one not reached statistically significance.
Our review includes three articles with specific results for wine consumption. It seems that low wine consumption acts as a protective factor against lung cancer in people who have never smoked. This protective effect ranges from 0.7 (95%CI: 0.4-1.2) for women who drunk no more than one glass per week in Hu et al.15 to 0.96 (95%CI: 0.47-1.98) for males in the study by Kubik et al.16 By contrast, for those who drunk more than one glass a day, Cui et al.30 found a positive association. However none of the studies reviewed reached statistical significance. Due to the limited evidence no conclusion can be done for wine consumption.
To address the effect of liquor and spirits, we have independent results in three investigations included in the review.15,16,32 It seems also reasonable to hypothesize that lung cancer risk in people who have never smoked increases with this type of alcohol consumption. Except Kúbik et al.,16 the other authors reported a positive association.
Results obtained for beer consumption are heterogeneous, although a review by Bandera et al.12 concluded that there may be an association between beer consumption and lung cancer (though it also included ever-smokers), in our review only two papers have available data but with opposite results. Raising a hypothesis would require more data.
Two of the studies in this review included results for total lung cancer risk and for its different histological subtypes. Troche et al.22 developed an independent analysis for adenocarcinoma, squamous cell carcinoma, small cell carcinoma and undifferentiated carcinoma, but due to the limited number of cases among people who had never smoked, they lost statistical power for testing an association. Freudenheim et al.,27 Rohrmann et al.,25 Shimazu et al.,24 Rachtan,32 Zang et al.31 and Bagnardi et al.29 considered the first three subtypes, but they did not performed the analysis exclusively in never smoking individuals. Kubik et al.16 use never smokers as referent. Ethanol in alcoholic beverages is classified by the International Agency for Research on Cancer as a group 1 carcinogenic to humans.34
There are several possible physiological explanations by which alcohol acts as carcinogenic. Acetaldehyde, it's primary metabolite, forms adducts with DNA in cultured human epithelial cells35 and, coupled with the induction of cytochrome P-4502E1, increases production of reactive oxygen species and nitrogen species.36 Another explanation suggests that the penetration of carcinogens through the mucosa of upper aerodigestive organs is enhanced by the role of alcohol, which could act as a solubilising agent of these carcinogens.37 Other possible mechanism could be the change in methylation and gene control resulting from the interaction produced in the intake, absorption and metabolism of vitamin B12 and B6.38
On the other hand, some studies associate the consumption of alcohol to protective effect on lung cancer risk, due to lower concentrations of various systemic biomarkers of inflammation39 on moderate alcohol drinkers, and to reduced oxidative damage.40 It is worthwhile to highlight the particular effect of wine polyphenols, especially resveratrol, whose results from in vitro and laboratory animals experiments demonstrate that it might induce neoplasic cell apoptosis in several cancer types.41
There exists a risk of bias in the included studies. Most of them have only adjusted their results by age and sex and do not consider environmental tobacco smoke. Furthermore, no study has considered residential radon exposure. In any case, radon seems not to be associated with alcohol consumption and therefore could act only as an effect modifier but not as a confounding variable. The case is different for ETS exposure that might be associated with alcohol consumption, especially in hospitality environments (previous to tobacco laws enforcement). Finally, the possibility of publication bias exists. We should not disregard that studies finding no effect for alcohol consumption or its different types could have been rejected due to the possible lack of statistical significance.
The present systematic review has some advantages. We have designed a comprehensive search strategy to minimize the risk of losing relevant information, and a proof of this is that the initial screening obtained more than 800 items. All included articles were reviewed independently by two reviewers. We obtained the same information from all of them, as the result of a thoroughly extraction. Finally, all included items were rated on the quality scale developed specifically.
Regarding limitations, besides the aforementioned high heterogeneity, we might have missed some studies published in languages different than English or Spanish though we are not aware of missing any study due to language limitations in our search. It is possible that some of these papers have been published in journals not indexed in Medline, EMBASE or CINAHL. This heterogeneity has impeded to obtain a quantitative result through a meta-analysis. Some potential biases might be present in the assessed studies. It is known that between 5 and 10% of ex-smokers are usually classified as never smokers. Some people could underestimate alcohol consumption, especially in the highest intake group. This information bias can lead to make misclassification of the exposure and finally to underestimate the effect. A last limitation resides in the different measurement of alcohol consumption used in the included publications. The alcohol content of a glass of wine can be different in distinct locations and the same can happen with the conclusion regarding consumption.
Only one study considered when analyzing the effect of alcohol type total alcohol consumption as a control variable.30 It would have been very interesting to consider which percentage of total alcohol consumption comes from a specific beverage type, but this information was not available in the studies reviewed.
Regarding the study question, the relevance of the present findings for drinkers is uncertain. In any case, we have to highlight that given the lack of studies; the effect of alcohol drinking on lung cancer in individuals with the highest alcohol intake should not be disregarded. This affirmation is reinforced by the fact that ethanol has been classified as a human carcinogen.
ConclusionThe main conclusion might be that there is an impressive lack of knowledge on the effect of alcohol consumption on lung cancer risk in people who have never smoked. There is also hardly any information on different alcoholic beverages. With the available studies, it seems that alcohol consumption, especially in high amounts, seems to increase the risk of lung cancer in people who have never smoked. It is extremely important to make an effort to increase research available exclusively in never smokers individuals to better assess the role of tobacco consumption in this subpopulation.
Editor in chargeCarlos Álvarez-Dardet.
Authorship contributionsJ.A. García-Lavandeira and A. Ruano-Ravina performed the literature search and selected the papers to be included. A. Ruano-Ravina had the idea of performing the systematic review. J.M. Barros-Dios and J.A. García-Lavandeira decided the search strategy. All authors have provided critical input to the manuscript content and approve its final version. All authors are responsible of the manuscript content. This paper is part of the work conducting to the PhD degree of J.A. García-Lavandeira.
FundingThis paper has been funded by a competitive research grant of the Xunta de Galicia: 10CSA208057PR “Risk factors of lung cancer in never smokers: a multicentre case-control study in the Northwest of Spain.”
Conflicts of interestNone.












