



To identify the effect of social capital on adolescent smoking.
MethodA stratified random sample of 1313 7th and 8th grade students from three counties in Transylvania, Romania, completed a self-administered questionnaire on smoking-related knowledge, attitudes and behaviours. The impact of social capital was measured (personal and community activities, school achievements and smoking-related knowledge). Multivariate multinomial logistic regression models were used to measure the association between social participation and smoking.
ResultsExperimenting with smoking was mostly related to knowledge about smoking, academic performance and second-hand tobacco smoke exposure at home. The strongest risk factor of adolescent smoking was the smoking behaviour of classmates: those who reported a significant proportion of smokers among their classmates were nine times more likely to smoke themselves than in other cases (adjusted odds ratio [aOR]: 9.05). Those who considered smoking to be harmless were 4 times more likely to be smokers than those who considered this behaviour to be dangerous (aOR: 4.28). Poor academic results increased adolescents’ smoking (aOR: 3.22 and 2.66). The odds were significantly higher for smoking, if they had an active social life (aOR: 2.54). Regular church attendance proved to be a protective factor (aOR: 0.45).
ConclusionsSeveral social capital factors can play a role in adolescent smoking. The organization and the development of community activities aimed at prevention must strengthen the factors related to the community's social capital to reduce the likelihood of teenage smoking.
Evaluar el efecto del capital social sobre el consumo de tabaco en adolescentes.
MétodoEl estudio se realizó en un grupo aleatorizado y estratificado compuesto por 1313 estudiantes de séptimo y octavo grado de tres municipios en Transilvania (Rumanía). Los participantes contestaron un cuestionario autocumplimentado en relación con el consumo de tabaco y sobre actitudes y comportamientos respecto a este. El impacto del capital social, entendido como actividades personales y comunitarias, así como el desarrollo académico y la información sobre el consumo de tabaco, fueron algunas de las medidas.
ResultadosExperimentar con el hábito de fumar se relaciona principalmente con el conocimiento sobre dicha adicción, el rendimiento académico y la exposición al consumo de tabaco en el hogar. El mayor riesgo para el consumo se deriva de la interacción con compañeros de clase que incurren en el consumo de tabaco. En tal caso, la probabilidad de consumo aumenta nueve veces (odds ratio ajustada [ORa]: 9,05). Quienes consideraron que fumar es inofensivo tuvieron cuatro veces más probabilidades de ser fumadores que quienes consideraron este comportamiento como peligroso (ORa: 4,28). En cuanto a los/las estudiantes con bajo rendimiento académico se observa un mayor incremento del consumo (ORa: 3,22 y 2,66). Al mismo tiempo, dicho patrón también se observa entre aquellos/as con un entorno social activo (ORa: 2,54). La asistencia a la iglesia de manera regular es un factor protector (ORa: 0,45).
ConclusionesDiferentes aspectos relacionados con el capital social se asocian al consumo de tabaco en adolescentes. La organización de actividades y el desarrollo comunitario deberán tener en cuenta estos aspectos para prevenir el consumo de tabaco. Hay que prestar especial atención a la clase social con el fin de reducir las probabilidades de consumo en adolescentes.
“Social capital” has been defined as the sum of the resources, actual or virtual, that accrue to an individual or a group by virtue of possessing a durable network of more or less institutionalized relationships of mutual acquaintance and recognition.1 Others note that social capital is built on trust, norms and networks, which enable self-affirmation and development.2,3 Moreover, social capital has been seen as a sustaining resource for social action and a contributor to population health as interpersonal relationships among people have impacts on health.2 Social capital acts through the relationship system that ensures pro-social motivation, through information channels, as well as obligations/expectations and norms/sanctions.4,5 This is an effect that can be a community-level protective factor; for example, if an adolescent is connected to the community through a strong network of contacts, then he/she internalizes the community expectations, which fosters pro-social behavior.
Adolescence is a turbulent time of attitudinal and behavioral development, often marked by the experimentation with risky behaviors such as the use of tobacco products. In Romania, according to a survey made in 2014, the adolescent smoking is a prevalent behavior, and the prevalence of weekly smoking increases by age: in 13-year-olds 6% of girls and 8% of boys, while for the 15-year-olds, 17% of girls and 20% of boys smoked.6
The local community is the natural living space, where the socio-cultural conditions are identical. It is a social structure where the members of the community are in consistent interaction; they have mutual values, interests, experiences and common expectations. The feeling of belonging, cohesion are the forces that result in its members having an influence on each other. Although the local communities in the counties we have studied, preserve traditions and retain deep community values, the sense of belonging and cooperation among residents seems to be weakening.7
We have tried to evaluate how the adolescents could make use of the social capital of local communities as they navigate the transition to adulthood. More specifically, which of the variables of social capital factors are most related to smoking behavior.
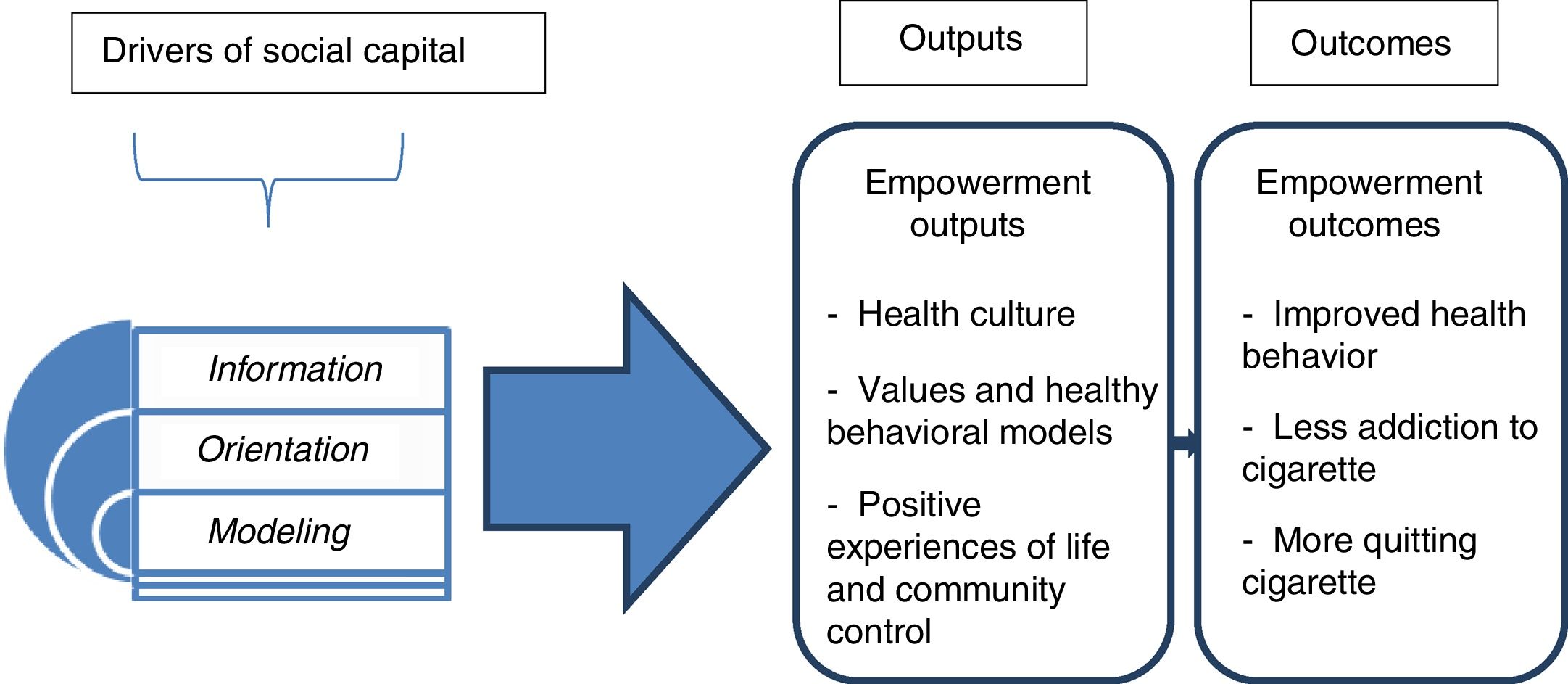
The aim of our study was to identify and explore the risks or protective factors embedded in the social capital construct, based on the three dimensions: information, orientation and modeling (Fig. 1) as related to the adolescent tobacco use.

We hypothesized that community activity, smoking among classmates, and school performance (as a marker for motivation for performance) are variables with significant impact on adolescent smoking.
The conceptual framework of the studyOur study is built on the Bourdieu and Wacquant's social capital theory,1 as well as on the Cultural Capital, and Community Empowerment Frameworks and the Information-Motivation-Behavioral Skills Model.8–10 The latter model describes how the development of motivation, information and behavioral skills leads to changes in behavior.9 While in the Cultural Capital Framework model the individuals’ socio-cultural environment affects their attitudes, values, and aspirations,10 the Community Empowerment Framework11 shows the recursive relationship between the policy intervention and the individual behavior in generating community empowerment. These models explain how interventions aiming at behavior change can be effective. Our study does not examine the effectiveness of an intervention, but it investigates the impact of the environment where adolescents live and act, focusing on the role of social participation and networks, among the various approaches of social capital.
We believe that behavior change may also occur if proper behavior models and values are present in adolescents’ lives and they are motivated enough to embrace them.
The framework of the study was developed based on the previously described models, but with a broader interpretation of concepts. We propose three main drivers of social capital (information, orientation and modeling) which shape the relationship between social capital and adolescent smoking (Fig. 1).
Information refers to the knowledge concerning a healthy lifestyle, which in case of anti-tobacco communication, can be acquired within the local community. Orientation is a much broader concept than the enhancement of motivation. It is related to the personality (identity, axiological orientation), the socio-cultural situation, (e.g. the family's financial situation), the developmental stage of the settlement and the school. It indicates the involvement in the community life, and it facilitates the modification of the adolescent's behavior also, according to the pro-social norms. And finally, in addition to providing cues for pro-social behavior and skills, modeling also contributes to self-determination and development of interpersonal skills.
MethodsStudy design and samplingA cross-sectional, questionnaire-based survey was administered to students in three Romanian counties (Mureș, Harghita and Covasna) in March 2014. A random, stratified, multistage sampling procedure was employed, based on enrollment records from the county school inspectorates. First, 36 strata were formed based on background variables such as county, settlement size, teaching language and grade.
In total, students from 36 schools in 26 settlements were sampled. Across the schools, 72 classrooms of 7th and 8th grade students (13-15 years-old) were sampled yielding a total of 1,313 respondents; 74 respondents were excluded from the analyses because of missing data. More than half (57%) studied in the Romanian language and 43% in the Hungarian language.
All procedures performed in this study were in accordance with the 1964 Declaration of Helsinki and its later amendments. We previously obtained written permission from schools’ inspectorates, headmasters (school management) and parents for conducting the survey. All parents were informed about the purpose, benefits and risks of the study. Participation in the study was optional. As the analysed unit was the class in all cases, all the consenting students, regardless of gender, filled in the questionnaire.
MeasuresThe self-administered questionnaire included both standardized questions from published sources, as well as questions developed by the research team.12,13 After the pilot test, the questionnaire was calibrated so that all students could respond to all questions within an average completion time of 40-45minutes. The survey contained 61 questions, generating 210 variables for analysis.
VariablesDemographic variables included the gender and the age. Students were classified into three groups according to their self-reported smoking status: never smokers, experimenters and smokers. Experimenters were defined as those who had lit a cigarette only once in their whole life.
The components of the model shown in Figure 1 were described using the following variables:
1) Information
The knowledge about smoking was measured with an index consisting of three questions: how dangerous you consider smoking to be, how easy or hard do you find quitting smoking, and how harmful is smoking in general. Mean responses were divided into the following categories: less than 3 points, “smoking is harmless”; between 3.0-3.9 points, “smoking is rather dangerous”; and 4 points, “smoking is very dangerous”.
2) Orientation
School results —as well as value achievements, motivation for performance— operationalized as respondents’ satisfaction with their school performance, was measured on a 1 to 10 scale. A distinct variable was developed to determine the level of the school, taking into account the school's average “capacity exam” score.
A community activity index was constructed from four questions: “Are there neighborhood gatherings in your residential area? Do you celebrate, have a good time together with your neighbors? Do you have fun, or do you play with your neighbors? How often do you participate in community programs?”. The variable was calculated based on the average of the standardized values of the four questions, which was divided into four categorical quartiles.
Church attendance was measured by four levels of frequency.
3) Modeling
Exposure to tobacco smoking at home was measured by the respondent report about how often he/she is in contact with others’ smoking in the home.
Smoker classmates was calculated as the average by class for respondent estimates of how many classmates smoke. From this, the share (percentage) of smokers was calculated in relation to the number of pupils per class, converted into four categories: very high (25%), high (17-25%), low (10-17%), and very low rate (<10%).
Smoking in the community was estimated by having respondents use a 0-10 scale to indicate how many out of ten adults smoke regularly in their area of residence (neighborhood). The values were divided into four categorical quartiles: very high, high, low and very low rate.
Four attitudes of the nearest neighbor towards smoking categories were created from answers to the question: “To what extent would your nearest neighbor oppose if they knew that you smoke?”. Categories were: very negative, prohibiting; rather negative, prohibiting; permissive; indifferent.
Statistical analysisBoth descriptive and inferential methods were used to describe the basic characteristics of the sample and answer our research questions. Simple frequency distributions were inspected to characterize the sample and background variables. The effect of the background variables on tobacco trial or smoking was examined using multivariate multinomial logistic regression analyses, after excluding the partial effects and multicollinearity. The clustering effect of classrooms was controlled through logistic regression methods.
The dependent variable within the multinomial regression models was the smoking status of the respondents, with never smokers as the reference category. Independent variables introduced in the model were basic demographic characteristics (age and gender), and variables from the orientation-information-modeling framework. We calculated the adjusted odds ratio (aOR) and 95% confidence interval (95%CI) for each variable, and p<0.05 was considered to be statistically significant. IBM SPSS version 23 was used for statistical analysis.
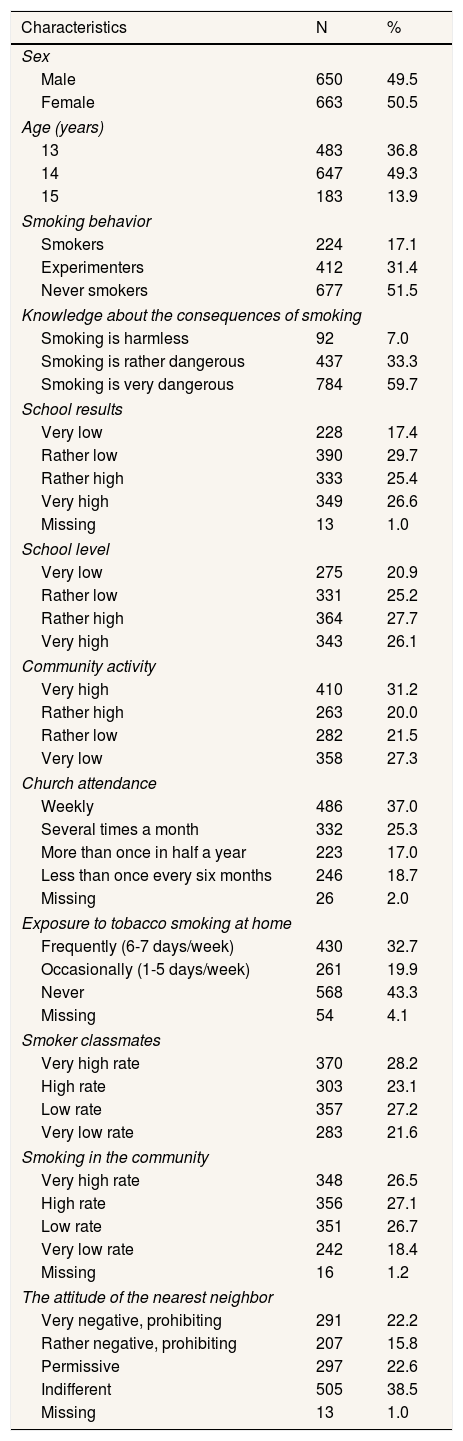
ResultsThe main characteristics of the sample are presented in Table 1.
Characteristics of the respondents (N=1313).
| Characteristics | N | % |
|---|---|---|
| Sex | ||
| Male | 650 | 49.5 |
| Female | 663 | 50.5 |
| Age (years) | ||
| 13 | 483 | 36.8 |
| 14 | 647 | 49.3 |
| 15 | 183 | 13.9 |
| Smoking behavior | ||
| Smokers | 224 | 17.1 |
| Experimenters | 412 | 31.4 |
| Never smokers | 677 | 51.5 |
| Knowledge about the consequences of smoking | ||
| Smoking is harmless | 92 | 7.0 |
| Smoking is rather dangerous | 437 | 33.3 |
| Smoking is very dangerous | 784 | 59.7 |
| School results | ||
| Very low | 228 | 17.4 |
| Rather low | 390 | 29.7 |
| Rather high | 333 | 25.4 |
| Very high | 349 | 26.6 |
| Missing | 13 | 1.0 |
| School level | ||
| Very low | 275 | 20.9 |
| Rather low | 331 | 25.2 |
| Rather high | 364 | 27.7 |
| Very high | 343 | 26.1 |
| Community activity | ||
| Very high | 410 | 31.2 |
| Rather high | 263 | 20.0 |
| Rather low | 282 | 21.5 |
| Very low | 358 | 27.3 |
| Church attendance | ||
| Weekly | 486 | 37.0 |
| Several times a month | 332 | 25.3 |
| More than once in half a year | 223 | 17.0 |
| Less than once every six months | 246 | 18.7 |
| Missing | 26 | 2.0 |
| Exposure to tobacco smoking at home | ||
| Frequently (6-7 days/week) | 430 | 32.7 |
| Occasionally (1-5 days/week) | 261 | 19.9 |
| Never | 568 | 43.3 |
| Missing | 54 | 4.1 |
| Smoker classmates | ||
| Very high rate | 370 | 28.2 |
| High rate | 303 | 23.1 |
| Low rate | 357 | 27.2 |
| Very low rate | 283 | 21.6 |
| Smoking in the community | ||
| Very high rate | 348 | 26.5 |
| High rate | 356 | 27.1 |
| Low rate | 351 | 26.7 |
| Very low rate | 242 | 18.4 |
| Missing | 16 | 1.2 |
| The attitude of the nearest neighbor | ||
| Very negative, prohibiting | 291 | 22.2 |
| Rather negative, prohibiting | 207 | 15.8 |
| Permissive | 297 | 22.6 |
| Indifferent | 505 | 38.5 |
| Missing | 13 | 1.0 |
The majority of the students were aware that smoking is very dangerous (59.7%), while only 7.0% considered it harmless. Half of the respondents (52.0%) were included in the “very high” and “rather high” school performance categories, with a similar distribution found for the quality of the school. Community activity was reported to be very high (31.2%) or high (20.0%) by most respondents. More than one-third (37.0%) reported attending church each week, while 18.7% of them reported attending church less half as frequently. Two-thirds of the students were exposed to secondhand smoke at least once a week. Very high levels of smoking were registered for students’ classmates (28.2%) and in the community (26.5%), and 38.0% of the respondents claimed that the nearest neighbor had a rejecting attitude towards smoking.
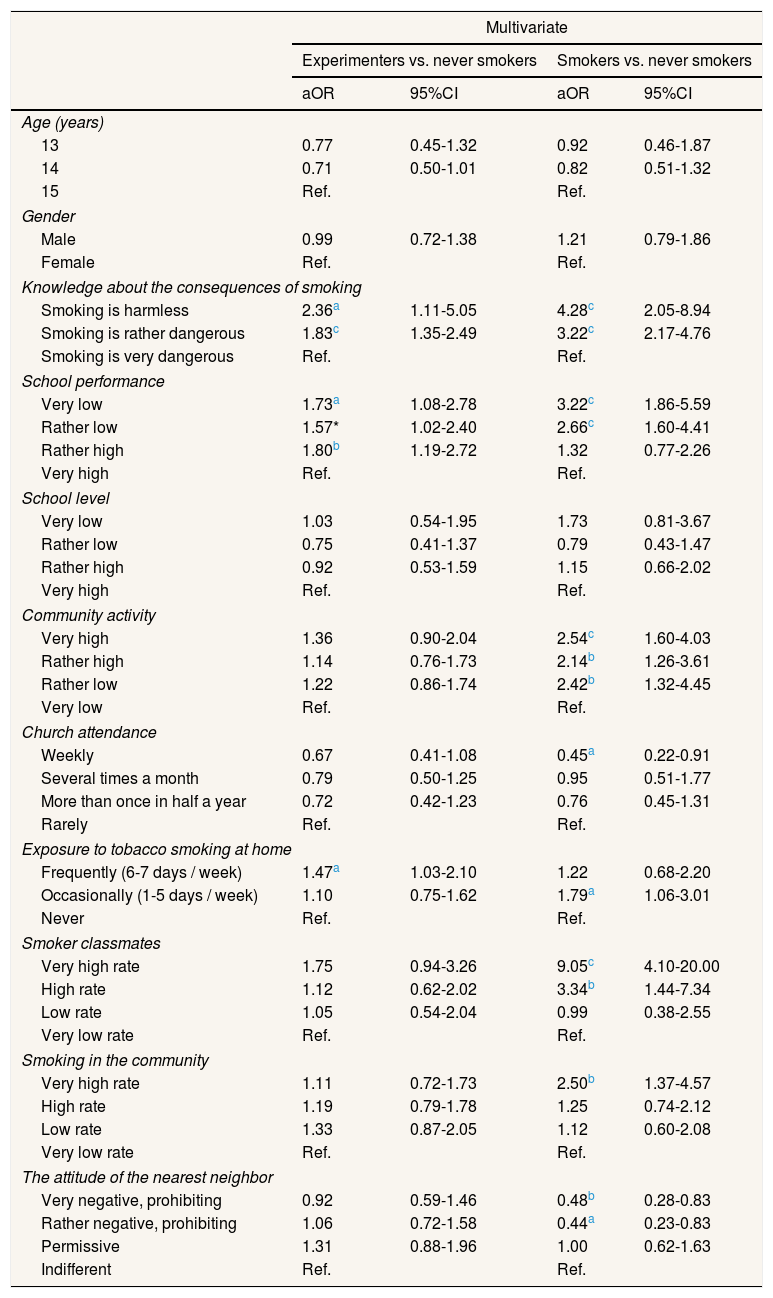
Controlling for all other factors in the model, experimenting with smoking is mostly related to knowledge about smoking (Table 2). Those who thought smoking was harmless or slightly dangerous were more likely to having had lit a cigarette in their life (aOR: 2.36, 95%CI: 1.11-5.05; and aOR: 1.83, 95%CI: 1.35-2.49, respectively). Academic/school performance is also important, as students with poor (very low and rather low) results were more likely to have tried cigarettes (aOR: 1.73, 95%CI: 1.08-2.78; and aOR: 1.57, 95%CI: 1.02-2.40, respectively), as well as those who are prone to exposure to tobacco smoke in the home (aOR: 1.47; 95%CI: 1.03-2.10).
Factors influencing tobacco smoking (multinomial logistic regression models).
| Multivariate | ||||
|---|---|---|---|---|
| Experimenters vs. never smokers | Smokers vs. never smokers | |||
| aOR | 95%CI | aOR | 95%CI | |
| Age (years) | ||||
| 13 | 0.77 | 0.45-1.32 | 0.92 | 0.46-1.87 |
| 14 | 0.71 | 0.50-1.01 | 0.82 | 0.51-1.32 |
| 15 | Ref. | Ref. | ||
| Gender | ||||
| Male | 0.99 | 0.72-1.38 | 1.21 | 0.79-1.86 |
| Female | Ref. | Ref. | ||
| Knowledge about the consequences of smoking | ||||
| Smoking is harmless | 2.36a | 1.11-5.05 | 4.28c | 2.05-8.94 |
| Smoking is rather dangerous | 1.83c | 1.35-2.49 | 3.22c | 2.17-4.76 |
| Smoking is very dangerous | Ref. | Ref. | ||
| School performance | ||||
| Very low | 1.73a | 1.08-2.78 | 3.22c | 1.86-5.59 |
| Rather low | 1.57* | 1.02-2.40 | 2.66c | 1.60-4.41 |
| Rather high | 1.80b | 1.19-2.72 | 1.32 | 0.77-2.26 |
| Very high | Ref. | Ref. | ||
| School level | ||||
| Very low | 1.03 | 0.54-1.95 | 1.73 | 0.81-3.67 |
| Rather low | 0.75 | 0.41-1.37 | 0.79 | 0.43-1.47 |
| Rather high | 0.92 | 0.53-1.59 | 1.15 | 0.66-2.02 |
| Very high | Ref. | Ref. | ||
| Community activity | ||||
| Very high | 1.36 | 0.90-2.04 | 2.54c | 1.60-4.03 |
| Rather high | 1.14 | 0.76-1.73 | 2.14b | 1.26-3.61 |
| Rather low | 1.22 | 0.86-1.74 | 2.42b | 1.32-4.45 |
| Very low | Ref. | Ref. | ||
| Church attendance | ||||
| Weekly | 0.67 | 0.41-1.08 | 0.45a | 0.22-0.91 |
| Several times a month | 0.79 | 0.50-1.25 | 0.95 | 0.51-1.77 |
| More than once in half a year | 0.72 | 0.42-1.23 | 0.76 | 0.45-1.31 |
| Rarely | Ref. | Ref. | ||
| Exposure to tobacco smoking at home | ||||
| Frequently (6-7 days / week) | 1.47a | 1.03-2.10 | 1.22 | 0.68-2.20 |
| Occasionally (1-5 days / week) | 1.10 | 0.75-1.62 | 1.79a | 1.06-3.01 |
| Never | Ref. | Ref. | ||
| Smoker classmates | ||||
| Very high rate | 1.75 | 0.94-3.26 | 9.05c | 4.10-20.00 |
| High rate | 1.12 | 0.62-2.02 | 3.34b | 1.44-7.34 |
| Low rate | 1.05 | 0.54-2.04 | 0.99 | 0.38-2.55 |
| Very low rate | Ref. | Ref. | ||
| Smoking in the community | ||||
| Very high rate | 1.11 | 0.72-1.73 | 2.50b | 1.37-4.57 |
| High rate | 1.19 | 0.79-1.78 | 1.25 | 0.74-2.12 |
| Low rate | 1.33 | 0.87-2.05 | 1.12 | 0.60-2.08 |
| Very low rate | Ref. | Ref. | ||
| The attitude of the nearest neighbor | ||||
| Very negative, prohibiting | 0.92 | 0.59-1.46 | 0.48b | 0.28-0.83 |
| Rather negative, prohibiting | 1.06 | 0.72-1.58 | 0.44a | 0.23-0.83 |
| Permissive | 1.31 | 0.88-1.96 | 1.00 | 0.62-1.63 |
| Indifferent | Ref. | Ref. | ||
aOR: adjusted odds ratio; 95%CI; 95% confidence interval; Ref.: reference value.
The strongest risk factor of adolescent smoking is the classmates’ (friends, peers) smoking behavior, suggesting that among adolescents in this study, smoking is a social environment-related activity. Independent of other factors, students who report a significant proportion of smokers among their classmates (more than a quarter) are 9 times more likely to smoke themselves than in other cases (aOR: 9.05; 95%CI: 4.10-20.00).
A second major factor is knowledge and attitude towards smoking. Those who consider smoking to be harmless are four times more likely to be smokers than those who consider this behavior very harmful (aOR: 4.28; 95%CI: 2.05-8.94). A third independent risk factor is related to the individual school performance: poor (very low and rather low) academic results increased adolescents’ odds of smoking (aOR: 3.22, 95%CI: 1.86-5.59; and aOR: 2.66, 95%CI: 1.60-4.41). A fourth factor is linked to social relationships, as smoking is strongly associated with intensive community activity; odds are significantly higher for smoking if they have an active social life (aOR: 2.54; 95%CI: 1.60-4.03). In the regression model, the perceived smoking rate in the respondent's community appears to be a stronger risk factor than smoking among family members (aOR: 2.50, 95%CI: 1.37-4.57; vs. aOR: 1.79, 95%CI: 1.06-3.01).
Variables such as regular church attendance and the prohibiting attitude of nearest neighbor proved to be protective factors for smoking. Respondents who attend church weekly were found to have less than half the odds of smoking as compared to those who rarely attend church (aOR: 0.45; 95%CI: 0.22-0.91). Also, if the nearest neighbor has a very negative (aOR: 0.48; 95%CI: 0.28-0.83) or rather negative (aOR: 0.44; 95%CI: 0.23-0.83) attitude towards adolescent smoking, it can be a protective factor.
According to the logistic regression analyses, the three components of our social capital model showed association with smoking behavior of the students. Considering “information” those who found smoking very dangerous, in case of “orientation” component those who had better school performance, and from the point of “modeling” the smokers among classmates, tobacco smoke exposure at home, and the negative attitude of the nearest neighbor can represent a protective factor of smoking in the community.
DiscussionFactors that may be associated with adolescent smoking habits were examined on several dimensions. Our study measured several key individual and community indicators hypothesized to be associated with smoking behavior among adolescents, including those related to information, orientation and modeling factors. The results partly support our hypothesis that community activity, smoking among classmates and school performance (motivation for performance) have a high impact on the adolescent smoking.
We found associations between information measures and smoking: the prevalence of smoking is much higher among those who think that smoking is harmless or less harmful. Kaya and Ünalan14 draw the attention to the fact that the beliefs and perceptions of adolescents about smoking should be given as much consideration as the negative effects of cigarettes in planning smoking free messages. Hohman et al.15 assumed that, at the community level, communication comprising anti-smoking messages to which adolescents are receptive may have an important influence on young people's behavior. The importance of awareness is emphasized in other studies also,16,17 confirming that health information represents a protective factor for health behavior.
Adolescent socialization is a significant orientation factor in the development of smoking habits. The integration of the adolescent in his/her community, i.e. the social milieu of the behaviors and values in which the adolescent socializes, leaves its mark on the adolescent's behavior.1
Our results show that the school can be a protective factor only if it is highly rated, it offers quality education and there are clear values and rules that can be followed. As hypothesized, an elevated school performance, will help reduce smoking rates. Our results are congruent with those reported previously showing that school results and teenage smoking status (former or current smoker) are strongly associated.18
In the case of community activity, we focused on activities that appear at the level of the neighborhood: participation in community programs, neighborhood gatherings, joint celebrations, joint entertainment and play. Contrary to our hypothesis, the risk of the adolescent smoking is higher if these types of activities are present in the neighborhood and the adolescent takes part in them, suggesting that the level of community activity itself is not a protective factor against smoking. Similar results were obtained by Pförtner et al,19 confirming that friend-related social capital was significantly associated with a higher likelihood of daily smoking. The time spent with peers will benefit the adolescent provided that the activity has some kind of guidance, such as going to church, and it conveys information about the harmful consequences of smoking. Coleman's findings2 are comparable: social capital is determined by the sense of belonging and it manifests its effects on orientation and behavioral standards. When a community disseminates information through its channels, it attempts to regulate the adolescent behavior by setting clear standards and expectations, by applying sanctions for deviations from norms, and by monitoring how adolescents keep their commitments; these all have an impact on adolescent behavior and promote a healthy socialization.
This study demonstrates that the orientation factors strongly associated with adolescent smoking among Romanian adolescents are: good school results; adult smoking patterns (parents, neighbors); peer smoking patterns; and community activities that not only imply living and having fun together, but also anti-smoking communication. Another important role is played by how much adolescents attach to their home communities and by the type of information they are exposed to about the harmful effects of smoking.
Our findings related to the modeling factor confirm our hypothesis that smoking classmates highly impact teenagers’ behavior. It also suggests that, in general, smoking by friends and attitudes and smoking by adults in the neighborhood are strongly associated with adolescent smoking. Our analysis reveals the perception of adult neighbors’ attitudes toward smoking may serve as a protective factor; i.e., adolescents in neighborhood with a negative attitude towards smoking are less likely to smoke than those whose immediate living environment is permissive or even indifferent about smoking. These results are similar what has been reported by other authors.20–22
One of the limitations of our research is that we did not make a sharp distinction between the individual versus social nature of particular activities, nor did we try to separate activities between youngsters and adults. Certain components of our index, such as cultural activities (like listening to music or regularly going to the theatre) are associated with an increased risk of smoking, as these are social activities undertaken with friends, while activities spent in one's private sphere (like reading a book) are associated with a reduced risk of smoking.
Another limitation of our study is the sample's representativity for Transylvania region only (one of the three main historical regions of Romania), which may narrow the generalizability of our findings.
We should also mention that the validity and reliability of the complete questionnaire have not been checked yet. A potential source of bias is also the self-reported nature of the data; we cannot exclude that the students under-report smoking due to the social desirability or exaggerate the effect of the variable: the negative/prohibiting attitude of the nearest neighbor. In general, the main bias could be that even if teenagers want to appear “desiderable” it is a period of time when they do believe and follow the social norms of their counterparts.
ConclusionsOur results suggest that several social capital factors can play a major role in the adolescent smoking. Although some elements of the social capital do not constitute health risk factors themselves, all may be considered as risk or protective factors, depending on their mode of action and interaction. Our results demonstrate that the organization and development of the community activities aimed at prevention must strengthen the factors mentioned above —information, orientation, modeling— because, through them, the community's social capital will expand and reduce the likelihood of teenage smoking.
Sociocultural environment has an impact on attitudes, values and behaviors. Social capital rules behavior through safe human relationships, information channels, duty and norms. This is a combination of effects that one turns to account depending on how she/he is connected to the community.
What does this study add to the literature?We have developed a model exhibiting the relationship between community capital and adolescent smoking. Consequently, prevention should emphasize the orientation, which means values, attitudes, health awareness, community/social life; the modeling (pro-social behavior models, interpersonal skills, self-determination), as well as the information transfer concerning the effects of smoking. A policy intervention, influencing adolescents’ behaviour serves the community empowerment.
Carlos Álvarez-Dardet.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
DeclarationAll procedures performed in this study were in accordance with the 1964 Declaration of Helsinki and its later amendments. We previously obtained written permission from schools inspectorates, headmasters (school management) and parents for conducting the survey. All parents were informed about the purpose, benefits and risks of the study. Participation in the study was optional.
Authorship contributionsE. Albert-Lorincz designed and planned the study. B. Szabo contributed to the implementation; carried out the statistical analysis and data interpretation. A.I. Gasparik conceived and wrote the final version of the manuscript. E. Paulik was in charge of overall direction of the study. K. Foley supervised the project. All authors were involved in the critical review and have approved the final version of the manuscript for publication.
FundingThe research reported in this publication was supported by the Fogarty International Center and the National Cancer Institute of the National Institutes of Health under Award Number 1 R01 TW09280-01. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Conflicts of interestNone.











