






The 3rd International Nursing and Health Sciences Students and Health Care Professionals Conference (INHSP)
Más datosThis study aimed to analyse the health risks related to the use of chemicals among workers in small footwear factories.
MethodsThis was a descriptive case study conducted in three selected small footwear factories located in Ciomas, Bogor, Indonesia. The assessment was conducted using the chemical health risk assessment method by the Department of Safety and Health Malaysia Year 2018.
ResultsResults showed that the level of risk of chemicals through inhalation fell on the moderate and high-risk categories, indicating that high exposure could lead to carcinogenic effects. Dermal exposure was categorised as moderate risk, causing such health effects as skin and eye irritation.
ConclusionFactory X, Y, and Z have been found to have a significant risk of hazardous chemical exposure (i.e., benzene and toluene), specifically at the glueing stations, either from inhalation or dermal contact.
Small- and medium-sized enterprises (SMEs) play a significant role in providing jobs and economic growth. According to the World Bank, SMEs contribute up to 60% of the total employment and 40% of gross domestic product (GDP).1–3 In Indonesia, SMEs contribute 97.16% to job creation and 58.65% to the national GDP.2 However, despite their economic significance and the number of individuals dependent on them for living, focus on occupational safety and health (OSH) in this sector is poor.3
According to the International Labour Organisation (ILO), work-related diseases inflicted a substantial mortality burden in 2008, and there were 2.02 million deaths caused by work-related diseases and 321,000 by work-related accidents.4,5 The small industry is over-represented in work-related deaths compared to larger enterprises, but under-represented in these organisations’ focus on OSH issues. Accidents are 20% more frequent in the small industry than in larger enterprises with more than 100 workers and 40% more frequent than in enterprises with more than 1000 workers.3,6,7
OSH implementation barriers in small industries include the following: lack of workforce, financial capacity, technological resources, and establishment of OSH committees.5,8–10 They also possess a lower capacity to assess and control risks compared with larger enterprises effectively.11,12
Footwear manufacturing in Indonesia is one of the industrial sectors that have demonstrated a sustainable growth level and is concentrated mainly in a small cottage industry.13 Workers in the footwear manufacturing industry are exposed to an extensive range of hazards such as complex mixtures of organic solvents, which may enter their system through inhalation and dermal routes.13,14
Todd et al. (2008) found an association between exposure to chemical hazards and adverse health outcomes in footwear manufacturing industries exposure.14 Some studies conducted in the footwear manufacturing small Industry in Bogor-Indonesia found that the average benzene and toluene levels were over the threshold limit value (TLV).15–17 The manufacturing process used in the footwear industry uses hazardous chemicals, and the associated risks are poorly managed. OSH risk assessment should be given much more priority in SMEs.18 Therefore, this study analysed the health risks related to the use of chemicals among workers in this sector.
MethodsThe study was a descriptive case study conducted in three selected small footwear factories located in Ciomas, Bogor, Indonesia. The total number of factory X, Y, and Z employees are 13, 12, and 8 workers respectively. Those factories were categorised as small industries according to Indonesian business classification.19 We selected two workers for each factory samples per factory that we determined to represent exposure to the maximum risk employee(s).
This study used the methodology from ‘Assessment of the Health Risks Arising from the Use of Hazardous Chemicals in the Workplace,’ by the Department of Occupational Safety and Health (DOSH) in Malaysia.20 We limited the routes of exposure to inhalation and dermal route. For the inhalation assessment, we conducted personal air sampling using the NIOSH manual of analytical methods 1501.21 The chemicals concerned in this study were benzene and toluene that its vapor concentrations were measured and then compared with the Indonesian occupational exposure limit (OEL), governed by Regulation of Ministry of Labour Number 5 the Year 2018 (TLV-TWA Benzene: 0.5ppm; toluene: 20ppm).22
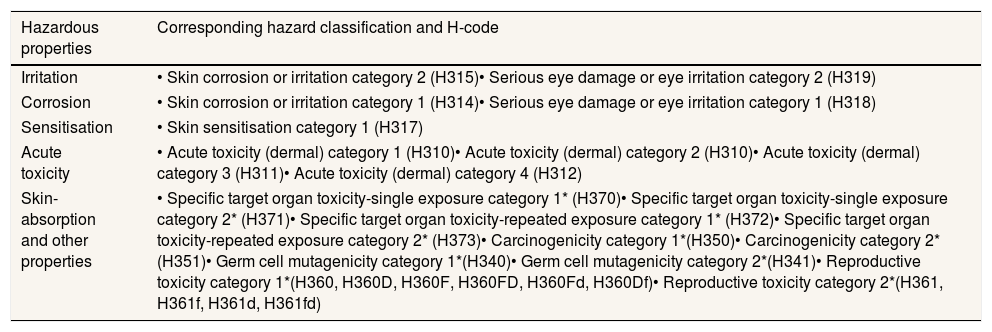
Chemical hazard information was obtained from the European Chemicals Agency (ECHA) to determine the hazard rating (HR) for inhalation and hazardous properties for dermal.23,24 The HR for inhalation is outlined in Table 1. We listed the HR assigned and selected the highest as the HR. The hazardous properties are outlined in Table 2. All the hazard classification of chemicals is following the Globally Harmonized System of Classification and Labelling of Chemicals.25
Hazard rating for inhalation exposure.
| HR | Hazard classification | H-code |
|---|---|---|
| 5 | Acute toxicity category 1 (inhalation) | H330 |
| Carcinogenicity category 1A | H350,H350i | |
| Mutagenicity category 1A | H340 | |
| Reproductive toxicity category 1A | H360,H360D,H360F,H360FD,H360Fd,H360Df | |
| Specific target organ toxicity – single exposure category 1 | H370 | |
| 4 | Acute toxicity category 2 (inhalation) | H330 |
| Carcinogenicity category 1B | H350,H350i | |
| Mutagenicity category 1B | H340 | |
| Reproductive toxicity category 1B | H360,H360D,H360F,H360FD,H360Fd,H360Df | |
| Effects on or via lactation | H362 | |
| Specific target organ toxicity – single exposure category 2 | H371 | |
| Specific target organ toxicity – repeated exposure category 1 | H372 | |
| Respiratory sensitisation category 1 | H334 | |
| 3 | Acute toxicity category 3 (inhalation) | H331 |
| Carcinogenicity category 2 | H351 | |
| Mutagenicity category 2 | H341 | |
| Reproductive toxicity category 2 | H361,H361f,H361d,H361fd | |
| Specific target organ toxicity – repeated exposure category 2 | H373 | |
| Specific target organ toxicity – single exposure category 3 (respiratory tract irritation) | H335 | |
| 2 | Acute toxicity category 4 (inhalation) | H332 |
| Specific target organ toxicity – single exposure category 3 (narcotic effect) | H336 | |
| 1 | Chemical not otherwise classified | H333 |
Hazardous properties relevant to dermal exposure.
| Hazardous properties | Corresponding hazard classification and H-code |
|---|---|
| Irritation | • Skin corrosion or irritation category 2 (H315)• Serious eye damage or eye irritation category 2 (H319) |
| Corrosion | • Skin corrosion or irritation category 1 (H314)• Serious eye damage or eye irritation category 1 (H318) |
| Sensitisation | • Skin sensitisation category 1 (H317) |
| Acute toxicity | • Acute toxicity (dermal) category 1 (H310)• Acute toxicity (dermal) category 2 (H310)• Acute toxicity (dermal) category 3 (H311)• Acute toxicity (dermal) category 4 (H312) |
| Skin-absorption and other properties | • Specific target organ toxicity-single exposure category 1* (H370)• Specific target organ toxicity-single exposure category 2* (H371)• Specific target organ toxicity-repeated exposure category 1* (H372)• Specific target organ toxicity-repeated exposure category 2* (H373)• Carcinogenicity category 1*(H350)• Carcinogenicity category 2*(H351)• Germ cell mutagenicity category 1*(H340)• Germ cell mutagenicity category 2*(H341)• Reproductive toxicity category 1*(H360, H360D, H360F, H360FD, H360Fd, H360Df)• Reproductive toxicity category 2*(H361, H361f, H361d, H361fd) |
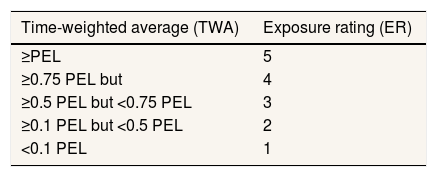
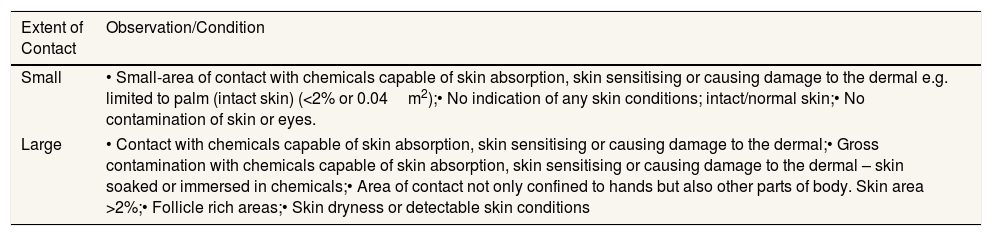
The evaluation for inhalation exposure was conducted quantitatively, while dermal exposure was performed qualitatively. The exposure rating (ER) was determined using the exposure measurement data based on the time-weighted average (TWA) of a typical working day. The ER for inhalation exposure is outlined in Table 3. The qualitative evaluation of dermal exposure was measured by determining the extent of dermal contact (outlined in Table 4) and dermal contact duration, categorised as being above or below 15min per shift.
Extent of dermal contact.
| Extent of Contact | Observation/Condition |
|---|---|
| Small | • Small-area of contact with chemicals capable of skin absorption, skin sensitising or causing damage to the dermal e.g. limited to palm (intact skin) (<2% or 0.04m2);• No indication of any skin conditions; intact/normal skin;• No contamination of skin or eyes. |
| Large | • Contact with chemicals capable of skin absorption, skin sensitising or causing damage to the dermal;• Gross contamination with chemicals capable of skin absorption, skin sensitising or causing damage to the dermal – skin soaked or immersed in chemicals;• Area of contact not only confined to hands but also other parts of body. Skin area >2%;• Follicle rich areas;• Skin dryness or detectable skin conditions |
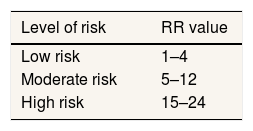
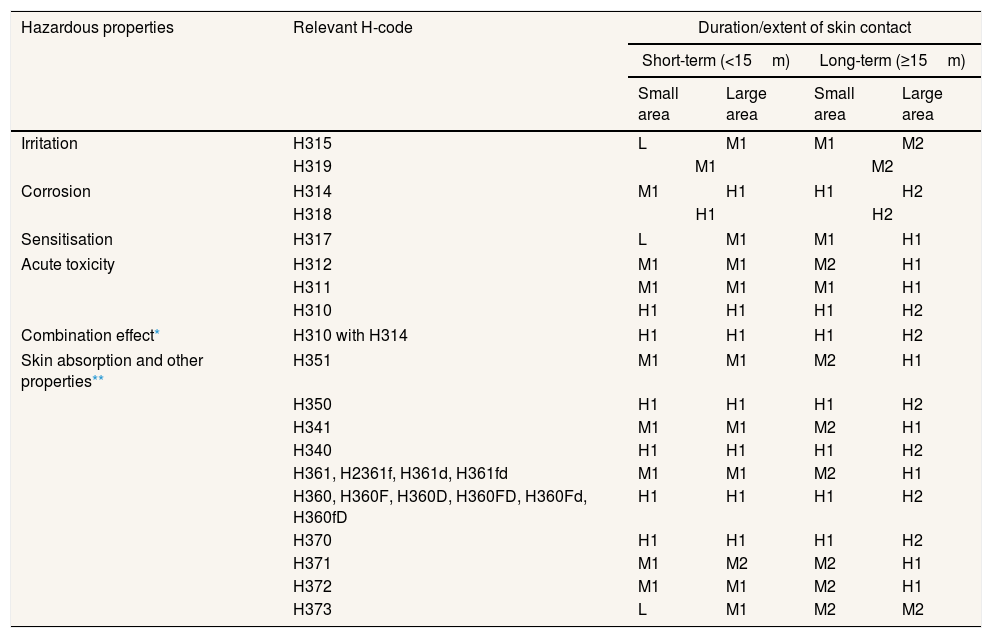
The level of risk for inhalation exposure was based on the risk rating (RR) derived from the HR and ER outlined in Table 5, and that of the level of risk for dermal exposure in Table 6.
Risk matrix for dermal exposure.
| Hazardous properties | Relevant H-code | Duration/extent of skin contact | |||
|---|---|---|---|---|---|
| Short-term (<15m) | Long-term (≥15m) | ||||
| Small area | Large area | Small area | Large area | ||
| Irritation | H315 | L | M1 | M1 | M2 |
| H319 | M1 | M2 | |||
| Corrosion | H314 | M1 | H1 | H1 | H2 |
| H318 | H1 | H2 | |||
| Sensitisation | H317 | L | M1 | M1 | H1 |
| Acute toxicity | H312 | M1 | M1 | M2 | H1 |
| H311 | M1 | M1 | M1 | H1 | |
| H310 | H1 | H1 | H1 | H2 | |
| Combination effect* | H310 with H314 | H1 | H1 | H1 | H2 |
| Skin absorption and other properties** | H351 | M1 | M1 | M2 | H1 |
| H350 | H1 | H1 | H1 | H2 | |
| H341 | M1 | M1 | M2 | H1 | |
| H340 | H1 | H1 | H1 | H2 | |
| H361, H2361f, H361d, H361fd | M1 | M1 | M2 | H1 | |
| H360, H360F, H360D, H360FD, H360Fd, H360fD | H1 | H1 | H1 | H2 | |
| H370 | H1 | H1 | H1 | H2 | |
| H371 | M1 | M2 | M2 | H1 | |
| H372 | M1 | M1 | M2 | H1 | |
| H373 | L | M1 | M2 | M2 | |
L: low risk; M: moderate risk; H: high risk.
Three factories were selected, namely factory X, Y, and Z. Most of the workers was male, ranging from 18 to over 60 years of age and have worked in their respective factories for more than a year. Most of them have worked in the industry throughout their careers and demonstrate a limited educational achievement level.
In the process of hazard identification, walkthrough surveys, and discussions with employees and employers were conducted. In general, footwear manufacturing involves four processes: preparation, stitching, assembling, and finishing. The stitching and assembling process had the most significant risk of occupational chemical exposure. According to the safety data sheet and data from previous studies, the organic solvents that were used for diluting the adhesives in Ciomas footwear small industry contained benzene and toluene.16,17,26
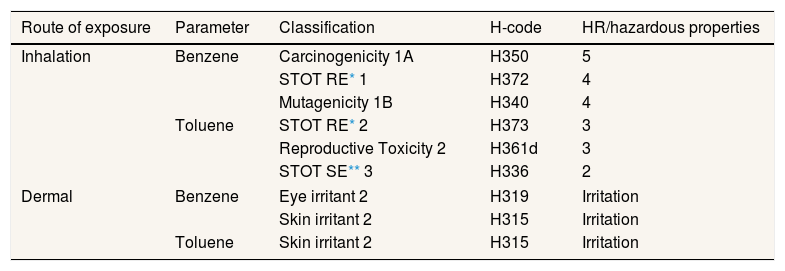
The glue application method increased the likelihood of solvent exposure via inhalation and dermal absorption to the glueing stations’ workers. Since the adhesives need to be heated for curing the glue, the solvent evaporation is accelerated. We also found that the potential of organic vapor exposure was exacerbated by poor ventilation. Wall exhaust fans were used to assist with airflow but were ineffective. Personal protective equipment (PPE) was not provided, and almost all workers applied glue with their bare hands; only a few used a brush or spatula. Taking all these factors into account confirmed that the glueing stations’ workers are exposed to hazardous chemical solvents via both respiratory and dermal routes. In order to assess health risks associated with chemical exposure, the HR and the ER of benzene and toluene were determined. The results for the HR determination are shown in Table 7.
Determination of the HR and hazardous properties.
| Route of exposure | Parameter | Classification | H-code | HR/hazardous properties |
|---|---|---|---|---|
| Inhalation | Benzene | Carcinogenicity 1A | H350 | 5 |
| STOT RE* 1 | H372 | 4 | ||
| Mutagenicity 1B | H340 | 4 | ||
| Toluene | STOT RE* 2 | H373 | 3 | |
| Reproductive Toxicity 2 | H361d | 3 | ||
| STOT SE** 3 | H336 | 2 | ||
| Dermal | Benzene | Eye irritant 2 | H319 | Irritation |
| Skin irritant 2 | H315 | Irritation | ||
| Toluene | Skin irritant 2 | H315 | Irritation | |
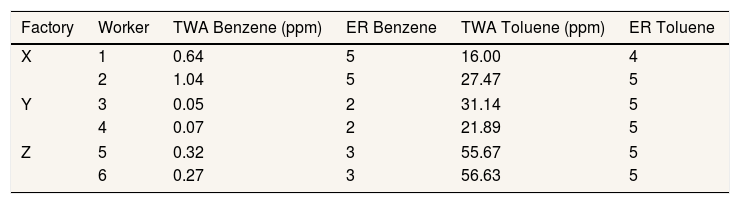
Table 8 shows the TWA value and the ER from the measurement results of benzene and toluene exposure of the six sampled workers.
Table 9 and Table 10 show the results of our CHRA for benzene and toluene.
CHRA for benzene and toluene exposure through dermal.
| Parameter | Classification | Hazardous properties | Exposure | RR | Level of risk | |
|---|---|---|---|---|---|---|
| Duration | Area skin contact | |||||
| Benzene | Eye irritant 2 – H319 | Irritation | Long term | Small | M2 | Moderate |
| Skin irritant 2 - H315 | Irritation | Long term | Small | M1 | Moderate | |
| Toluene | Skin irritant 2 - H315 | Irritation | Long term | Small | M1 | Moderate |
Footwear factories in the sub-district of Ciomas are home-based industries. Previous studies found benzene and toluene are parts of the adhesives and solvents’ ingredients in Ciomas footwear factories, at about 1.34–1.52% for benzene and 73.72–76.79% for toluene.16 In this study, we found that health risks caused by benzene exposure at the glueing stations of factory X and Z were categorised as high risks, while those at factory Y were found to be moderate. Those risks were partially due to benzene's high HR (HR=5) because benzene is confirmed as a carcinogen.16,23,25,27,28 Another factor was the ER of benzene, which were 5 and 3 at factory X and Z, respectively, above the OEL. However, the concentration of benzene at factory Y was lower than in factory X and Z (ER=2). Long-term (≥1 year) exposure to benzene can harm the bone marrow, resulting in anaemia and excessive bleeding.27
On the other hand, toluene is less hazardous than benzene, with lower toxicity (HR=4). Prolonged exposure to toluene can lead to central nervous system damage, sexual function, fertility impairment, and aspiration toxicity.24,29,30 Due to the high exposure level of toluene at the glueing stations of factory X, Y, and Z (ER=4–5), it is categorised as high risk.
Even though factory X, Y, and Z utilise hazardous chemicals in their work processes, we found no separation between hazardous and non-hazardous areas. Therefore, health risks caused by benzene and toluene exposure may also develop to other groups of workers in that factory. Furthermore, there was also a lack of ventilation, OSH awareness, and even PPE. Analogous with our findings, Pastorino et al. (2004) found that small enterprises’ environmental conditions are usually unsatisfactory and caused by the lack of available rooms, safety ranges, fixed pathways, and lighting. Small enterprises generally do not pay much attention to the working conditions at the design stage. Therefore risk controls may be little to none, mostly limited to PPE only.16 Todd et al. (2008) reported that the prevalence of symptoms after being hired was much higher than the prevalence of symptoms before being hired for workers in footwear industries. This result implies that there is an association between exposure to chemical hazards and adverse health outcomes.14
For dermal exposure assessment, according to the Agency for Toxic Substances and Disease Registry (ATSDR), dermal effects, including skin and eye irritation, can occur after benzene exposure. Dermal contact with toluene can cause skin damage because it can remove lipids from the skin. Workers exposed to solvent mixtures, in which toluene is the main component, have been found to have skin problems on their hands. Moreover, eye irritation in humans can occur after exposure to toluene vapor in the workplace.29
Chemical exposure can also come from the hand application of glues to the footwear and equipment pieces as they are assembled.14 Almost all workers in the footwear manufacturing SMEs apply glue with the palms of their bare hands. According to the workers’ interviews, using their hands instead of a brush or spatula was more effective. However, they also admitted that their palms would feel hot when performing the glueing process and sometimes peel off after finishing the process.
ConclusionFactory X, Y, and Z have a significant risk of hazardous chemical exposure (i.e., benzene and toluene), specifically at the glueing stations. The existing control measures at those factories are poorly managed. We found that the health risks from chemical exposure through inhalation are more significant than those from dermal exposure. The level of risk of chemical exposure through inhalation fell under the moderate and high-risk categories. Long-term exposure to benzene may cause cancer and harmful effects on the bone marrow. While, through the dermal route fell under moderate risk, leading to skin and eye irritation.
No effective control measures were found in the workshops. Therefore, we recommend that OSH control measures should be established. Chemical exposure through inhalation can be minimised through proper ventilation, providing workspace separation, and PPE, such as masks. Gloves should be provided to minimise the dermal exposure they would receive. Workers should also be given proper OSH awareness regarding their overall work process.
Conflicts of interestThe authors declare no conflict of interest.
Peer-review under responsibility of the scientific committee of the 3rd International Nursing, Health Science Students & Health Care Professionals Conference. Full-text and the content of it is under responsibility of authors of the article.











