




The aim of this paper was to test the validity and reliability of a Spanish sign language (SSL) adaptation of KIDSCREEN-27, a health-related quality of life (HRQoL) questionnaire for use in deaf children and adolescents.
MethodsWe performed an observational cross-sectional study of 114 deaf children and adolescents aged 8 to 18 years old. The Spanish version of the KIDSCREEN-27 was adapted to SSL through the translation-back translation technique. The adapted questionnaire was then administered using a web tool to ensure complete access to study participants. Floor and ceiling effects were calculated. Structural and cultural validity were tested using exploratory and confirmatory factor analysis. Cronbach's α was used to assess internal consistency. The questionnaire was administered for a second time to the entire sample after 2 to 4 weeks (test-retest reliability).
ResultsIn the SSL version of the KIDSCREEN-27, as in the original Spanish scale, five dimensions explained 59% of the variance. None of the participants obtained the minimum or maximum scores on the scale (floor and ceiling effect, respectively). Confirmatory factor analysis showed the goodness-of-fit of the factor solution with five dimensions of the SSL version. The Cronbach's α of both the total scale and of each of the distinct dimensions was above 0.75. The intra-class correlation coefficient of the test-retest scale was considered acceptable in all the dimensions.
ConclusionsThe reliability and validity of the SSL version of the KIDSCREEN-27 are similar to those of the original Spanish version, providing a new tool for measuring HRQoL in deaf children and adolescents.
Evaluar la validez y la fiabilidad del cuestionario de calidad de vida relacionada con la salud KIDSCREEN-27 traducido a lengua de signos española (LSE) para niños y adolescentes sordos.
MétodoEstudio observacional transversal en el que participaron 114 niños y adolescentes sordos de 8 a 18 años de edad. Utilizando la técnica traducción-retrotraducción se adaptó la versión española del KIDSCREEN-27 a la LSE, y se diseñó una herramienta web para que el cuestionario fuese totalmente accesible. Se calculó el efecto suelo y el efecto techo. La validez estructural y transcultural se comprobó mediante análisis factorial exploratorio y confirmatorio. Para evaluar la consistencia interna se utilizó el coeficiente α de Cronbach. El 100% de la muestra efectuó un retest al cabo de 2-4 semanas (fiabilidad test-retest).
ResultadosEn la versión del KIDSCREEN-27 en LSE subyacían cinco dimensiones que explicaban el 59% de la varianza. Ningún participante obtuvo la puntuación mínima o máxima de la escala (efecto suelo y techo, respectivamente). El análisis factorial confirmatorio mostró la bondad de ajuste de la solución factorial con cinco dimensiones de la versión en LSE. El α de Cronbach tanto de la escala total como de cada dimensión fue superior a 0,75. El coeficiente de correlación intraclase del test-retest fue significativo en todas las dimensiones.
ConclusionesLa versión adaptada a la LSE del KIDSCREEN-27 presentó coeficientes de fiabilidad y validez similares a los de la versión original en español, permitiendo disponer de un nuevo instrumento para medir la calidad de vida relacionada con la salud en niños y adolescentes sordos.
In Spain approximately 25 per 1000 people aged six or more years experience some type of hearing impairment (the term ‘deaf’ is used here to refer to all the degrees of hearing impairment, what means mild, moderate, severe or profound hearing impairment).1 For deaf people to fully achieve their potential, it is necessary to provide the relevant resources to support personal, cognitive, professional, cultural and academic development.2 Technological advances have facilitated access for the people to spoken language, but sign language also has an important role for 120,000 deaf people in Spain.3,4 Sign language serve all practical and theoretical purposes of a natural language, including age appropriate language acquisition in infants and children.2,5–7
In comparison with the hearing population, deaf people have more mental health problems and a generally poorer health-related quality of life (HRQoL). This is mainly due to communication problems,8,9 which lead to higher levels of psychological distress and affect emotional development. However, mental health and quality of life have been not related with the degree of deafness.10
HRQoL in deaf children and adolescents has been mainly used as a measure of effectiveness of cochlear implants. Self-administered instruments such as KINDLR11 and FKSI (Frankfurt Self-Concept Scales for Children),12 among others, have been used for this purpose.
In a recent study 15 generic HRQoL questionnaires which have been adapted or created for children and adolescents in Spain were identified. There is great variability in both the number and characteristics of the dimensions included.13 The KIDSCREEN project (2001-2004), a partnership of 13 European countries, developed a standardized instrument to measure HRQoL in children and adolescents in the trans-cultural field.14 Three versions of the Spanish KIDSCREEN questionnaire were subsequently developed (52, 27 and 10 items respectively). These have proved to have good acceptability, reliability and validity for the general paediatric population (from 8 years) and adolescents (under 18 years).15,16
Studies have shown that the average reading level of deaf people is well below that of the general population.17–19 At least 47% of the deaf population lack any form of basic education or are illiterate. Approximately 92% of the deaf population fails to complete their high school studies and the ones who do are regarded as functional illiterates because they have serious problems to understand written text and to express themselves effectively in writing.20 For this reason, such questionnaires are not appropriate. However, deaf people's ability to understand psychological tests is not affected by this low reading level if they are administered in sign language.21
In an Austrian study, the WHO Quality of Life (WHO-QOL) Questionnaire, 12-item General Health Questionnaire (GHQ-12) and Brief Symptom Inventory (BSI) were adapted to Austrian Sign Language.21 But no HRQoL instrument has been translated and adapted for Spanish deaf children and adolescents. Perhaps this is why the HRQoL of deaf children has not been tested by any study in Spain; this should be a starting point for evaluating any work on this population.
The aim of this study was to adapt the HRQoL instrument KIDSCREEN-27 for children and adolescents between 8 and 18 years old22,23 to Spanish Sign Language (LSE). The LSE version is fully accessible to deaf children and adolescents who use sign language, and can be self-administered. The validation of this instrument will provide insight into the perception of deaf children and young people on their quality of life, while contextualizing the information within national and international settings.
MethodsStudy procedure and subjectsThis study is an observational cross-validation of a HRQoL instrument involving 114 deaf children and adolescents aged 8-to-18 years. All of them completed the questionnaire twice with a 2-4 weeks interval. Participants were recruited from schools, colleges, high schools and associations of deaf people from the Regions of Castilla-La Mancha and Madrid. First we contacted with 79 schools and eight associations in Castilla-La Mancha. For the sake of a greater sample we contacted with seven schools and fourteen associations in Madrid. Finally, 61 schools and three associations of Castilla-La Mancha and four schools of Madrid participated in the study. Our final sample was composed of 75 subjects from Castilla-La Mancha and 39 subjects from Madrid. Fieldwork took place during the 2009-2010 and 2010-2011 school years.
The study protocol was approved by the Clinical Research Ethics Committee of the Virgen de la Luz Hospital in Cuenca, and also had the express support of the Provincial Office of Education in Cuenca and that of the Confederation of Deaf People. A letter was sent to parents informing them about the aims of the study and inviting them to accept the participation of their children by signing an informed consent document. The protocol follows the principles of the Declaration of Helsinki,24 and information management was conducted according to the provisions of the Organic Law of Protection of Personal Data (Law 15/1999)25 and its regulations (RD 1720/2007).26
Variables and measurement instrumentsAs well as socio-demographic variables (age, sex, socioeconomic status), other variables were included: degree of hearing loss, type of deafness (congenital or acquired), time of onset of deafness (pre-lingual or post-lingual), preferred form of communication (sign language or spoken language), functionality of communication, communication problems, parental responsibilities and expectations of the deaf child's development, parental acceptance of the child's deafness, and education (mainstream or special school). HRQoL responses were obtained by self-administered versions of the KIDSCREEN-27 for children and adolescents adapted and translated into LSE.
The KIDSCREEN-27 questionnaire consisted of 27 items which are used to assess HRQoL across five dimensions: physical well-being (five items); psychological well-being (seven items); autonomy and parents (seven items); peers and social support (four items); and school environment (four items). The items assess either the frequency of behaviour/feelings or, in fewer cases, the intensity of an attitude and are answered on a five-point scale with a timeframe of one week. Higher scores indicate better HRQoL.27
Adaptation of the KIDSCREEN-27 to the LSEBecause many deaf children have difficulties with reading, the children's version of the KIDSCREEN-27 was translated and adapted into LSE.22 So that this could be self- administered and have utility for other professionals or other Spanish-speaking communities who use LSE. In addition, a web tool was designed in LSE for the questionnaire (http://www.cess.uclm.es/qd/) so that it is fully accessible to deaf children and adolescents who are users of this language.
Since we did not have a sufficient number of the sample's families with deafness to validate an adapted the adult version of the instrument, we have only adapted the children's version of the KIDSCREEN-27.
Translation-back translation of the questionnaireBack translation was used in order to ensure cultural alignment of the original (written Spanish) and new (LSE) versions. Three bilingual deaf adults (Spanish and LSE) with high levels of reading skills took part in the translation of the Spanish questionnaire to LSE (and the subsequent preparation of the carrier medium). They were supplied with a Spanish version of the KIDSCREEN-27 children and were asked to translate each item into LSE. Working alongside an LSE interpreter, a consensus was reached on the best version of each item and the first recording of the survey was made.
The visual material was delivered to another LSE interpreter and to a post-lingually deaf bilingual who had not taken part in the translation of the written version to LSE. They translated independently each item from LSE to written Spanish. The back-translations were then compared with the original Spanish written version to assess the degree of concordance.
In this first revision of the original instrument and of the translation to LSE, some items with unclear meaning (i.e. “Have you been in a good mood?”, “Have you been happy with the way you are?”, among others) were identified, and possible alternatives were discussed. These items were then reassessed by a bilingual deaf person and discussed with the interpreter who had taken part in the first adaptation. A second translation was then created by them with special emphasis on clarifying the ambiguous items. A second back-translation was then prepared by two additional translators: one was deaf, and one with a moderate hearing loss; both were bilingual and with a high level of reading skill.
Finally, a group of LSE experts and deaf people met in order to select the final LSE version of each item for video-recording. There were two signers for the video: a female Spanish/LSE interpreter and a hearing young male, whose father was deaf and who was bilingual in LSE and Spanish.
The software for delivering the questionnaire was specially developed to meet the characteristics and needs of deaf people. In order to enable the questionnaire to be self-administered, written Spanish and LSE are displayed for both the questions and the response options, and it is possible to reply the LSE video clips before responding. Each answer choice is marked with a colored dot as a visual aid for deaf children.21,28 Responses are completed on a paper version of the questionnaire, and the respondent answers each item before moving to the next.
Statistical analysisA descriptive analysis of the sample characteristics was performed, the floor and ceiling effects (proportion of cases obtaining the minimum and maximum scores respectively) were calculated; and the overall score and scores for each of the dimensions were also calculated according to the KIDSCREEN-27 questionnaire instructions.
An exploratory factor analysis (EFA; main components analysis) was conducted to check if the dimension factor was saturated by each item in order to ensure that it constituted a valid indicator. The Kaiser-Meyer-Olkin (KMO) test and Bartlett's sphericity test were also used to assess whether the factor analysis was appropriate to test the scale structure. A factor analysis would be appropriate if the KMO test reaches values above 0.5 and the Barlett test obtains values lower than 0.05.
The adequacy of the LSE-adapted KIDSCREEN-27 was assessed by means of confirmatory factor analysis (CFA) using IBM SPSS Amos 19 software.29 The adjustment of the model was analyzed in various ways. A chi-square (χ2) was used to assess the fit to the data of the sample. The goodness of fit was analyzed using the criteria of Hu and Bentler,30 including the comparative fit index (CFI) and standardized root mean square residual (SRMR).
An analysis of multiple groups was performed to examine gender differences. A χ2 test of differences was used to determine whether differences in the factor loadings were statistically significant.
To test the factor structure of the KIDSCREEN-27, the sample was divided into two subsamples and EFA and CFA were conducted using these two sub-samples respectively.
The internal consistency of the scale was analyzed using Cronbach's alpha coefficient for both the total scale and for each dimension.
For the test-retest reliability the deaf children completed the questionnaire twice with a 2-4 weeks interval. This time gap was selected as it was considered long enough to ensure that participants would not remember their responses and that it was short enough to avoid significant changes in the quality of the participants’ lives.
The intra-class correlation coefficient (ICC) was used to estimate the correlation between baseline scores on the questionnaire and the scoring of their responses 2-4 weeks later.
Except for CFA analyses were performed with IBM SPSS Statistics 19 software.
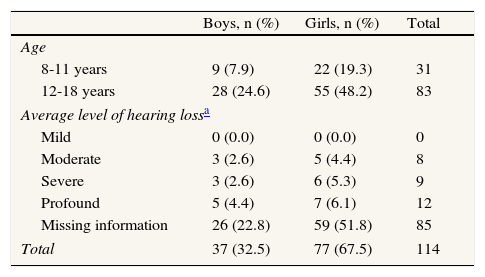
ResultsThe final sample comprised 114 deaf children and adolescents aged 8-to-18 years, of whom 77 (67.54%) were girls. Most of them (74’5%) did not provide information about his/her level of hearing loss (Table 1).
Sample characteristics by degree of deafness, age group and gender (n=114).
| Boys, n (%) | Girls, n (%) | Total | |
| Age | |||
| 8-11 years | 9 (7.9) | 22 (19.3) | 31 |
| 12-18 years | 28 (24.6) | 55 (48.2) | 83 |
| Average level of hearing lossa | |||
| Mild | 0 (0.0) | 0 (0.0) | 0 |
| Moderate | 3 (2.6) | 5 (4.4) | 8 |
| Severe | 3 (2.6) | 6 (5.3) | 9 |
| Profound | 5 (4.4) | 7 (6.1) | 12 |
| Missing information | 26 (22.8) | 59 (51.8) | 85 |
| Total | 37 (32.5) | 77 (67.5) | 114 |
Approximately half of the sample was signer, thus they used the computer version (the web tool) of the questionnaire in LSE. In both cases, those who prefer LSE version and those who prefer in paper form the questionnaire was self-administered.
No participants obtained the minimum or maximum scores on the scale (floor and ceiling effect, respectively).
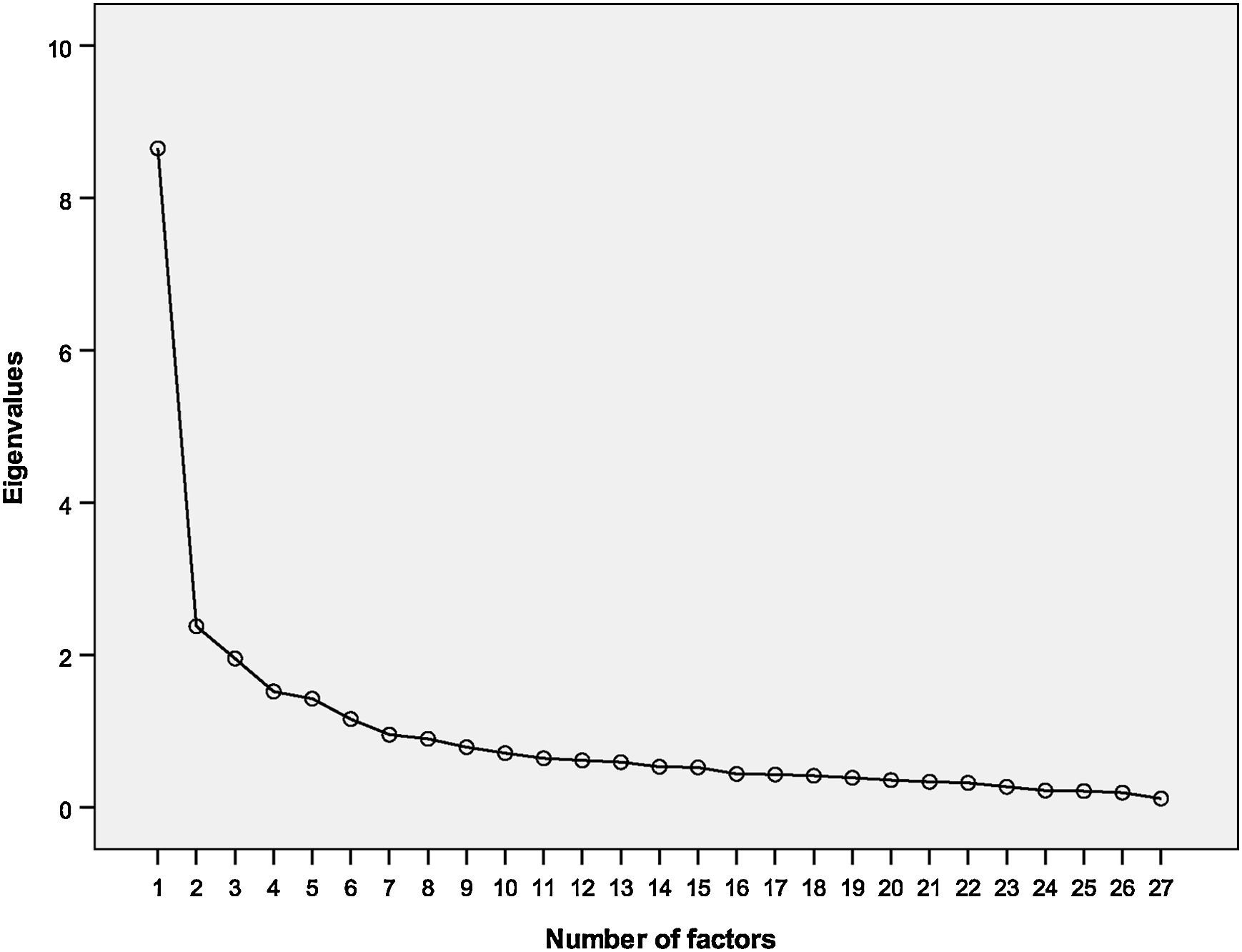
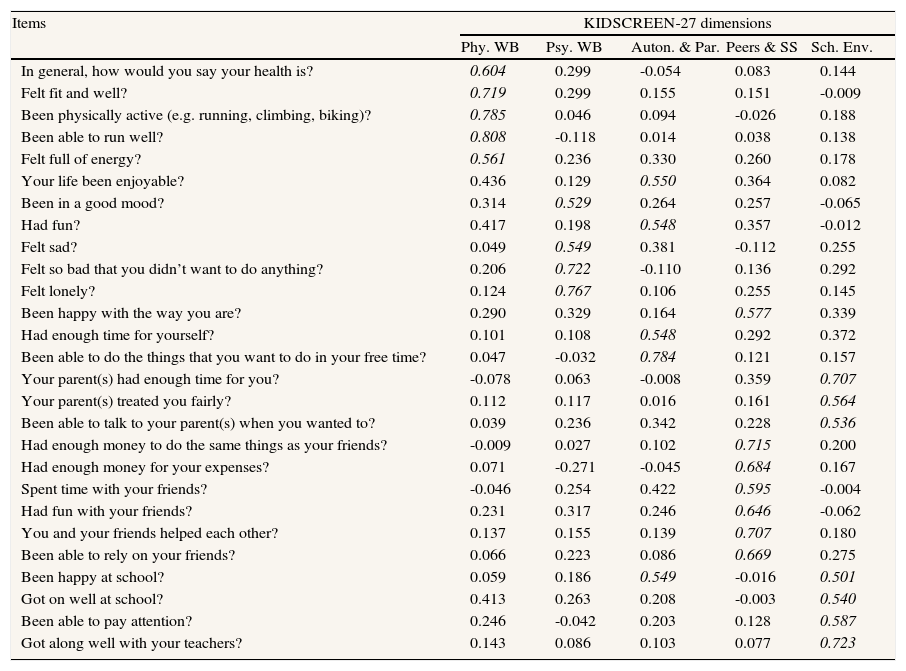
Exploratory factor analysisAn exploratory analysis identified six factors with an eigenvalue greater than 1, but in the screen plot it was observed that a solution with five factors would be appropriate (Fig. 1). This five-factor solution showed good sampling adequacy indexes (Kaiser-Meyer-Olkin 0.822; Barlett sphericity p<0.001), explained 59% of the variance, and was more comparable to the analysis of the original Spanish version. Some differences between the original Spanish KIDSCREEN-27 and the LSE version in the allocation of items after Varimax rotation were observed (Table 2).

Exploratory factor analyses: factor loadings after varimax rotation of KIDSCREEN-27 LSE version.
| Items | KIDSCREEN-27 dimensions | ||||
| Phy. WB | Psy. WB | Auton. & Par. | Peers & SS | Sch. Env. | |
| In general, how would you say your health is? | 0.604 | 0.299 | -0.054 | 0.083 | 0.144 |
| Felt fit and well? | 0.719 | 0.299 | 0.155 | 0.151 | -0.009 |
| Been physically active (e.g. running, climbing, biking)? | 0.785 | 0.046 | 0.094 | -0.026 | 0.188 |
| Been able to run well? | 0.808 | -0.118 | 0.014 | 0.038 | 0.138 |
| Felt full of energy? | 0.561 | 0.236 | 0.330 | 0.260 | 0.178 |
| Your life been enjoyable? | 0.436 | 0.129 | 0.550 | 0.364 | 0.082 |
| Been in a good mood? | 0.314 | 0.529 | 0.264 | 0.257 | -0.065 |
| Had fun? | 0.417 | 0.198 | 0.548 | 0.357 | -0.012 |
| Felt sad? | 0.049 | 0.549 | 0.381 | -0.112 | 0.255 |
| Felt so bad that you didn’t want to do anything? | 0.206 | 0.722 | -0.110 | 0.136 | 0.292 |
| Felt lonely? | 0.124 | 0.767 | 0.106 | 0.255 | 0.145 |
| Been happy with the way you are? | 0.290 | 0.329 | 0.164 | 0.577 | 0.339 |
| Had enough time for yourself? | 0.101 | 0.108 | 0.548 | 0.292 | 0.372 |
| Been able to do the things that you want to do in your free time? | 0.047 | -0.032 | 0.784 | 0.121 | 0.157 |
| Your parent(s) had enough time for you? | -0.078 | 0.063 | -0.008 | 0.359 | 0.707 |
| Your parent(s) treated you fairly? | 0.112 | 0.117 | 0.016 | 0.161 | 0.564 |
| Been able to talk to your parent(s) when you wanted to? | 0.039 | 0.236 | 0.342 | 0.228 | 0.536 |
| Had enough money to do the same things as your friends? | -0.009 | 0.027 | 0.102 | 0.715 | 0.200 |
| Had enough money for your expenses? | 0.071 | -0.271 | -0.045 | 0.684 | 0.167 |
| Spent time with your friends? | -0.046 | 0.254 | 0.422 | 0.595 | -0.004 |
| Had fun with your friends? | 0.231 | 0.317 | 0.246 | 0.646 | -0.062 |
| You and your friends helped each other? | 0.137 | 0.155 | 0.139 | 0.707 | 0.180 |
| Been able to rely on your friends? | 0.066 | 0.223 | 0.086 | 0.669 | 0.275 |
| Been happy at school? | 0.059 | 0.186 | 0.549 | -0.016 | 0.501 |
| Got on well at school? | 0.413 | 0.263 | 0.208 | -0.003 | 0.540 |
| Been able to pay attention? | 0.246 | -0.042 | 0.203 | 0.128 | 0.587 |
| Got along well with your teachers? | 0.143 | 0.086 | 0.103 | 0.077 | 0.723 |
In italics: factor loadings>0.50.
Phy. WB: physical well-being; Psy. WB: psychological well-being; Auton. & Par.: autonomy and parents; Peers & SS: peers and social support; Sch. Env.: school environment.
The factorial structure of the LSE version with the items arranged in the same way than the original Spanish version was tested by CFA. A five-factor model showed acceptable goodness of fit (χ2=551.8; CFI=0.808; normal fit index [NFI]=0.648; p=0.0001; SRMR=0.0832; root mean square error of approximation [RMSEA]=0.082) (Fig. 2). The model displayed good fit by sex and the factor loadings showed no differences between males and females (χ2 DIFF=1218 – 1195=23, df DIFF=650 – 628=22, p=0.29).
Internal consistency/reliability analysis
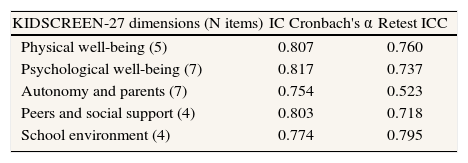
The Cronbach's α coefficient for the KIDSCREEN-27 LSE version was 0.819, and did not increase with elimination of any of the items. This coefficient was higher than 0.75 in all dimensions. ICC for test-retest analysis of the different KIDSCREEN-27 dimensions in the LSE version ranged from 0.523 (Autonomy & Parents) to 0.795 (School Environment) (Table 3).
Internal consistency and retest reliability analysis of the KIDSCREEN-27 LSE version.
| KIDSCREEN-27 dimensions (N items) | IC Cronbach's α | Retest ICC |
| Physical well-being (5) | 0.807 | 0.760 |
| Psychological well-being (7) | 0.817 | 0.737 |
| Autonomy and parents (7) | 0.754 | 0.523 |
| Peers and social support (4) | 0.803 | 0.718 |
| School environment (4) | 0.774 | 0.795 |
IC: internal consistency; ICC: intra-class correlation coefficient.
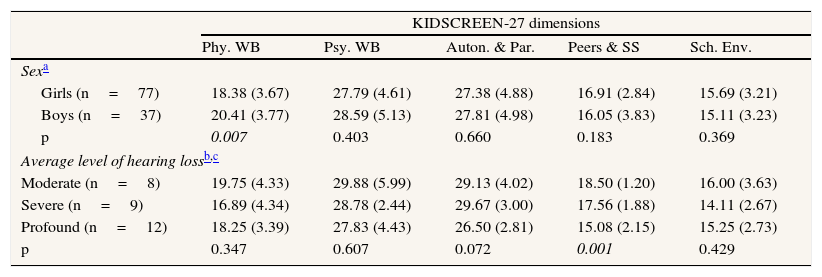
Table 4 show the mean scores of the KIDSCREEN-27 dimensions in the LSE version, by sex, and by level of hearing loss. Boys scored higher than girls in the Physical Well-Being dimension, and not significant differences by sex were found in the other dimensions. On the other hand, Peers and Social Support was the only dimension that showed differences by level of hearing loss.
Mean (standard deviation) of the dimensions of KIDSCREEN-27 LSE version, by sex, and by level of hearing loss.
| KIDSCREEN-27 dimensions | |||||
| Phy. WB | Psy. WB | Auton. & Par. | Peers & SS | Sch. Env. | |
| Sexa | |||||
| Girls (n=77) | 18.38 (3.67) | 27.79 (4.61) | 27.38 (4.88) | 16.91 (2.84) | 15.69 (3.21) |
| Boys (n=37) | 20.41 (3.77) | 28.59 (5.13) | 27.81 (4.98) | 16.05 (3.83) | 15.11 (3.23) |
| p | 0.007 | 0.403 | 0.660 | 0.183 | 0.369 |
| Average level of hearing lossb,c | |||||
| Moderate (n=8) | 19.75 (4.33) | 29.88 (5.99) | 29.13 (4.02) | 18.50 (1.20) | 16.00 (3.63) |
| Severe (n=9) | 16.89 (4.34) | 28.78 (2.44) | 29.67 (3.00) | 17.56 (1.88) | 14.11 (2.67) |
| Profound (n=12) | 18.25 (3.39) | 27.83 (4.43) | 26.50 (2.81) | 15.08 (2.15) | 15.25 (2.73) |
| p | 0.347 | 0.607 | 0.072 | 0.001 | 0.429 |
Phy. WB: physical well-being; Psy. WB: psychological well-being; Auton. & Par.: autonomy and parents; Peers & SS: peers and social support; Sch. Env.: school environment.
p: differences in mean and standard deviation, by sex, and by level of hearing loss (in italics differences statistically significant).
This is the first study to validate a sign language version of a HRQoL questionnaire adapted to a population from 8-to-18 years with hearing impairment. The LSE version of the KIDSCREEN-27 contributes to avoid the problems of limited written language skills so common in this population. We have also developed a web tool to make it possible for the questionnaire to be self-administered and accessible to deaf children and adolescents whose preferred LSE.
The KIDSCREEN-27 is one of the few instruments measuring HRQoL in children and adolescents whose validity has been proven in most of European languages, ensuring cross-cultural equivalence.27,31 The results of our study confirm that the LSE version of the KIDSCREEN-27 shows good psychometric properties and an acceptable level of validity and reliability in deaf children and adolescents.
Behind the 27 items of the KIDSCREEEN-27 in LSE, as in the original Spanish version, were identified five dimensions, although the assignment of items to the different dimensions is not identical in the two versions. Similar observations have been made in adaptations of the questionnaire to other Spanish-speaking countries.32
In general, the factor structure of the KIDSCREEN-27 in LSE confirms the theoretical model of the original Spanish version.23 Although eight items were allocated to different dimensions in the EFA (Table 2), analysis procedures (i.e. rotation technique) could be behind these differences in the items arrangement between both the original Spanish and the LSE scales. When we tested by CFA the five factors model with the same items distribution than in the original Spanish version, the model showed an acceptable goodness of fit. Thus we decided to preserve the same structure than the original Spanish version for the sake of improved comparability.
The KIDSCREEN-27 in LSE has been designed specifically to meet the information and communication needs of deaf children and adolescents (http://www.cess.uclm.es/qd/).21,28 Thus, our study together with a small number of others,21 has begun to fill a gap both nationally and internationally, in terms of adaptation of psychometric tests for the population with hearing impairment.
Another new aspect of our work is the use of technical translation/back translation in sign language. This is the first time such a technique has been used for translations from Spanish to LSE. This technique allowed us to ensure comparability of the KIDSCREEN-27 in Spanish and LSE versions, so that the versions share content and structure.
Overall, participants with moderate level of hearing impairment scored higher in all of the dimensions of the KIDSCREEN-27 in LSE version (Table 4), but these differences were statistically significant only in Peers and Social Support dimension. Some studies have reported no differences in the social relationships area between people with and without hearing impairment33, and only hard of hearing people tend to have more restricted social lives than those with complete prelingual deafness (people who are born deaf or lose their sense of hearing before acquiring speech).34 On the other hand, in our study, according with the results from a cross-cultural survey in 13 European countries of the KIDSCREEN-27,31 boys scored greater than girls in Physical Well-Being dimension, and not differences were found in the other dimensions.
The main limitation of our study was the small sample size, particularly when we tested differences among categories of hearing impairment. Furthermore, even though we had requested information about participants’ level of hearing loss, only a few of them provided us this information. Therefore, we were unable to describe some group comparisons. However, the sample size was large enough to the validation analysis.
Since we did not get the individualized data about how the questionnaire was administered (web tool or writing down on paper), we could not analyze the differences between both groups, although we are aware about that the self-ratings might be influenced by the way of administration.
Our study has only adapted the children's version of the KIDSCREEN-27. The parent's version has not been adapted to LSE since, as is the case in general,20 most deaf children's parents were hearing, and we would not have a sufficient number of families to validate and adapted the adult version of the instrument.
We believe the KIDSCREEN-27 in LSE will provide a valid and reliable instrument to measure the impact of deafness on HRQoL in children and adolescents, and will serve as an outcome measure in intervention studies in which HRQoL is one of the objectives.
- •
Deaf people have limited or no reading skills, thus self-administered questionnaires in written language are not suitable for them. However, they can understand psychological tests if they are administered in sign language. No health-related quality of life (HRQoL) instrument has been translated and adapted for Spanish deaf children and adolescents, neither the HRQoL of this population has been tested by any study in Spain.
- •
This is the first study to validate a sign language version of a HRQoL questionnaire adapted to a population from 8 to 18 years with hearing impairment. The KIDSCREEN-27 in Spanish Sign Language will provide a valid and reliable instrument to measure the impact of deafness on HRQoL in children and adolescents, and will serve for intervention studies including HRQoL as an outcome measure.
M.J. Pardo-Guijarro and V. Martínez-Vizcaíno devised and coordinated the project, and assisted in data acquisition and interpretation. P. Moya-Martínez contributed in the design of the web tool. M. Martínez-Andrés contributed in the field work and revised the manuscript. B. Woll and E.E. Cortés-Ramírez advised the team in all the stages. All authors contributed ideas, reviewed drafts of the manuscript, contributed to drafting and approved the final version. M.J. Pardo-Guijarro and V. Martínez-Vizcaíno had full access to all of the data in the study and they are the responsible for the integrity of the data and the accuracy of the data analysis, and will act as guarantors.
FundingHealth and Social Research Centre, University of Castilla-La Mancha, Cuenca, Spain.
Conflicts of interestNone.
The authors wish to thank the various centers (local education authorities, schools, high schools, National Confederation of Deaf People [CNSE], federations and associations of deaf people, and federations and associations of parents and friends of deaf children) for their contribution and involvement in this project. We also thank all the deaf children and adolescents and their families who participated in the study for their generous collaboration.











