



The 1st International Conference on Safety and Public Health
More infoClean and healthy living behavior (CHLB) habituation in elementary-school-age children can be influenced by a variety of factors, including exposure to health-promoting media, parents’ and teachers’ roles in children's CHLB.
MethodThis research was conducted from February through August of 2019 at all elementary schools in the northern area of Kramatwatu District, with a sample of 170 fifth graders enrolled by the purposive sampling technique. This research employed a cross-sectional design with a bivariate analysis.
ResultsResults showed that 45.3% of the respondents possessed good CHLB. There were significant relationships of exposure to health-promoting media, parents’ role, teachers’ role to CHLB in fifth graders.
ConclusionsFacility and infrastructure availability becomes a driving factor in behavioral change.
Clean and healthy living behavior (CHLB) instillment at school must start from the elementary school level given that elementary school years constitute a golden period for inculcating clean and healthy behavior. Another reason for which instilling CHLB in elementary school becomes essential is that because elementary school age is the age of agent of change.1 Not only are they highly sensitive to behavioral change, children of elementary school age can also act as health promoters for their parents and society.1 Habituation of clean and healthy living behavior since early ages, in particular the school age, will produce a behavioral change that tends to settle.
Aside from being agents of change, elementary-school-age children are also an age group highly susceptible to transmission of diseases, particularly those transmitted through poor clean living behavior like URTI (upper respiratory tract infection), diarrhea, and intestinal worm infection. Intestinal worm infection is one of the most common infections affecting elementary school students. In support of this finding, Lubis also stated that 40–60% of school-age children are with intestinal worms.2 Diarrhea is another frequent disease in school-age children. It is recorded by the World Health Organization (WHO) that, per annum, 100,000 Indonesian children die from diarrhea. Out of a nationally estimated of 6,897,467 diarrheal cases found at health facilities in Indonesia in 2016, only 2,544,084 (36.9%) received treatment.3
Such behavior-based disease rate of incidence can be attributed to wide-ranging factors, including availability of health-promoting media at school, teachers’ role, and parents’ role. As pointed out in Lina's study, the CHLB indicators least exhibited by students were buying food and beverages from the school canteen, having the body weight and height measured, eradicating mosquito larvae at school, and using the toilet facility at school.4 An extra factor influencing elementary school students’ CHLB is the role of the parents and the teachers. Parents and teachers attend children when performing their daily life activities. The role of the parents and the teachers are predominant and determinant of the children's quality of life in the future. Parents are a reference for children at home, while teachers are role models at school. Research results indicated that there was a significant relationship between teachers’ knowledge and role and implementation of CHLB programs for elementary school students.5 There was also a significant relationship, as stated by Nasiatin, between the roles of teachers, parents, with CHLB practices.6 Students whose parents performed their role well demonstrated a higher percentage in showcasing CHLB than did those whose parents performed their role poorly.7
Kramatwatu District, one of the districts in the Province of Banten, has 31 elementary schools across its area, consisting of 21 schools in the north and 10 in the south. A study at the elementary schools in Kramatwatu District showed that 32% of the respondents had poor CHLB and that 35.5% of the elementary schools revealed no health-promoting media were in place.8 On account of the above mentioned, the authors were interested in conducting an analysis of the factors linked to CHLB in fifth graders in Kramatwatu District in 2019. This research aimed at figuring out what factors were related to CHLB in elementary school students in Kramatwatu District in 2019.
MethodThis research employed a cross-sectional research design with the independent variables exposure to health-promoting media, parents’ role, teachers’ role, and the dependent variable CHLB being observed simultaneously.
The present research was conducted at all elementary schools in the northern part of Kramatwatu District (21 elementary schools) from February through August of 2019. The population of this research was comprised of 1,729 grade 5 elementary school students. A sample of 170 fifth graders was purposively extracted based on the grand sampling formula for cross-sectional research. The data required in this research consisted of primary from the respondents using questionnaires, interviews with elementary school students.
The questionnaire contains questions about clean and healthy living behavior, exposure to health-promoting media, teachers’role, parents’ role, are self-developed by researchers and the variables tested for validity are the teacher's role and parent's role variables. The test results showed that 16 questions about the teacher's role that were declared valid and reliable were 11 questions and from 12 questions about the role of parents who were declared valid and reliable as many as 8 questions. The validity test uses as many as 50 elementary students as respondents. Data analysis was performed univariately and bivariate using the Chi-square test at a significance level α (alpha)=5% and 95% confidence interval.
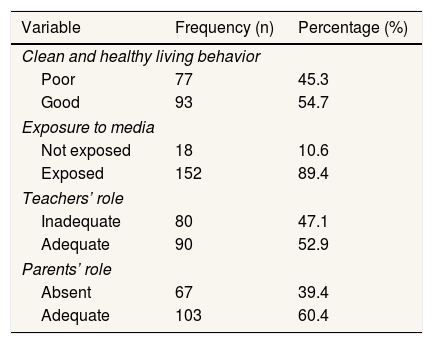
ResultsBased on Table 1, 45.3% of the respondents had good CHLB, 89.4% of the respondents stated they were exposed to CHLB-related media, 52.9% of the teachers performed their role adequately and 60.4% of the parents performed their role adequately.
Research variables’ frequency distribution.
| Variable | Frequency (n) | Percentage (%) |
|---|---|---|
| Clean and healthy living behavior | ||
| Poor | 77 | 45.3 |
| Good | 93 | 54.7 |
| Exposure to media | ||
| Not exposed | 18 | 10.6 |
| Exposed | 152 | 89.4 |
| Teachers’ role | ||
| Inadequate | 80 | 47.1 |
| Adequate | 90 | 52.9 |
| Parents’ role | ||
| Absent | 67 | 39.4 |
| Adequate | 103 | 60.4 |
Source: Primary Data, 2019.
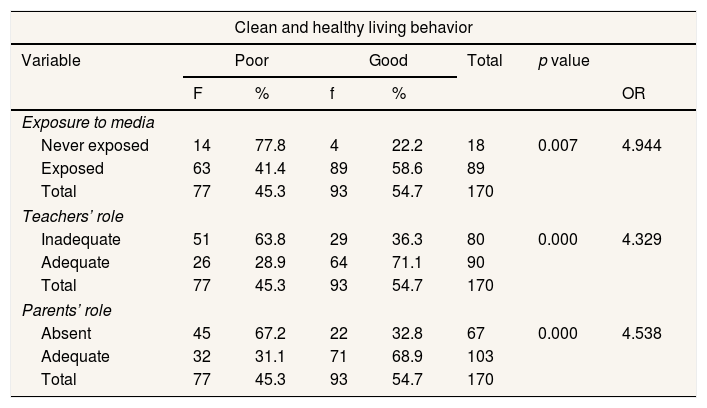
Based on Table 2, there were significant relationships of exposure to health-promoting media, parents’ role and teachers’ role to CHLB in fifth graders.
Analysis of clean and healthy living behavior in fifth graders.
| Clean and healthy living behavior | |||||||
|---|---|---|---|---|---|---|---|
| Variable | Poor | Good | Total | p value | |||
| F | % | f | % | OR | |||
| Exposure to media | |||||||
| Never exposed | 14 | 77.8 | 4 | 22.2 | 18 | 0.007 | 4.944 |
| Exposed | 63 | 41.4 | 89 | 58.6 | 89 | ||
| Total | 77 | 45.3 | 93 | 54.7 | 170 | ||
| Teachers’ role | |||||||
| Inadequate | 51 | 63.8 | 29 | 36.3 | 80 | 0.000 | 4.329 |
| Adequate | 26 | 28.9 | 64 | 71.1 | 90 | ||
| Total | 77 | 45.3 | 93 | 54.7 | 170 | ||
| Parents’ role | |||||||
| Absent | 45 | 67.2 | 22 | 32.8 | 67 | 0.000 | 4.538 |
| Adequate | 32 | 31.1 | 71 | 68.9 | 103 | ||
| Total | 77 | 45.3 | 93 | 54.7 | 170 | ||
Source: Primary Data, 2019.
OR: odds ratio.
CHLB is a behavior resulted from learning and practiced voluntarily for the realization of maximum degree of health. It is developed in all settings, including the educational one. CHLB in school-age children is the most effective way of health promotion and education given that these children are agents of change who are highly sensitive to any form of change. As suggested by the research results, 45.3% of the respondents demonstrated poor CHLB, a proportion approaching that of respondents who showed the otherwise (54.7%). This is consistent with the finding of previous research which shows nearly balanced proportions of good and poor CHLB in students.9 If we are to refer to the CHLB indicators in school settings, there were some that fell short of the requirement. The highest-percentage poor CHLB found in this research was body weight and height measurement. The healthy snacking behavior also fell into the poor category. The behavior in the indicator of school toilet for defecating and urinating was also still categorized as poor. These results are in line with those of previous study, in which the handwashing behavior indicator was categorized as adequate, healthy snacking, no-smoking indicator and no-littering as poor.10
Media refer to the tools used as channels to deliver health messages and to facilitate the messages receipt by the community or clients,11 that can take either print or electronic forms. It is instrumental that the CHLB media employed to promote health must use simple, concise, easy-to-understand, interesting language to the readers/audiences. According to the research results, most of the respondents (89.4%) conveyed to have ever been exposed to CHLB. The percentage of respondents exposed to CHLB media and demonstrating good behavior was higher than those demonstrating poor behavior and so were those who had never been exposed to CHLB media.
The results also showed that the respondents with zero exposure were at five times higher risk for poor CHLB than exposed respondents. This finding is in line with that of Hanif et al. (2019), stating that print media (CHLB pocketbook) was effective in improving knowledge of, attitude toward, and intention for CHLB.12 Elementary school students gain information on CHLB from a variety of media, including newspapers, television, radio, books and magazines at school, books and magazines at home, the Internet, parents, and teachers. The research results demonstrated that the elementary school students obtained CHLB information mostly from parents (81.2%), teachers (80.6%), and books and magazines at school (71.2%). This suggests that the students at school received the most exposure to CHLB from parents and schools. It is thus essential that the school increases the availability of CHLB-related health-promoting media.
The promotion of CHLB can also be performed by Course Review Horay method, by which a cheerful, fun atmosphere is created. Research results showed that this method of Course Review Horay was able to improve the knowledge, attitude, and practice of school-age students in relation to CHLB.13,14 Besides, health socialization can also serve as an alternative for delivering health messages. It has been proven effective in improving one of the indicators of CHLB at school, that socialization activitiy significantly impacted on the increase in body weight, body height, and nutritional status of elementary school students.15
In this research, teachers’ role encompassed providing health information and socialization, teaching, planning, making referrals, and reprimanding students. Based on the research results, the respondents stating the teachers performed their role inadequately were at four times higher risk for poor CHLB than those stating the teachers performed their role adequately. This finding is supported by research, which, too, stated that teachers’ role was related to students’ CHLB.16 Based on the results, the piece of information predominantly given by the teachers to the students at school was that on CHLB. According to such results, it became obvious that the teachers’ role which was still lacking was the one in confiscating cigarettes at school. Confiscation is seen as necessary by the teachers as an anticipative effort to prevent the increase in smoking prevalence among school-age students.
Parents have a role in education, including being role models, providing advice, and reminding children to always maintain their personal cleanliness. It is also helpful for the parents to stress the importance of CHLB for the children. The percentage of respondents demonstrating good CHLB was higher in those who stated parents’ adequate performance of role in the children's CHLB. This is consistent with the previous research which stated that parents’ role was related to students’ CHLB.7,17 This shows that health education should first and foremost be provided by parents as parents are the first and foremost party with a pivotal role in giving shape to children's behavior.
ConclusionsFacility and infrastructure availability becomes a driving factor in behavioral change.
Conflicts of interestThe authors declare that they have no conflict of interest.
Peer-review under responsibility of the scientific committee of the 1st International Conference on Safety and Public Health (ICOS-PH 2020). Full-text and the content of it is under responsibility of authors of the article.











