



The 3rd International Nursing and Health Sciences Students and Health Care Professionals Conference (INHSP)
More infoThis study aims to determine the relationship between estradiol hormone levels and duration of the usage on sexual dysfunction in Depo Medroxy Progesterone Acetate acceptors.
MethodFamily Planning (KB/Keluarga Berencana) Depo Medroxy Progesterone Acetate as many as 43 respondents who meet the sample criteria. The sampling technique used was accidental sampling. Data analysis was performed by using chi square.
ResultsThe results showed that there was a significant relation between levels of the hormone estradiol and the incidence of sexual dysfunction (p=0.000), as well as the length of time using Depo Medroxy Progesterone Acetate on sexual dysfunction (p=0.000).
ConclusionThe result of data analysis is that the duration of Depo Medroxy Progesterone Acetate injection usage significantly reduces the level of the hormone estradiol which can cause sexual dysfunction in Depo Medroxy Progesterone Acetate acceptors.
Hormonal contraception is the type of contraception most favored by family planning participants. Based on data submitted by the BKKBN, there are up to 1,256,250 new family planning participated nationally. When viewed per type of contraception, the percentages are as follows: Intra Uterine Device (IUD): 83,153 (6.62%), female surgery method (MOW/metode operasi wanita): 21,140 (1.68%), male surgery method (MOP/metode operasi pria): 3347 (0.27%), condoms: 75,444 (6.01%), implants: 89,590 (7.13%), injections: 637,379 (50.74%), pills: 346,197 (27.56%).1,2 From these data, it can be seen that hormonal contraceptives, especially injectable contraceptives and pill contraceptives, are the types of contraception that have most participants with filled the first and second ranking.3
Sexual dysfunction in women is an important reproductive health problem because it is related to the continuity of a woman's reproductive function and has a major influence on the harmony of husband and wife relationships. Sexual dysfunction is a persistent or repeated failure, either partially or completely, to obtain and or maintain a vasocongestial lubrication response until the end of sexual activity.4,5
Long-term usage of DMPA will affect estradiol so that it may be lower or in the range of levels in the early follicular phase. After the medicine is used up in the body ovulation and conception can occur and the endometrium can return to normal function.6
Renardy's research (2008) states that in DMPA family planning users for 1–2 years, the average blood estradiol level is 78.69±29.76pg/ml and DMPA family planning users for 3–5 years are 54.23±21.07pg/m.7 Another study conducted by Ningsih (2002) at the Kassi-Kassi Public Health Center in Makassar stated that the use of the DMPA injection contraceptive method affects the incidence of acceptor sexual dysfunction,8 as well as parity affecting the incidence of dysfunction and age is the most influencing factor in the incidence of sexual dysfunction.
The decreasing of sexual desire (libido) in DMPA family planning injection acceptors are rare and not experienced in all women, but in long-term use, it may arise due to hormonal changes, resulting in vaginal drying which causes pain during sexual intercourse and ultimately reduces sexual desire/passion. This situation is a common complaint submitted by 1 in 10–100 acceptors of DMPA users.9,10
Bara-Baraya public health center of Makassar the number of PUS is around 6393 and the coverage of active family planning is 72.22% in 2015. Based on reports at the Bara-Baraya public health center in December 2015, injection acceptors were 31.34% with usage >1 year, pills: 205 (3.65%), IUD: 18 (0.32%), implants: 18 (0.32%) and condoms: 37 (0.66%) (Makassar City Health Office, 2015). In an interview that was conducted on one of the patients who had the family planning injection that the patient had used DMPA injection contraceptives for 7 years and had no complaints other than weight gain and had never checked estradiol levels, only examining vital signs.
Based on the background description above, the long-term use of injectable contraceptives for Depo Medroxyprogesterone Acetate can have an effect on sexual dysfunction in users. Therefore, the author intends to carry out a study that aims to determine the relation between estradiol levels and the length of time usage on sexual dysfunction in Depo Medroxy Progesterone Acetate acceptors at the Bara Baraya public health center of Makassar.
MethodsResearch designThis research was conducted on 19 July–31 July 2016. It was located at Puskesmas Bara-Baraya Makassar, South Sulawesi. This study used a cross-sectional quantitative approach.
Population and sampleThe population in this study were 80 combination pill acceptors in the working area of Bara-Baraya Public Health Center (Puskesmas/pusat kesehatan masyarakat), age <49 years. The sampling technique was carried out by means of accidental sampling.
Method of collecting dataData on the implementation of direct interviews with a questionnaire sheet, consisting of the identity of the respondent and questions about sexual function using the Female Sexual Index Function (FSFI) questionnaire. Radiation levels was measured by using the Makassar Prodia laboratory.
Data analysisThe data analysis used was significant chi square test (α=0.05), it was said that the independent variable and the dependent variable had a significant relationship if the value of ρ<α.
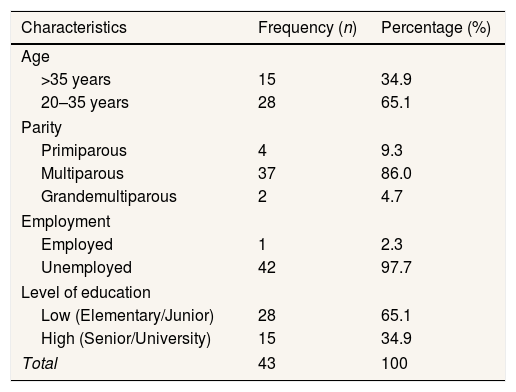
ResultsTable 1 data shows that out of 43 respondents, the majority were not at risk, there were 28 people (65.1%) and the majority with multiparity, there were 37 people (86.0%), most respondents were not working, there were 42 people (97.7%), and the majority of respondents with low education were 28 people (65.1%).
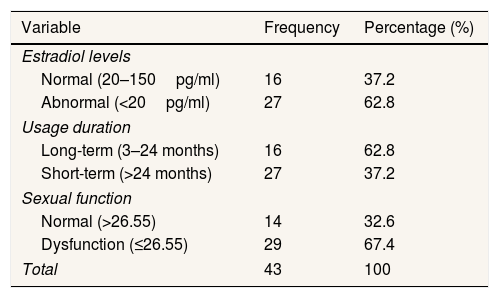
Data in Table 2 shows that of the 43 respondents, the majority of respondents with abnormal estradiol levels were 27 people (62.8%) and respondents with normal estradiol levels were 16 people (37.2%). The majority of the use of Depo Medroxy Progesterone Acetate (DMPA) injections was with long-term use, there were 27 people (62.8%) and short-term use were 16 people (37.2%). 14 people had normal sexual function (32.6%), while 29 people experienced abnormal sexual function (67.4%).
Univariate analysisSee Tables 1 and 2.
Respondent frequency distribution based on characteristics in the public health center work area, Bara-Baraya, Makassar.
| Characteristics | Frequency (n) | Percentage (%) |
|---|---|---|
| Age | ||
| >35 years | 15 | 34.9 |
| 20–35 years | 28 | 65.1 |
| Parity | ||
| Primiparous | 4 | 9.3 |
| Multiparous | 37 | 86.0 |
| Grandemultiparous | 2 | 4.7 |
| Employment | ||
| Employed | 1 | 2.3 |
| Unemployed | 42 | 97.7 |
| Level of education | ||
| Low (Elementary/Junior) | 28 | 65.1 |
| High (Senior/University) | 15 | 34.9 |
| Total | 43 | 100 |
Respondents frequency distribution based on the variables public health center area, Bara-Baraya, Makassar.
| Variable | Frequency | Percentage (%) |
|---|---|---|
| Estradiol levels | ||
| Normal (20–150pg/ml) | 16 | 37.2 |
| Abnormal (<20pg/ml) | 27 | 62.8 |
| Usage duration | ||
| Long-term (3–24 months) | 16 | 62.8 |
| Short-term (>24 months) | 27 | 37.2 |
| Sexual function | ||
| Normal (>26.55) | 14 | 32.6 |
| Dysfunction (≤26.55) | 29 | 67.4 |
| Total | 43 | 100 |
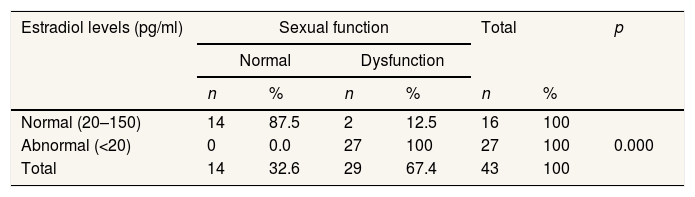
The data in Table 3 shows the results of the chi square analysis with value (ρ=0.000<0.05), it was found that the majority of normal estradiol levels experienced normal sexual function as many as 14 people (93.3%) and there were only 2 respondents (12.5%) who have normal estradiol levels but experienced sexual dysfunction. The majority of respondents with abnormal estradiol levels experienced sexual dysfunction as many as 27 people (100%) and none of the respondents with abnormal estradiol levels experienced normal sexual function.
The relations between estradiol levels and sexual dysfunction in injection acceptors of the Depo Medroxy Progesterone Acetate at Bara-Baraya public health center of Makassar.
| Estradiol levels (pg/ml) | Sexual function | Total | p | ||||
|---|---|---|---|---|---|---|---|
| Normal | Dysfunction | ||||||
| n | % | n | % | n | % | ||
| Normal (20–150) | 14 | 87.5 | 2 | 12.5 | 16 | 100 | 0.000 |
| Abnormal (<20) | 0 | 0.0 | 27 | 100 | 27 | 100 | |
| Total | 14 | 32.6 | 29 | 67.4 | 43 | 100 | |
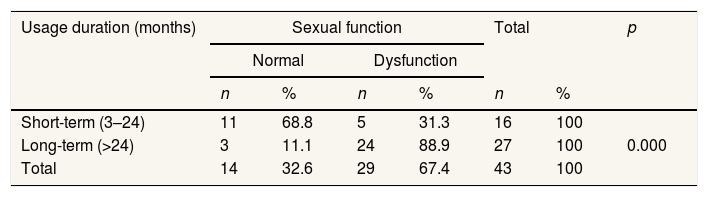
There is data in Table 4 showing the results of the chi square analysis (p=0.000<0.05), it was found that respondents with a long-term of time using Depo Medroxy Progesterone Acetate (DMPA) injections in the short category experienced normal sexual function as many as 11 people (68.8%) and those who experienced sexual dysfunction as many as 5 people (31.3). For respondents who used the old category of Depo Medroxy Progesterone Acetate (DMPA) injection, the majority experienced sexual dysfunction as many as 24 people (88.9%) and only 3 respondents (11.1%) who experience sexual function within normal limits.
The relations between the duration use of Depo Medroxy Progesterone Acetate injections with sexual dysfunction in the acceptors of Depo Medroxy Progesterone Acetate at Bara-Baraya public health center of Makassar.
| Usage duration (months) | Sexual function | Total | p | ||||
|---|---|---|---|---|---|---|---|
| Normal | Dysfunction | ||||||
| n | % | n | % | n | % | ||
| Short-term (3–24) | 11 | 68.8 | 5 | 31.3 | 16 | 100 | 0.000 |
| Long-term (>24) | 3 | 11.1 | 24 | 88.9 | 27 | 100 | |
| Total | 14 | 32.6 | 29 | 67.4 | 43 | 100 | |
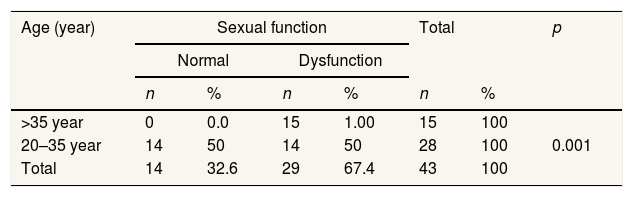
The data in Table 5 shows the results of the chi square analysis (p=0.001<0.05), it was found that respondents aged 20–35 years who experienced normal sexual function and dysfunction had the same number of 14 people (50%). Respondents aged>35 years, the majority of them experienced sexual dysfunction as many as 15 people (100%) and there were no respondents who experienced normal sexual function at the age of the respondents who were at risk.
Relation between age and sexual dysfunction in acceptors of Depo Medroxy Progesterone Acetate at Bara Baraya public health center of Makassar.
| Age (year) | Sexual function | Total | p | ||||
|---|---|---|---|---|---|---|---|
| Normal | Dysfunction | ||||||
| n | % | n | % | n | % | ||
| >35 year | 0 | 0.0 | 15 | 1.00 | 15 | 100 | 0.001 |
| 20–35 year | 14 | 50 | 14 | 50 | 28 | 100 | |
| Total | 14 | 32.6 | 29 | 67.4 | 43 | 100 | |
From the research results, it was found that the value of ρ=0.000<0.05, which means that there is a relationship between estradiol levels and sexual dysfunction in the injection acceptors of Depo Medroxy Progesterone Acetate (DMPA) at the Bara-Baraya Public Health Center Makassar in 2016. Based on the theory that low estradiol levels in women as a result of using Depo Medroxyprogesterone Acetate (DMPA) injectable contraceptives partly contribute to sexual dysfunction. Low levels of serum estradiol and progesterone after injection of Depo Medroxy Progesterone Acetate (DMPA), this is due to inhibition of follicle growth caused by suppression of gonadotropins, causing a decrease in the synthesis of estradiol and progesterone by the ovum (Fortherby et al., 1980).
The results of this study showed that 27 people (100%) experienced Depo Medroxy Progesterone Acetate (DMPA) injection acceptors with abnormal estradiol levels. According to Fraser (1994), estradiol levels decreased with the use of injections of Depo Medroxy Progesterone Acetate (DMPA).11 The injection of Depo Medroxy Progesterone Acetate (DMPA) can reduce ovulation and cause a decreasing libido and sex potency. The mechanism of action of Depo Medroxy Progesterone Acetate (DMPA), which is a long-acting progestational steroid (progesterone), suppresses the production of follicle stimulating hormone (FSH), thereby inhibiting the increase in estrogen levels.
The effect of the injection of Depo Medroxy Progesterone Acetate (DMPA) which reduces serum estradiol levels is closely related to complaints of mood changes, depression and reduced sexual desire of users. From the results of the study using the FSFI score, it was also found that 14 people (87.5%) had normal estradiol levels, but also 2 respondents (12.5%) who experienced sexual dysfunction, this could happen. because women were in the period of breastfeeding. One of the respondents who experienced sexual dysfunction in the category of normal estradiol levels still had a 4 months old child, at which time the acceptors were still breastfeeding their babies. In breastfeeding women, high prolactin levels reduce sex drive and low estrogen levels are associated with vaginal dryness. Sexual problems that occur after childbirth are loss of sexual desire or avoidance and a decrease in the frequency of sexual activity due to more focused attention on baby care, especially at night.12
The results of a study conducted by Fraser (1994), in Australia, found that sexual difficulties in the form of complaints of loss of interest, vaginal dryness and dyspareunia could lead to discontinuation of the use of contraception.11 This complaint was expressed by 43% of the women who became respondents, but continued to use the Depo Medroxy Progesterone Acetate (DMPA) injection method.
The results showed that the value of p=0.000<0.05. Shows that there is a significant relationship between the length of time using Depo Medroxy Progesterone Acetate (DMPA) injections to sexual dysfunction in family planning acceptors at the Bara Baraya Makassar Health Center in 2016.
According to Saifuddin et al. (2006), the length of use is the time passed by the acceptor using contraceptives.13 The side effects caused by the prolonged use of Depo Medroxy Progesterone Acetate (DMPA) injection Depo Medroxyprogesterone Acetate (DMPA), among others, explain that half of the users of Depo Medroxy Progesterone Acetate (DMPA) injection will experience sexual dysfunction. Hormonal contraceptives can cause vaginal dryness, resulting in pain (dyspareunia) during sexual intercourse.
The results of this study found that 24 people (88.9%) experienced Depo Medroxy Progesterone Acetate (DMPA) injection acceptors experienced sexual dysfunction and only 3 respondents (11.1%) experienced normal sexual function. In 3 respondents who experienced normal sexual function, this could be because the estradiol levels in 3 respondents were in the normal range. According to theory, another factor is age. This respondent is still around the age of 27 years. Where at the young reproductive age, the function of the reproductive organs has not decreased. So there is no decrease in the function of the ovaries which produce the hormones estrogen and progesterone which affect sexual function itself.
This means that the use of injections of Depo Medroxy Progesterone Acetate (DMPA) for a long-term resulted a sexual dysfunction. The use of hormonal contraceptives, one of which is the injection of Depo Medroxy Progesterone Acetate (DMPA), will have an effect on the positive feedback effect of estrogen and negative feedback on progesterone. Giving hormones that come from outside the body such as hormonal contraception in the form of estrogen and progesterone causes an increase in the levels of these two hormones in the blood, this will be detected by the anterior pituitary and anterior pituitary and will cause negative feedback by reducing the secretion of FSH and LH hormones and in the presence of progesterone the inhibitory effect of estrogen will be manifold. Within a certain period of time the body can compensate by increasing the secretion of estrogen to keep it in a normal state but in the long term it causes loss of body compensation and decreased secretion of hormones, especially estrogen.14 The use of Depo Medroxyprogesterone Acetate (DMPA) injections over two years has a big risk of the impact of low serum estradiol levels, which can include bone mass loss, prolonged amenorrhea and sexual dysfunction such as low sexual desire that affects a person's sexual life.15
This is in line with the study of Minghui et al. (1999), which studied 44 women who used Depo Medroxy Progesterone Acetate (DMPA) injection, the estradiol serum levels in 20 women who used 4–8 times (12–24 months) were 150.5pmol/l, in 24 women who used Depo Medroxy Progesterone Acetate (DMPA) injection more than 8 times (>24 months) the average estradiol level was 137.6pmol/l.16
The results showed that p=0.010<0.05, indicating a relation between age and sexual dysfunction. This means that the age of the depot injection acceptor of depo medroxyprogesterone acetate affects sexual dysfunction that occurs. From the results of the study, there were 15 people (100%) of respondents aged >35 who experienced sexual dysfunction. The effect of age is highly dependent on hormonal changes regulated by the central nervous system that affect dynamic neural behavior, cognition, biological rhythms and sexual behavior. In the measurement of hormone secretion synchrony, it has been shown that there is a decrease in a regular rhythmic pattern of hormone secretion due to increasing age.
The increasing age, the more frequent sexual disorders are found in women. Due to a lack of the hormone estrogen, blood flow to the vagina is reduced, vaginal fluid is reduced, and the vaginal epithelial cells become thin and prone to injury. Several studies have shown that adequate estrogen levels are the most important factor for maintaining health and preventing the vagina from drying out so that it no longer causes pain during intercourse.6
The results of the study by Morley (2005), on 1,749 women aged between 18 and 59 years showed that 43% of women experienced sexual dysfunction.17 The results of the study indicate that women are more likely to experience decreased sexual function due to increasing age. The thing that needs to be a concern in providing information about the injection contraceptive method of Depo Medroxyprogesterone Acetate (DMPA). Depo Medroxyprogesterone Acetate (DMPA) is the age at which the acceptor will use this method. Although it is still recommended for women over 35 years of age, it needs to be explained that prolonged use (>24 months) will affect hormonal cycles which have an impact on sexual function and the reproductive system and the use of the Depo Medroxyprogesterone Acetate (DMPA) injection method and other hormonal contraceptive methods. should be stopped during perimenopause or around the age of 45 in Indonesian women.18
ConclusionThe results of the study, the duration of using Depo Medroxy Progesterone Acetate injections significantly reduced levels of the hormone estradiol which could cause sexual dysfunction in Depo Medroxy Progesterone Acetate acceptors. Based on the foregoing, it is necessary to carry out further research on other factors that can cause sexual dysfunction such as previous contraceptive history, weight, obesity, psychology, occupation, history of illness, occupation, fatigue and other factors. The need for age grouping of respondents to prevent variables counfounding.
Conflicts of interestThe authors declare no conflict of interest.
Peer-review under responsibility of the scientific committee of the 3rd International Nursing, Health Science Students & Health Care Professionals Conference. Full-text and the content of it is under responsibility of authors of the article.











