



The 3rd International Nursing and Health Sciences Students and Health Care Professionals Conference (INHSP)
More infoThis study aimed to analyze the effectiveness of gentle prenatal yoga on the anxiety problem in primigravida and multigravida pregnant women.
MethodThis study was conducted at Bara-Baraya Health Center, Antang Health Center, Kapasa Health Center, and Mamajang Health Center. The applied research design in this study was a quasi-experiment with a non-equivalent control group design approach. Samples were selected using a purposive sample technique. Furthermore, the instrument used was the Hamilton Anxiety Rating Scale (HARS) questionnaire. The number of samples in this study was 24 respondents divided into two groups, 12 in the intervention group and 12 in the control group. Meanwhile, the criteria of samples in this study were pregnant women in the first to fifth pregnancy, having been in trimester II-III with the gestational age of ≥20–30 weeks, and not having complications in pregnancy.
Resultsthe HARS scores in the intervention group showed that the mean rank of the pre-test was 23.75, In the mid-test, it was 20.00, and in the post-test, it was 16.00. Meanwhile, in the control group, its mean rank was 23.50, mid-test it was 21.58, and the post-test it was 20.41 showed that the intervention group experienced a significant decrease in anxiety levels. From the results of the Mann Whitney test, the intervention group p=0.001<(α 0.05) showed that there were significant changes.
ConclusionThere were differences in HARS (Hamilton Anxiety Rating Scale) scores between the intervention and control groups before and after a gentle prenatal yoga treatment.
Pregnancy is a crisis period that ends with the birth of a baby. This process lasts about 40 weeks, affecting physiological, psychological, and biological changes in mothers caused by hormone levels during pregnancy.1 This is experienced by primigravid and multigravid pregnant women. During pregnancy, women are very vulnerable to experience psychological disorders such as anxiety. Pregnancy anxiety is a negative emotional state that involves anxiety about the health and condition of the fetus, the birthing process that will go through, and the problem of readiness to become a mother who is often associated with adverse effects on the mother and fetus that further have an impact on the growth and development of children. About 30.9% of mothers experience anxiety during each trimester of pregnancy. Meanwhile, 6.9% of them experience anxiety throughout their pregnancy.
Anxiety and depression occur due to dysfunction in the cortical and limbic areas, which manages the mood, learning, focus, and working memory. They are related to the coping mechanism in each individual and the improvement of the neurobiological system. Several studies mention that anxiety is a cause of complications in pregnancy. In addition, several factors that can affect antenatal anxiety are parity, obstetric status, husband support, and health behavior. Measurement of the level of anxiety in pregnant women was using the Hamilton Anxiety Rating Scale (HARS), which consists of 14 question items and is rated 0, 1, 2, 3, or 4 for each item. A value of 0 indicates that no symptoms are visible, while a value of 4 indicates that symptoms are often experienced and very disturbing. The obtained total value will determine the level of anxiety, i.e., mild (14–20), moderate (21–27), severe (28–41), very severe (42–56).
Before pregnancy, vulnerabilities relating to social, family, cultural, and environmental conditions can also increase anxiety during the pregnancy process. It further implicates the maternal–fetal–placental system, especially during sensitive periods such as early pregnancy. To overcome these problems, several appropriate and safe solutions for pregnant women are a spiritual approach, meditation, and behavioral techniques Schetter (2011)2 such as pregnancy exercise and yoga. Pregnancy exercise is a fitness movement to strengthen muscles, reduce pain, and reduce maternal anxiety during pregnancy and the birthing process.3 In a study conducted by Miftah (2015),4 he found out that prenatal yoga reduces anxiety levels in pregnant women. A similar result was also found by Hamdiah et al. (2017)5 that giving yoga treatment twice a week can reduce stress and anxiety levels and increase emotional intelligence.
MethodsThe applied research design in this study was a quasi-experiment with a non-equivalent control group design approach. The design involved two groups, i.e., the intervention group and the control group. Each group was tested three times, i.e., before being given treatment I, before being given Treatment IV, and after being given Treatment VIII using the Hamilton Anxiety Rating Scale (HARS) questionnaire. The number of samples in this study was 24 respondents divided into two groups, 12 in the intervention group and 12 in the control group. The criteria of samples in this study were pregnant women in the first to fifth pregnancy, having been in trimester II-III with the gestational age of ≥20–31 weeks, and not having complications in pregnancy.
Research locationThis study was conducted at the Bara Baraya Health Center, Antang Health Center, Kapasa Health Center, Mamajang Health Center from February to June 2020. This study also had received an ethical approval recommendation with protocol number UH19121116 on January 30, 2020.
Data sourceThe collected data were demographic data (age, educational level, occupation, and gravida) and respondents’ anxiety level data using the HARS (Hamilton Anxiety Rating Scale) questionnaire.
Data collection techniqueIn this study, data were collected using a HARS questionnaire sheet. The collected data were then documented in the master table.
Data analysisData were analyzed and statistically tested based on the research variables. In this study, the applied analysis method was comparative hypothesis testing for numerical variables with abnormal data distribution using the Wilcoxon test and Mann Whitney test.
ResultsThe research results are presented as follows.
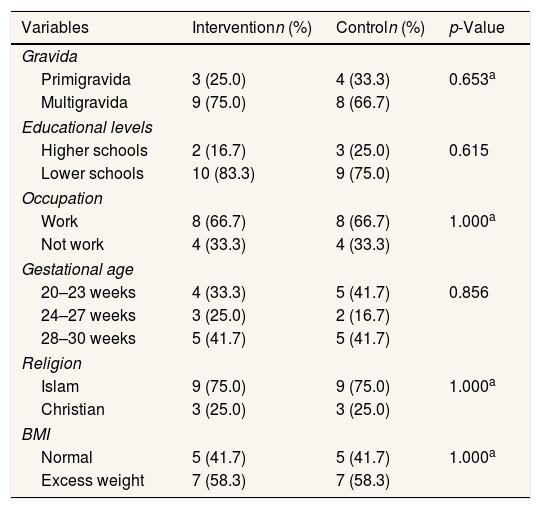
DiscussionBased on the statistical tests in Tables 1 and 2, the characteristics of the respondents did not show a significant difference based on gravida, educational level, and occupation between respondents from the intervention group and the control group.
Characteristics of respondents.
| Variables | Interventionn (%) | Controln (%) | p-Value |
|---|---|---|---|
| Gravida | |||
| Primigravida | 3 (25.0) | 4 (33.3) | 0.653a |
| Multigravida | 9 (75.0) | 8 (66.7) | |
| Educational levels | |||
| Higher schools | 2 (16.7) | 3 (25.0) | 0.615 |
| Lower schools | 10 (83.3) | 9 (75.0) | |
| Occupation | |||
| Work | 8 (66.7) | 8 (66.7) | 1.000a |
| Not work | 4 (33.3) | 4 (33.3) | |
| Gestational age | |||
| 20–23 weeks | 4 (33.3) | 5 (41.7) | 0.856 |
| 24–27 weeks | 3 (25.0) | 2 (16.7) | |
| 28–30 weeks | 5 (41.7) | 5 (41.7) | |
| Religion | |||
| Islam | 9 (75.0) | 9 (75.0) | 1.000a |
| Christian | 3 (25.0) | 3 (25.0) | |
| BMI | |||
| Normal | 5 (41.7) | 5 (41.7) | 1.000a |
| Excess weight | 7 (58.3) | 7 (58.3) | |
a Chi-square.
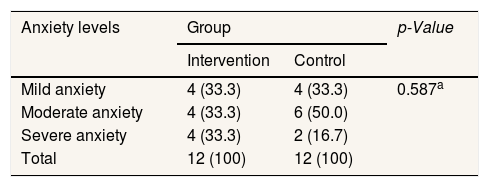
Characteristics of respondents based on the level of anxiety in the intervention and control groups.
| Anxiety levels | Group | p-Value | |
|---|---|---|---|
| Intervention | Control | ||
| Mild anxiety | 4 (33.3) | 4 (33.3) | 0.587a |
| Moderate anxiety | 4 (33.3) | 6 (50.0) | |
| Severe anxiety | 4 (33.3) | 2 (16.7) | |
| Total | 12 (100) | 12 (100) | |
a Chi-square.
In Diagram 1, the HARS scores of the primigravid and multigravid pregnant women in the intervention group showed that a mean rank of the pre-test was 23.75, meaning that they were at a mild anxiety level. In the mid-test, it was 20.00, meaning that they were still at a mild anxiety level. Furthermore, in the post-test, it was 16.00, meaning that they were also at a mild anxiety level. Meanwhile, in the control group, the mean rank of the pre-test was 23.50, meaning that they were at a moderate anxiety level. In the mid-test, it was 21.58, meaning that they were at a mild anxiety level. Furthermore, in the post-test, it was 20.41, meaning that they were at a moderate anxiety level.
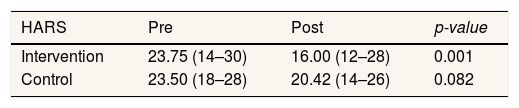
In Table 3, the Mann Whitney test result indicates a difference between the level of anxiety in primigravida and multigravida pregnant women after being given a prenatal gentle yoga treatment eight times.
the result of Mann Whitney test on comparing HARS scores between primigravid and multigravid pregnant women during the pre-test, post-test in the intervention and control groups.
| HARS | Pre | Post | p-value |
|---|---|---|---|
| Intervention | 23.75 (14–30) | 16.00 (12–28) | 0.001 |
| Control | 23.50 (18–28) | 20.42 (14–26) | 0.082 |
a Wilcoxon test.
Anxiety during pregnancy cannot be avoided because pregnancy is a source of anxiety stressors Rahmitha (2017)6 related to mental, emotional, and behavioral conditions.7 Anxiety is an emotional response to an individual's subjective assumption influenced by the subconscious yet explicitly known for its causes. Therefore, in dealing with anxiety, pregnant women need safe and comfortable therapy, such as yoga. In its implementation, yoga consists of five parts, i.e., physical exercise (asana), breathing exercise (pranayama), position exercise (Nidra), meditation exercise (dhyana), and deep relaxation exercise combined with positive affirmations.8 Yoga provides benefits in building a healthy balance between all aspects of the body and mind, increasing the inner bonds of mother and fetus, creating relaxed conditions, and giving a positive aura to the body.
This study showed a decrease in the HARS score or anxiety level after respondents were given prenatal gentle yoga treatment eight times, combined with physical exercise, mental exercise, spiritual exercise, breathing exercise, and positive affirmation exercise. Some previous studies suggested that yoga helps improving mental energy, increasing positive feelings, and reducing depression and anxiety. Nasal breathing techniques in yoga can increase parasympathetic activity, make breathing regular, and give a feeling of calm and relaxation.9–11 In addition, the result of this study is in line with a study conducted by Novelia et al. (2018)8 that, by using the HARS instrument, there are differences in anxiety levels between the intervention and control groups meaning that yoga relaxation affects anxiety levels of pregnant women. A similar result was found in a study conducted by Maharani and Hayati (2020)12 that pregnant women who have severe anxiety before being given a yoga treatment have decreased anxiety levels to be in a mild anxiety level with a p-value of <0.001 after being given a yoga treatment.
ConclusionPrenatal gentle yoga therapy effectively reduces anxiety levels in primigravid and multigravid pregnant women indicated by the results of the HARS scores in which pregnant women have decreased anxiety levels from before being given treatment to after being given treatment IV after being given treatment VIII.
Conflicts of interestThe authors declare no conflict of interest.
Peer-review under responsibility of the scientific committee of the 3rd International Nursing, Health Science Students & Health Care Professionals Conference. Full-text and the content of it is under responsibility of authors of the article.











