




To assess differences in mortality rates between social security statuses in two independent samples of Belgian and Spanish male workers.
MethodsStudy of two retrospective cohorts (Belgium, n=23,607; Spain, n=44,385) of 50–60 year old male employees with 4 years of follow-up. Mortality rate ratios (MRR) were estimated using Poisson regression models.
ResultsMortality for subjects with permanent disability was higher than for the employed, for both Belgium [MRR=4.56 (95% CI: 2.88–7.21)] and Spain [MRR=7.15 (95% CI: 5.37–9.51)]. For the unemployed/early retirees, mortality was higher in Spain [MRR=1.64 (95% CI: 1.24–2.17)] than in Belgium [MRR=0.88 (95% CI: 0.46–1.71)].
ConclusionMRR differences between Belgium and Spain for unemployed workers could be partly explained because of differences between the two social security systems. Future studies should further explore mortality differences between countries with different social security systems.
Evaluar diferencias en la mortalidad según el estado de afiliación a la seguridad social en dos muestras independientes de hombres trabajadores belgas y españoles.
MétodosDos cohortes retrospectivas de hombres asalariados de 50-60 años de edad (23.607 belgas y 44.385 españoles) seguidos durante 4 años. Se estimaron razones de tasas de mortalidad (RTM) mediante modelos de regresión de Poisson.
ResultadosLa mortalidad para los incapacitados permanentes fue mayor que para los empleados en ambos países [RTM=4,56 (IC95%: 2,88-7,21) en España y RTM=7,15 (IC95%: 5,37-9,51) en Bélgica], pero para los desempleados/jubilados anticipadamente fue mayor en España [RTM=1,64 (IC95%: 1,24 - 2,17)] que en Bélgica [RTM=0,88 (IC95%: 0,46-1,71)].
ConclusiónLas diferencias encontradas entre los desempleados de Bélgica y España podrían ser parcialmente explicadas por las diferencias entre ambos sistemas de seguridad social. Futuros estudios deberían explorar estas diferencias entre países con distintos sistemas de seguridad social.
A main function of social security arrangements is to provide assistance and income support to workers who leave the active labor force before the legal retirement age, due to early retirement, unemployment or permanent disability.1,2 For these workers, income replacement schemes play a key role in maintaining their living status and –related to that– also their health status. In this respect, it has been shown that social inequalities in health/mortality between citizens in different social statuses vary between countries with different levels of social protection.3
Our aim was to address this fundamental question for the first time using social security registry data. More specifically we aim to explore mortality differences according to social status in older working-aged men, in Belgium and Spain.
MethodsData from BelgiumThe Belgian sample was based on the Crossroads Bank for Social Security (CBSS) registry.4 This study is based on data from an ad-hoc extraction of a 10% sample of the social security registry database for private sector employees aged 50 to 59 in 2003. These persons were followed registering their mortality from 1 January 2004 to 31 December 2007. The information about the individuals in this sample (with anonymous identifier) contained personal data and affiliation data, including old age retirement, disability and unemployment as well as data on mortality.
Data from SpainThe Spanish sample was based on the administrative registry of the population affiliated to the Social Security System. This system includes those who were workers, unemployed receiving an unemployment benefit, and pensioners. For this study we used the so-called Continuous Working Life Sample (CWLS).5 This sample was initiated in 2004 and comprised a random sample of 4% of the individuals affiliated with the Spanish Social Security System. The individual information in the CWLS (also anonymous) includes personal data and affiliation characteristics such as information related to contracts, unemployment benefits, disability and retirement pension, as well as the date of decease.
Arrangement of data and statistical analysisAfter a process of data harmonization, making both administrative datasets mutually comparable, we obtained two retrospective cohorts of men with a 4-year follow-up. Women were excluded from both cohorts because in the Belgian cohort reliable data on female workers was not available yet due to the impossibility of assigning exact employment statuses. For both cohorts, individuals aged 50 to 60 who were working as employees one year before the start of follow-up were retained (January 2003 for Belgian and 2004 for Spanish). This lag between the cohort definition and the beginning of follow-up was considered in order to achieve, at this point, a sample with more than one year of enrollment to the system and therefore, minimize selection bias as a consequence of the healthy worker effect. The main exposure variable was social security status, consisting of three categories: employed, unemployed and disabled. Also for reasons of comparability, the unemployed and early retired were included together in both cohorts, since Spanish registry does not distinguish between early retirees and unemployed in workers under age 60. The social security statuses were observed at the beginning of the follow-up–that is, in January 2004 for the Belgian cohort and January 2005 for the Spanish cohort. Sample size at the beginning of follow-up was 23,607 employees for Belgium (12,316 manual and 11,291 non-manual) and 44,385 for Spain (23,231 and 21,154 respectively). Person-years were calculated for each employee from the beginning of follow-up until either the end of follow-up or the decease. Crude mortality rates (MR) and occupation-adjusted mortality rate ratios (MRR) were estimated for the Belgian and Spanish sample, using Poisson regression models, using Stata 10.1 © software.
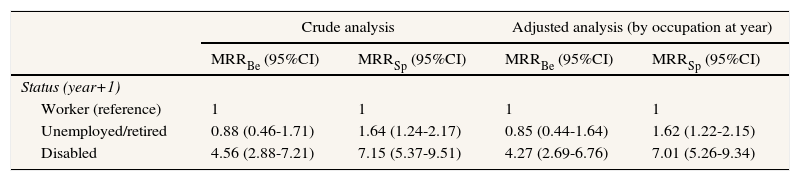
ResultsThe MR (Table 1) for individuals still working at the beginning of follow-up (reference category) was 52.87 (95%CI: 48.13-57.95) per 10,000 person-years for Belgium and 46.6 (95%CI: 43.39-49.98) for Spain. The MR (Tables 1 and 2) for those individuals that were disabled at the beginning of follow-up, was considerably higher in both Belgium [MR=244.64 (95%CI: 147.29–382.03); adjusted MRR=4.27 (95%CI: 2.69–6.76)] and Spain [MR=333.02 (95%CI: 247.17–439.04); adjusted MRR=7.01 (95%CI: 5.26-9.34)]. The MR for those individuals that were unemployed at the beginning of follow-up compared with those who remained working, was significantly higher in Spain [MR=76.44 (95%CI: 57.09-100.24); adjusted MRR=1.62 (95%CI: 1.22-2.15)], but not in Belgium [MR=61.84 (95%CI: 44.18-84.20); MRR=0.85 (95%CI: 0.44–1.64)].
Mortality rate (per 10,000 person-years) among men aged 50-60 in the beginning of 4 years follow-up (2004-2007, Belgium and 2005-2008, Spain) by social security status.
| Belgium | Spain | |||||
|---|---|---|---|---|---|---|
| Cases | Person-years | MR (95%CI) | Cases | Person-years | MR (95%CI) | |
| Status (year+1) | ||||||
| Worker (reference) | 456 | 86,250 | 52.87 (48.13 - 57.95) | 781 | 167,605 | 46.6 (43.39 - 49.98) |
| Unemployed/retired | 40 | 6,469 | 61.84 (44.18 - 84.20) | 52 | 6,803 | 76.44 (57.09 - 100.24) |
| Disabled | 19 | 777 | 244.64 (147.29 - 382.03) | 50 | 1,501 | 333.02 (247.17 - 439.04) |
MR: mortality rate.
Mortality rate ratios among men aged 50-60 in the beginning of 4 years follow-up (2004, Belgium; 2005, Spain) by social security status.
| Crude analysis | Adjusted analysis (by occupation at year) | |||
|---|---|---|---|---|
| MRRBe (95%CI) | MRRSp (95%CI) | MRRBe (95%CI) | MRRSp (95%CI) | |
| Status (year+1) | ||||
| Worker (reference) | 1 | 1 | 1 | 1 |
| Unemployed/retired | 0.88 (0.46-1.71) | 1.64 (1.24-2.17) | 0.85 (0.44-1.64) | 1.62 (1.22-2.15) |
| Disabled | 4.56 (2.88-7.21) | 7.15 (5.37-9.51) | 4.27 (2.69-6.76) | 7.01 (5.26-9.34) |
MRR: mortality rate ratio; Be: Belgium; Sp: Spain.
In this study, mortality differences in two comparable national samples of older workers were analyzed separately. MRR for workers who became unemployed in the year prior to mortality follow-up, compared to those who remained employed was not significant in Belgium, while it was in Spain. At the same time, for both countries, the MRR of those becoming disabled in the year prior to follow-up was significant when compared to the same reference category of workers who remained employed.
Regarding the differences in mortality for unemployed, it could be assumed that differences in social security coverage explain the more favourable situation of the Belgian unemployed. We must take into account that unemployment insurance benefit duration has no limit in Belgium, while it is limited to 24 months in Spain.6 Furthermore, along the mortality follow-up period, the replacement rates for long term unemployment vary, depending on the family burdens, between 35 and 81% in Belgium and 0 and 54% in Spain.7 These replacement rates, i.e. the losses in purchasing power, can be a crucial pathway through which unemployment affects health.8,9 In order to better confirm these hypotheses, future studies should ideally include additional information, for example on the composition of the category of the unemployed (e.g. the economic sectors and occupations), the selection criteria of other income replacement schemes,10 detailed socio-economic and demographic background characteristics, etc. On the other hand, results were similar when the association between permanent disability and mortality was assessed, founding higher mortality for disability pensioners in both countries. A result which is consistent with previous results.11,12
The main limitations of this study include difficulties related to making datasets comparable. This obliged the researchers to make compromises related to the study design as well as the number of covariates and the extent of detail of the categorization of central indicators. Also, as it was remarked in the methods section, the absence of data for women was due to problems related to the reliability of the data. A future inclusion of women employees in our analysis will give a necessary gender perspective. Finally, the absence of disability and mortality medical diagnoses on the CWLS has been, to date, a major challenge that must be taken into account as well as the absence of other health measures.
Nevertheless, bearing these limitations in mind, we would like to highlight the value for occupational health research of comparing cohorts of workers coming from social security registry data from different countries. Nowadays, in Europe, more countries dispose of detailed administrative datasets allowing for the reconstruction of detailed and long-term employment careers and relating these to outcomes of mortality, disability or medical consumption.13
In this respect, a cross-country panel of normalized data taken from administrative registers would improve our knowledge on this important issue.
Editor in chargeMiguel Ángel Negrín Hernández.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Income differences related to generosity of unemployment benefits have been described as an explanation for cross-national differences in the association between unemployment status and health.
What does this study add to the literature?Initially employed 50-60 year old employees, becoming unemployed have higher mortality risk compared to those remaining employed in Spain, but not in Belgium. This study should be considered as a first standardized comparison of employment-related mortality data from two national administrative registries, which is a new and promising research approach.
This work was supported by grants from the Instituto Salud Carlos III-FEDER (FIS PI14/00057), the Spanish National Health Institute Carlos III (FIS 08/0914 and FIS 11/01470), the CIBER of Epidemiology and Public Health and the Research Foundation Flanders (G036816N).
Authorship contributionsP. Deboosere and F.G. Benavides conceived the idea of this paper and designed the study with X. Duran and C. Vanroelen. X. Duran conducted the statistical analyses. X. Duran and C. Vanroelen wrote the initial draft. All of the authors critically reviewed numerous drafts of the manuscript and agreed on this final version.
Conflict of interestNone.











