




To estimate the intangible effects of alcohol misuse on the drinker's quality of life, based on general population preferences
MethodsThe most important effects (dimensions) were identified by means of two focus groups conducted with patients and specialists. The levels of these dimensions were combined to yield different scenarios. A sample of 300 people taken from the general Spanish population evaluated a subset of these scenarios, selected by using a fractional factorial design. We used the probability lottery equivalent method to derive the utility score for the evaluated scenarios, and the random-effects regression model to estimate the relative importance of each dimension and to derive the utility score for the rest of scenarios not directly evaluated.
ResultsFour main dimensions were identified (family, physical health, psychological health and social) and divided into three levels of intensity. We found a wide variation in the utilities associated with the scenarios directly evaluated (ranging from 0.09 to 0.78). The dimensions with the greatest relative importance were physical health (36.4%) and family consequences (31.3%), followed by psychological (20.5%) and social consequences (11.8%).
ConclusionsOur findings confirm the benefits of adopting a heterogeneous approach to measure the effects of alcohol misuse. The estimated utilities could have both clinical and economic applications.
Estimar los efectos intangibles del consumo abusivo de alcohol en la calidad de vida del bebedor, según las preferencias sociales.
MétodosLos efectos más relevantes se identificaron mediante dos grupos focales realizados con pacientes y especialistas. Los niveles de estas dimensiones se combinaron para producir diferentes escenarios. Una muestra de 300 personas de la población general española evaluó un subconjunto de estos escenarios, seleccionados mediante un diseño factorial fraccional. Se utilizó el método de lotería equivalente para obtener la utilidad asociada a cada uno de los escenarios evaluados. Para estimar la importancia relativa de cada dimensión y obtener la utilidad para el resto de escenarios no evaluados se estimó una regresión con efectos aleatorios.
ResultadosSe identificaron cuatro efectos intangibles relevantes (familia, salud física, salud psicológica y social) con tres niveles de intensidad. Las utilidades asociadas a cada uno de los escenarios evaluados presentan una amplia variación (entre 0,09 y 0,78). La dimensión con mayor importancia relativa son las consecuencias en la salud física (36,4%) y las consecuencias en la familia (31,3%), seguidas de las consecuencias psicológicas (20,5%) y las sociales (11,8%).
ConclusionesNuestros resultados confirman la conveniencia de adoptar un enfoque heterogéneo para medir los efectos del abuso del alcohol. Las utilidades estimadas podrían tener aplicaciones tanto clínicas como económicas.
Alcohol-related disorders have multiple intangible adverse effects —such as suffering, loss of healthy living, or the deterioration of social and family relationships— that lead to a reduction in the drinker's quality of life.1 Traditionally alcohol-related disorders were divided into two separate categories, abuse and dependence. However, the last edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM–5)2 combines these categories into a single disorder measured on a continuum from mild to severe. In adopting this approach, we expect the adverse effects of alcohol misuse on the quality of life (QoL) to increase as we move along this continuum of severity. Although there is no universally accepted definition for the concept of QoL, ample literature identifies several dimensions that may be affected.3,4 In the empirical literature, the measurement of these effects has been approached in different ways. The majority of the studies quantifying the effect of alcohol misuse on QoL have devoted their attention to measure the health-related quality of life (HRQL), using non preference-based generic instruments such as the 36-Item Short Form Health Survey (SF-36) and its variants.4–10 However, these instruments are not appropriate for economic evaluations, in other words, they cannot be used to prioritize different health care programs and thus to assist decision- making about the allocation of health resources.11
For economic evaluations, the recommended approach for measuring HRQL is to use preference-based measures, quality-adjusted life year (QALY) being the most widely used. To estimate the number of QALYs lost because of alcohol misuse (or gained from an intervention), life years are weighted by preference weights (or utilities), where zero indicates death and one indicates good health (with a negative value indicating states worse than death). In studies on alcoholism, utilities are usually obtained to measure HRQL changes in response to a treatment or intervention, using generic HRQL scales, primarily the EuroQol-5D12–14 or the Short Form 6D.15,16 Another approach (also using generic scales), involves conducting population studies,17–20 which seek to estimate the HRQL lost from alcohol misuse by using other groups of general population as a control group. However, the generic scales cited focus on evaluating the effects of alcohol misuse on HRQL and they ignore other intangible effects (family breakdown, social isolation, etc.), which may even have a greater impact on QoL than do health problems.3,4,21,22 This narrow focus can lead to a large underestimation of the impact of different scenarios of alcohol misuse and could explain the lack of responsiveness of these generic HRQL scales in detecting meaningful changes in QoL found in the empirical literature.18–20,14 In this line of reasoning, the suitability of these generic scales to measure the impact of alcohol misuse has been questioned.23
The few studies that have quantified the impact on QoL in a broad sense, using preference-based measures and estimating directly utilities for alcohol misuse profiles, have obtained a significant negative impact.24–26 However, these studies have important limitations. Stouthard et al.26 and Sanderson et al.25 obtain the utility weights from the preferences of a small sample of physicians (less than 50). On the contrary, economic evaluation manuals recommend eliciting preferences from a representative sample of the general population.11 In addition, the study of Stouhard et al.26 does not directly estimate the weights for alcohol dependence (these weights were elicited from interpolations of others disease stages directly evaluated). Finally, the methodology used in these studies does not allow to identify and estimate the relative importance of QoL dimensions that are more affected by alcohol abuse.
This pilot study provides new empirical evidence on the loss of QoL associated with alcohol misuse, trying to overcome the limitations of previous studies. First, we estimate not only the impact on HRQL (as the generic HRQL scales do) but also other intangible effects, closely related to alcohol misuse. We focus on evaluating intangible effects because they have received the least attention in the literature and because the World Health Organization advocates “that they be explicitly separated from financial costs” (e.g., lost productivity or health care costs).1 Second, we consider alcohol-related problems along a continuum of severity and therefore, although most evaluated states correspond to situations of alcohol dependence, we do not assume an explicit separation between abuse and dependence. The methodology proposed is capable of both identifying this heterogeneity and assigning values to several patient profiles. Third, we estimate utility indices based on a representative sample of the general population. Fourth, the method used to elicit preferences, the “probability lottery-equivalent” method, has only recently been applied in health economics, but it seems to mitigate some of the problems encountered when using the “standard gamble” method. Finally, we identify the relative importance of each dimension.
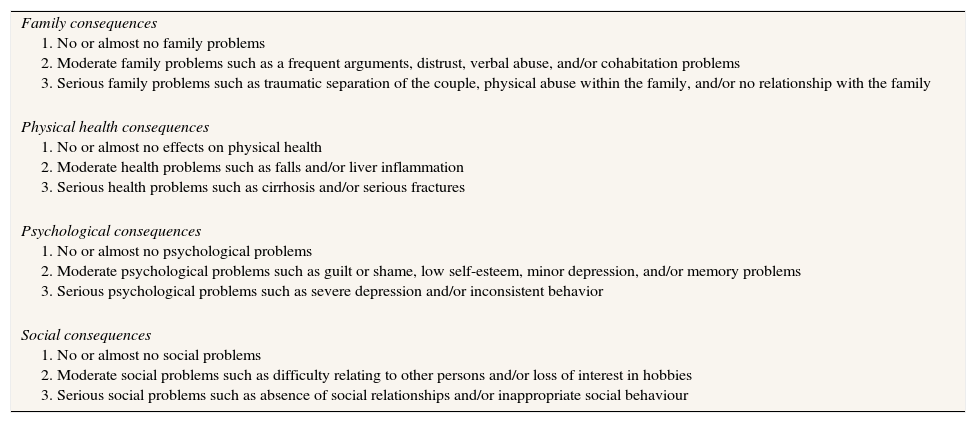
MethodsFocus groups and sampleThe objective of our study's initial phase was to identify the most relevant consequences (dimensions) of alcohol misuse on the drinker's QoL. Dimensions were identified by means of two focus groups conducted with patients and specialists, both recruited from an alcoholism treatment unit in Galicia, a region in northwest Spain (see supplementary online Appendix 1). Briefly, we began by requesting the participants to identify what they considered the most negative consequences of alcohol misuse in a drinker's life. These consequences were then discussed within each group, grouping those reflecting similar outcomes. Finally, each participant ordered the assembled consequences in terms of their importance. We performed a subsequent interview with the specialist group to discuss the levels of dimensions and the clustering of some of them. As result of this process the following (ordered) list of consequences were obtained: family consequences, physical health consequences, psychological consequences, social consequences, labor problems, legal problems and health expenditures. Both groups listed these consequences; the only exception was health expenditures, which was mentioned only by the specialists. We selected the first four dimensions because these were considered the most relevant by participants in both groups and clearly captured the intangible effects of alcohol misuse. Table 1 lists the dimensions and the levels selected.
Intangible effects of alcohol dependence.
| Family consequences 1. No or almost no family problems 2. Moderate family problems such as a frequent arguments, distrust, verbal abuse, and/or cohabitation problems 3. Serious family problems such as traumatic separation of the couple, physical abuse within the family, and/or no relationship with the family |
| Physical health consequences 1. No or almost no effects on physical health 2. Moderate health problems such as falls and/or liver inflammation 3. Serious health problems such as cirrhosis and/or serious fractures |
| Psychological consequences 1. No or almost no psychological problems 2. Moderate psychological problems such as guilt or shame, low self-esteem, minor depression, and/or memory problems 3. Serious psychological problems such as severe depression and/or inconsistent behavior |
| Social consequences 1. No or almost no social problems 2. Moderate social problems such as difficulty relating to other persons and/or loss of interest in hobbies 3. Serious social problems such as absence of social relationships and/or inappropriate social behaviour |
Altogether, the different levels of each dimension yield 81 hypothetical scenarios. As usual, we assume that the utility of each scenario can be represented by an additive model without interactions. This assumption allows us to reduce the total number of states (cards) to be evaluated to nine by using an orthogonal, fractional factorial design. To evaluate the nine cards, face-to-face interviews were conducted with individuals from a sample of 300 people living in Galicia. The sample was randomly selected using stratified random sampling adjusted for gender and age quotas.
Elicitation procedureWe used the probability lottery–equivalent method,27,28 a variant of the lottery-equivalent method,29 to derive utility weights. There is empirical evidence suggesting that this method mitigates the overvaluation of health states from the “standard gamble” approach.28,30 Another advantage of our approach is that the same procedure can be used to estimate utilities both of states better and worse than dead.
Participants were asked to suppose that life circumstances had led them to consume alcohol excessively and that, as a result, they found themselves in the situation described on one of the nine cards. Respondents were then asked to choose between two hypothetical free treatments. Treatment A has a 50% chance of success (alcohol dependence would be cured) and a 50% chance of failure (their state of alcoholism would continue). Treatment B has a 50% chance of success and a 50% chance of failure, but in this case, the result of failure is death (supplementary online Appendix 2 shows this part of the questionnaire). Depending on the respondent's answer, the probability P of treatment B's success is varied according to a pre-established sequence. Each variation of this question is accompanied by a corresponding visual aid. The objective of this iteration is to identify at what point the respondent is indifferent between the two treatments.
We use P* to denote the probability of success that makes the respondent indifferent between treatments A and B; we denote by U(S) the utility of any health state S, where U(G) and U(D) correspond to the utility of two specific states: good health and death. Then, according to the theory of expected utility, 0.5×U(G)+0.5×U(S)=P*×U(G)+(1−P*)×U(D). By convention we have U(G) = 1 and U(D) = 0, so U(S) = (P* − 0.5)/0.5. We use this expression to calculate the utility of the nine cards for each respondent. From a practical standpoint, however, it is not always possible to find the “indifference probability” P* for the person being interviewed. Frequently we can only obtain an interval within which P* falls (for example, if treatment B is preferred when P=0.90 but treatment A is preferred when P=0.85). In such cases, U(S) is presumed to be the interval's intermediate utility. Appendix shows the utilities associated with each of the sequence outcomes in the shaded boxes.
QuestionnaireEach participant valued the nine alcohol dependence states —in a randomized order— using the probability lottery–equivalent method. For each state, participants were asked to imagine themselves being in that situation. They were told the state of dependence described by each card did not result in loss of income because it had no effect on their job, because they never worked, or because they received social assistance that compensated for any loss incurred. Thus, participants were informed that they should consider only the consequences shown. Next, respondents indicated if they preferred treatment A or B and, depending on the answer, one of the routes shown in Appendix was followed. We also recorded each participant's socioeconomic characteristics: age, gender, education, income, labour status, and type of cohabitation. With regard to alcohol, respondents were asked about their own levels of consumption and whether anyone they knew well had alcohol problems. Finally, their state of health was assessed via the SF-6D,31 applying the weights estimated for Spain.28
Statistical analysisFirst, utilities were derived for the nine states evaluated by each participant. Second, in order to estimate utilities for states that were not valued directly, a regression analysis was performed in which the dependent variable was the utility provided by the interviewee for each of the nine cards and the independent variables were the different levels that a card contained. The random-effects regression model was used because the same individual provided nine answers and so those observations were not independent. The relative importance of each dimension can be calculated from the estimated coefficients, using the partial log-likelihood analysis,32 which is appropriate when an orthogonal design is used.
Validity analysisWe calculated dominance tests to analyze the internal consistency of responses. Situations of dominance were identified among the nine cards analyzed. We say that one card “dominates” another card when the former describes a state that is better in terms of at least one dimension and no worse along any other dimension. Accordingly, card 9 dominated cards 1, 2, 6, 7, and 8; and card 6 was dominated by cards 3, 4, 5, 7, and 9. We consider that a dominance test is violated if a worse health state is valued higher than a better health state. The individual test is naturally more difficult than the aggregate test because individuals cannot evaluate all the cards at once. We therefore expected that some individuals would commit random errors when assigning their valuations. Theoretical validity was assessed by checking for whether the coefficients estimated in the regression model were of the expected sign.
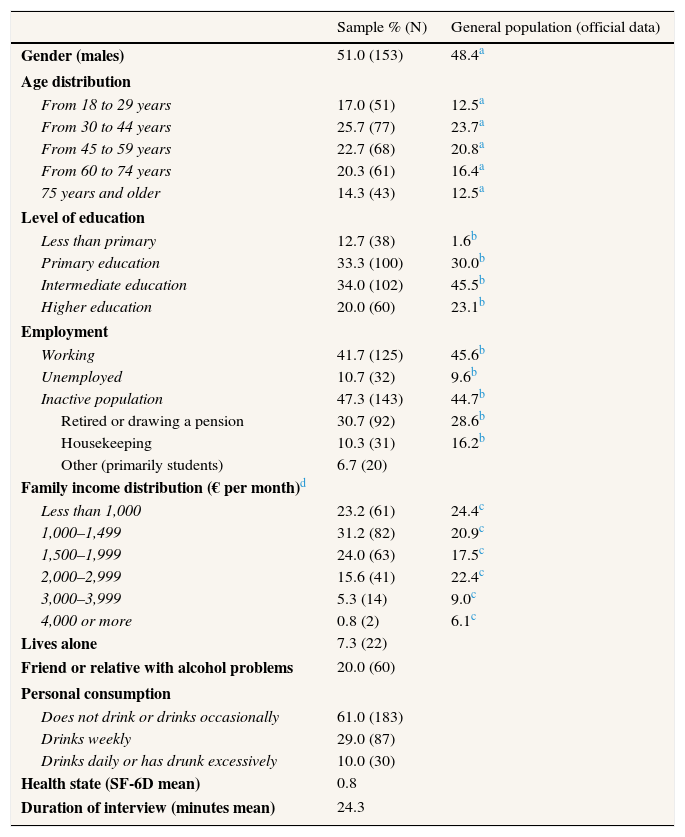
ResultsTable 2 gives the characteristics of the sample along with official data for the Galician general population from which the sample was taken. The sample was strongly similar to the general population in terms of age, gender, and labor status but exhibited slightly lower levels of education and income.
Description of the sample.
| Sample % (N) | General population (official data) | |
|---|---|---|
| Gender (males) | 51.0 (153) | 48.4a |
| Age distribution | ||
| From 18 to 29 years | 17.0 (51) | 12.5a |
| From 30 to 44 years | 25.7 (77) | 23.7a |
| From 45 to 59 years | 22.7 (68) | 20.8a |
| From 60 to 74 years | 20.3 (61) | 16.4a |
| 75 years and older | 14.3 (43) | 12.5a |
| Level of education | ||
| Less than primary | 12.7 (38) | 1.6b |
| Primary education | 33.3 (100) | 30.0b |
| Intermediate education | 34.0 (102) | 45.5b |
| Higher education | 20.0 (60) | 23.1b |
| Employment | ||
| Working | 41.7 (125) | 45.6b |
| Unemployed | 10.7 (32) | 9.6b |
| Inactive population | 47.3 (143) | 44.7b |
| Retired or drawing a pension | 30.7 (92) | 28.6b |
| Housekeeping | 10.3 (31) | 16.2b |
| Other (primarily students) | 6.7 (20) | |
| Family income distribution (€ per month)d | ||
| Less than 1,000 | 23.2 (61) | 24.4c |
| 1,000–1,499 | 31.2 (82) | 20.9c |
| 1,500–1,999 | 24.0 (63) | 17.5c |
| 2,000–2,999 | 15.6 (41) | 22.4c |
| 3,000–3,999 | 5.3 (14) | 9.0c |
| 4,000 or more | 0.8 (2) | 6.1c |
| Lives alone | 7.3 (22) | |
| Friend or relative with alcohol problems | 20.0 (60) | |
| Personal consumption | ||
| Does not drink or drinks occasionally | 61.0 (183) | |
| Drinks weekly | 29.0 (87) | |
| Drinks daily or has drunk excessively | 10.0 (30) | |
| Health state (SF-6D mean) | 0.8 | |
| Duration of interview (minutes mean) | 24.3 | |
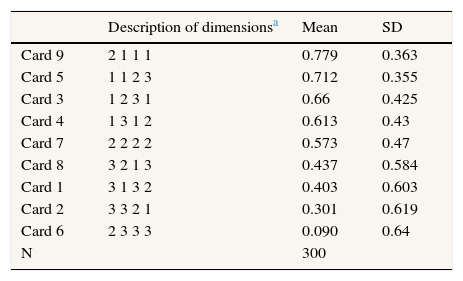
The first data column of Table 3 gives the mean utility for each of the nine cards. The difference in utility between the highest- and lowest-valued card was 0.69, a difference that indicates considerable heterogeneity among the various scenarios evaluated. All dominance tests were positive at the aggregate level, supporting internal consistency among responses. Means tests confirmed that the utility of card 9 was significantly greater than the utilities of cards 1, 2, 6, 7, and 8 and that the utility of card 6 was less than the utilities of cards 3, 4, 5, and 7 (p<0.001). For analyses at the individual level, 70% of the sample passed all dominance tests and 15.3% failed one test.
Mean utility of the scenarios directly evaluated.
| Description of dimensionsa | Mean | SD | |
|---|---|---|---|
| Card 9 | 2 1 1 1 | 0.779 | 0.363 |
| Card 5 | 1 1 2 3 | 0.712 | 0.355 |
| Card 3 | 1 2 3 1 | 0.66 | 0.425 |
| Card 4 | 1 3 1 2 | 0.613 | 0.43 |
| Card 7 | 2 2 2 2 | 0.573 | 0.47 |
| Card 8 | 3 2 1 3 | 0.437 | 0.584 |
| Card 1 | 3 1 3 2 | 0.403 | 0.603 |
| Card 2 | 3 3 2 1 | 0.301 | 0.619 |
| Card 6 | 2 3 3 3 | 0.090 | 0.64 |
| N | 300 |
SD: standard deviation.
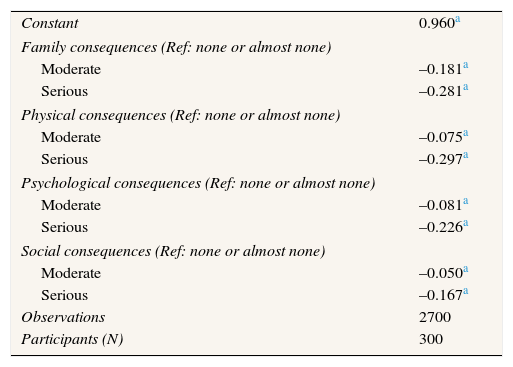
Table 4 shows the results of the regression. The coefficients for each level of a dimension indicate the lost utility incurred by being in that state as compared with having no (or almost no) problems in that dimension. As expected, having the least severe level in all dimensions yields a valuation close to 1 (the value of the constant). From the coefficients estimated, we can estimate the utility weight for any state. The values of all hypothetical scenarios range from −0.01 to 0.91. The results support our model's theoretical validity: the coefficients are significant and their signs are in the expected direction (more negative as the severity increases). The greatest reduction in utility resulted from serious physical health problems followed by serious family problems, serious psychological problems, moderate family problems, and serious social problems. The dimension with the greatest relative importance was physical health consequences (36.4%), followed by family consequences (31.3%), psychological consequences (20.5%), and social consequences (11.8%). In addition, we re-estimated model 1 (not shown) including the characteristics of the respondents shown in the Table 2. The coefficients for each level of dimensions were not affected. From the added variables, only labor status and having a close friend or relative with alcohol problems were statistically significant (being retired, being a homemaker and having a close friend or family member with alcohol problems reduced the mean utility).
Utility losses estimated from random-effects regression.
| Constant | 0.960a |
| Family consequences (Ref: none or almost none) | |
| Moderate | –0.181a |
| Serious | –0.281a |
| Physical consequences (Ref: none or almost none) | |
| Moderate | –0.075a |
| Serious | –0.297a |
| Psychological consequences (Ref: none or almost none) | |
| Moderate | –0.081a |
| Serious | –0.226a |
| Social consequences (Ref: none or almost none) | |
| Moderate | –0.050a |
| Serious | –0.167a |
| Observations | 2700 |
| Participants (N) | 300 |
Ref: reference group.
This paper estimates the impact of alcohol misuse on QoL, in terms of utility, based on general population preferences. It identifies four dimensions: physical, psychological, family and social. These dimensions are in line with the primary domains mentioned in the literature.22,33 The dimensions with the greatest importance were physical health consequences and family consequences. Table 3 shows a wide variation in the utilities associated with the nine profiles directly valued (from 0.09 to 0.78). The range is even greater when we predict the utility of remaining profiles.
There are other studies that directly estimate utilities for alcohol misuse profiles.24–26 However, the methodological differences make the comparisons difficult. Kraemer et al.’s study24 is the one most akin to ours: they evaluate hypothetical scenarios (although only two, “alcohol dependence” and “alcohol abuse”, are described as harming health, mood, social or family life), eliciting preferences from a sample of the general population and obtaining utilities in risk decision contexts. They estimate that the utility for “dependence” and “abuse”, using a standard gamble, were 0.67 and 0.75, respectively. Comparisons with other prior studies25,26 become even more dubious when one considers the marked differences in methodology (utilities obtained in a certainty context), the sample (a small sample of physicians) and the scenarios evaluated. Stouhard et al.26 assign (by interpolation) a utility weight of 0.89, 0.45 and 0.17 for “problem drinking”, “manifest alcoholism” and “psycho-organic disorder (delirium)”, respectively. Sanderson et al.25 assign a utility weight (using the time trade-off method) of 0.92, 0.83 and 0.66 for 3 levels of alcohol dependence (“a few symptoms”, “some symptoms” and “many symptoms”, respectively). In any case, the range of utilities estimated in our paper encompasses all other results in the literature.
This study is not free of limitations. First, although the objective of this study was to measure the intangible effects of alcohol misuse on QoL, those effects could have not been adequately isolated. The dimensions analyzed allude to intangible effects, but interviewees might still have considered the financial consequences (in particular, lost income and the cost of treatments). We attempted to isolate employment effects by asking interviewees to assume that the scenarios described by each card did not affect their income. With regard to the possible effect of treatment costs on responses, we believe that it is small or nonexistent because treatment for diseases associated with this pathology is free in the region where the sample population resides. Second, it is difficult to determine whether respondents were incorporating some scenario-specific externalities into their valuations. For example, in response to descriptions of deteriorating family relations, participants may have taken into account how it would affect the QoL of their family.34 Third, in this pilot study we select four main dimensions. Future research should evaluate whether these dimensions provide an adequate reflection of the adverse consequences of alcohol misuse or whether these dimensions ought to be split down into more specific items.
The utilities estimated could have both clinical and economic applications. They can be used in medicine as a supplemental tool for measuring the clinical course of a disease and its impact on family and social life. This study assumes that alcohol consumption and its harmful effects exist upon a very long continuum and therefore our results could be applied to evaluate the impact of different scenarios of alcohol misuse if relevant effects on QoL are already evident. Moreover, given that we estimate utility scores, our results can be used as part of the economic evaluation of programs aimed at reducing or preventing the harmful effects of alcohol, in conjunction with the values from more widely focused generic instruments. We obtain that family and social consequences are almost as important for society as are health consequences; therefore, ignoring these effects may lead to underestimating the impact of alcohol misuse. Future research should explore the possibility of designing and validating a specific QoL instrument for this population, in order to complement the poor sensitivity of generic instruments. It would be highly useful both to conduct comparative studies in different population groups and to analyze the effectiveness of different interventions aimed at this condition.
Alcohol-related disorders have multiple adverse effects on a drinker's quality of life. Studies addressing this issue, within the QALY framework, have focused on health-related effects on quality of life. Empirical evidence suggests these instruments may not be sensitive enough to detect significant changes in quality of life.
What does this study add to the literature?Using general population preferences as the base, we estimate the effects of alcohol misuse on quality of life in terms of utility. We identify four dimensions (physical, psychological, family and social) and estimate their relative importance. The utilities obtained can be used as a supplemental tool to measure the clinical course of the disease as well as to assess programs aimed at reducing or preventing the harms of alcohol on the quality of life.
Clara Bermúdez-Tamayo.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsE. Rodríguez-Míguez conceived the idea for the study and designed the questionnaire. J. Mosquera conducted the focus groups. Both authors contributed equally to the analysis and interpretation of results and writing of the paper.
FundingSpanish Ministry of Science and Innovation (grant ECO2011-25661) and Consellería de Economía e Industria - Regional Government of Galicia (grant no. 10SEC300038PR).
Conflicts of interestNone.
Questionnaire sequence and utilities associated with each outcome












