




The 3rd International Nursing and Health Sciences Students and Health Care Professionals Conference (INHSP)
More infoThis study aimed to compare serum levels of Insulin-like Growth Factor Binding Protein-3 in children with malnutrition and good nutritional status.
MethodThis cross-sectional study included 41 participants consisting of 31 malnourished, 10 well-nourished children aged between 36 and 60 months. Demographic data of participants were obtained utilizing a questionnaire. Nutritional status was determined by calculating the Z-score of body weight for age, height for age, and body weight for height indices using the WHO classification. IGFBP-3 levels were determined by the Enzyme-Linked Immunosorbent Assay (ELISA) method.
ResultMedian serum IGFBP-3 levels in malnourished children were found to be lower i.e. 0.35mcg/mL (minimum–maximum: 0.04–1.52mcg/mL) compared to well-nourished children 1.52ng/mL (minimum–maximum 0.47–3.17mcg/mL).
ConclusionSerum IGFBP-3 levels can be used as indicators to assess nutritional status.
Malnutrition in children under five years of age is one of the leading health problems in all countries.1 In addition, malnutrition is the leading cause of death, estimated to be about 45% of deaths in children aged 0–59 months.2
Nutritional problems in Indonesia are one of the main problems in human development. As one of the countries with a very diverse population complexity, Indonesia is faced with the dynamics of malnutrition. Although Indonesia's development process has been able to overcome the problem of nutrition, if seen from the trend of statistical data, there are still many problems that need to be assessed and resolved, especially those concerning under-nutrition.3
Malnutrition is a medical condition caused by insufficient intake, and this condition is often associated with malnutrition due to lack of food consumption, low absorption, or excessive loss of nutrients.4 Another impact of malnutrition is that apart from causing death, it also disrupts intelligence growth and development, where everyone who experiences malnutrition is reported to have a risk of losing IQ by 10–13 points.5 If the food intake for toddlers is insufficient, it will cause malnutrition. The toddler period is a period of very rapid growth and development. Toddlers over one year old have started to understand language and have a powerful sense of curiosity.
Lack of food or nutritional intake in children under five is caused by factors such as economic factors, education, knowledge, and food security. The family's economic status, classified as weak, causes a lack of community ability to provide nutritious food. If this continues for a long time, there will be chronic malnutrition in children, which will result in stunting. In addition, the education and knowledge of parents or caregivers greatly influence parenting styles. Good parenting can meet all toddlers to cause them to grow and develop optimally; on the other hand, poor parenting will interfere with toddlers’ growth and development.6
Average growth and development in children also depend on hormonal factors. Normal nutritional status is required for linear growth.7 Nutritional status plays an essential role in controlling GH and IGF-1 in circulation, regulating their work and delivery in body fluids and tissues. GH mediates growth, and IGF-1 as a mediator of GH action, bioavailability, and bioactivity of IGF-1 is modulated by the binding protein IGFBP-3.8,9
Nutritional deficiencies can affect GH signaling and lead to a state of GH resistance, resulting in higher systemic growth hormone levels and decreased IGF-1 and IGFBP-3 production. IGFBP-3 is the primary protein binding to IGF in serum and functions as a circulating IGF reserve. IGFBP-3 carries IGF-1 in the blood circulation, directs it to target tissues, protects it from proteolytic degradation, and regulates its interaction with IGF-1R. About 99% of IGF-1 in the blood circulation is mainly bound to IGFBP-3.8,9
The identification of the nutritional status of toddlers by examining the hormones involved in growth is still rarely used, and there is still a lack of knowledge and research on the examination of hormones involved in growth, even though the examination of the hormones involved in growth is an accurate test to determine the level of nutritional status.
Research methodsLocation and research designThis study used a cross-sectional study method, which is a design by measuring or observing variables simultaneously. This study aimed to determine the levels of IGFBP-3 in malnourished toddlers aged 36–60 months. This research was carried out by the Bara-Baraya Health Center in Makassar City, South Sulawesi, Indonesia.
Population and subjectThe population of this study was all toddlers aged 36–60 months. The sampling technique used in this study was simple random sampling with the subject in this study was 41 people consisting of well-nourished and malnourished toddlers aged 36–60 months. This study has received a recommendation of approval from the Ethical Commission for Health Research of Medical Faculty, Hasanuddin University Makassar with number 420/UN4.6.4.5.31/PP36/2020 and Protocol Number UH20050223.
Method and data analysisThe instruments used in this study were questionnaires and measuring levels of IGFBP-3. The questionnaire is data collection by providing a list of questions to the respondent to provide answers to all the questions listed. Measurement of levels of IGFBP-3 (Insulin-Like Growth Factor Binding Protein-3) using ELISA (Enzyme-Linked Immunosorbent Assay) at the Hasanuddin University RSP Research Laboratory Unit. Then, data analyzed using the Fisher exact and Mann–Whitney statistical test.
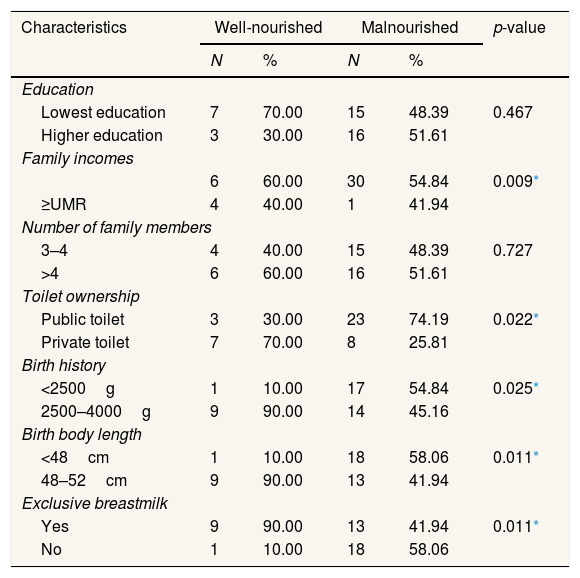
ResultsTable 1 shows the number of maternal education is low; family income is at most
Distribution characteristics of Respondents at Community Health Center (Puskesmas) Bara-Baraya Makassar (n=41).
| Characteristics | Well-nourished | Malnourished | p-value | ||
|---|---|---|---|---|---|
| N | % | N | % | ||
| Education | |||||
| Lowest education | 7 | 70.00 | 15 | 48.39 | 0.467 |
| Higher education | 3 | 30.00 | 16 | 51.61 | |
| Family incomes | |||||
| 6 | 60.00 | 30 | 54.84 | 0.009* | |
| ≥UMR | 4 | 40.00 | 1 | 41.94 | |
| Number of family members | |||||
| 3–4 | 4 | 40.00 | 15 | 48.39 | 0.727 |
| >4 | 6 | 60.00 | 16 | 51.61 | |
| Toilet ownership | |||||
| Public toilet | 3 | 30.00 | 23 | 74.19 | 0.022* |
| Private toilet | 7 | 70.00 | 8 | 25.81 | |
| Birth history | |||||
| <2500g | 1 | 10.00 | 17 | 54.84 | 0.025* |
| 2500–4000g | 9 | 90.00 | 14 | 45.16 | |
| Birth body length | |||||
| <48cm | 1 | 10.00 | 18 | 58.06 | 0.011* |
| 48–52cm | 9 | 90.00 | 13 | 41.94 | |
| Exclusive breastmilk | |||||
| Yes | 9 | 90.00 | 13 | 41.94 | 0.011* |
| No | 1 | 10.00 | 18 | 58.06 | |
Fisher exact.
To find out the differences in IGFBP-3 levels in malnourished and normal under-five children is essential; the Mann–Whitney statistical test was used because the data on IGFBP-3 levels were not normally distributed. The results of statistical tests showed that there were differences in IGFBP-3 levels in malnourished and typical toddlers (p<0.001) (Table 2). This indicates that Insulin-like Growth Factor Binding Protein-3 (IGFBP-3) levels are low in malnourished toddlers.
Differences in levels of IGFBP-3 in malnourished and well-nourished toddlers.
| Malnutrition status | Median (minimum–maximum) (mcg/mL) | p-value |
|---|---|---|
| Normal | 1.52 (0.47–3.17) | <0.001* |
| Malnourished | 0.35 (0.04–1.27) |
Mann–Whitney.
Based on the results of the Mann-Whitney test, it shows that there are differences in levels of Insulin-like Growth Factor Binding Protein-3 (IGFBP-3) in toddlers with normal nutritional status and toddlers with malnutrition nutritional status.
Toddler time needs adequate nutrition because the Toddler period is a golden period. A period of life that is very important for physical and mental development is when toddlers begin to do a lot and discover new things. In this case, good nutrition plays an important role.10 Regarding individual nutritional status, the GH and IGF-1 axis are the endocrine system principles that regulate linear growth in children. GH is a stimulator of IGF-I secretion and action11 and a significant regulator of IGFBP-3 production in humans. Apart from GH regulation, nutrition and age also play a role in regulating IGFBP-3 production.12
IGF-1 and IGFBP-3 serve as primary mediators of GH action and as GH-independent growth factors. Many studies have shown that GH and IGF-1 concentrations are responsive to nutritional status changes.13 IGFBP-3 is an IGF-1 carrier protein and regulates the bioavailability of IGF-1 so that it has a very close relationship.14 The function of IGF-1 is to metabolize food protein, energy, and carbohydrates13 and the growth of cartilage. When the amount of Insulin-Like Growth Factor-1 (IGF-1) secreted increases in response to Growth Hormone (GH) stimulation, there will be an increase in Insulin-Like Growth Factor Binding Protein-3 (IGFBP-3) to absorb it in the circulation. Low concentrations of IGF and IGFBP-3 can inhibit linear growth until body weight and height are stopped.11
Weight gain and linear growth were associated with IGF-1 and IGFBP-3.13 Malnutrition has a strong effect on IGF-I, IGFBP-3, and ALS,15 and reduced serum concentrations are influenced by nutritional status. Examination of serum levels of Insulin-Like Growth Factor-1 (IGF-1) and IGF-binding protein, namely IGFBP-3, can complement the growth status assessment to predict growth response.11
Adequate dietary intake is essential to maintain normal circulating levels of IGF-1 and IGFBP-3 in serum. Energy and protein restriction in children leads to decreased IGF-1 and IGFBP-3 levels. Smith et al. observed that calorie restriction led to decreased IGF-1 and IGFBP-3 in both adults and children. After nutritional rehabilitation, there was an increase in IGF-1 and IGFBP-3, but the increase was not significant or did not reach baseline levels.16
This study showed that the levels of IGFBP-3 in malnourished children were low, with a median (minimum–maximum) value of 0.35 (0.04–1.27)mcg/mL. This is in line with previous studies that have also shown that malnutrition decreases IGFBP-3 production. IGFBP-3 has been intensively studied in light of this protein's physiological role in acute changes in plasma glucose, IGF, and insulin levels. Secretion of IGF-1 is GH dependent and stimulated by an increase in blood glucose after feeding. The biological effects of IGF-1 are regulated by IGFBP-3, which is responsible for its transport in the blood.17
ConclusionA cross-sectional study has been conducted, and after statistical analysis, it can be concluded that IGFBP-3 levels are low in malnourished children under five and can be used as a parameter to assess nutritional status.
Conflicts of interestThe authors declare no conflict of interest.
Peer-review under responsibility of the scientific committee of the 3rd International Nursing, Health Science Students & Health Care Professionals Conference. Full-text and the content of it is under responsibility of authors of the article.











