




The 1st International Conference on Safety and Public Health
More infoThe objective of this study was to provide an overview of the equipment supporting Kangaroo Mother Care (KMC).
MethodThe review adopted a five-stage methodological framework that included research question identification, relevant study identification and selection, and data charting, collating, summarizing, and reporting. We conducted reviews to analyze the current research on the design of KMC-supporting devices. Publications were identified from January 2008 to July 2020.
ResultsUsing the inclusion criteria, 17 relevant studies were identified that concerned the design of supporting equipment for KMC. Five types of equipment improved the comfort of the mothers performing KMC, another five monitored the health and development of the infants, and four served as therapy for the infants. Three equipment types showed no significant effect in supporting KMC.
ConclusionsThis study provides information on equipment that effectively and efficiently improves the quality of KMC.
Kangaroo Mother Care (KMC) is the treatment of preterm infants by their mothers, who make skin-to-skin contact with the infants.1 KMC improves growth, reduces morbidity, and decreases the duration of hospitalization.2,3 It also increases the compatibility between the mothers’ and infants’ saliva levels 4and results in a significant improvement in vital physiological parameters.5 KMC is an alternative to conventional care; it is affordable, simple, acceptable, and feasible for the mothers.6–8
In KMC practices involving mothers, children, and health workers, a comprehensive approach is needed. One important aspect involves the devices that support this activity and enable it to run effectively and efficiently. The availability of devices and other items that support KMC depends on the commitment from hospital directors and senior staff.9 The appropriate equipment or devices can overcome problems related to safety, health, and efficiency by improving the conditions under which the KMC activities are conducted.10 The aim of the present study was to provide an overview of the equipment currently available to support continuous KMC, focusing on the ability of the equipment to extend the duration of the KMC, maintain the mother's comfort, and support the growth and development of low-birthweight infants.
MethodThis review adopted a five-stage methodological framework that included: 1) identification of the research question, 2) identification of relevant studies, 3) study selection, 4) charting the data, and 5) collating, summarizing, and reporting on the results of the studies.11 In the first stage, we developed the following research question: What is the extent of the information available regarding the devices available to support continuous KMC? We then established the keywords for our search strategy by combining relevant keywords (“kangaroo mother care” OR “kangaroo care” OR “kangaroo-mother care” OR KMC) AND (equipment OR device OR appliances).
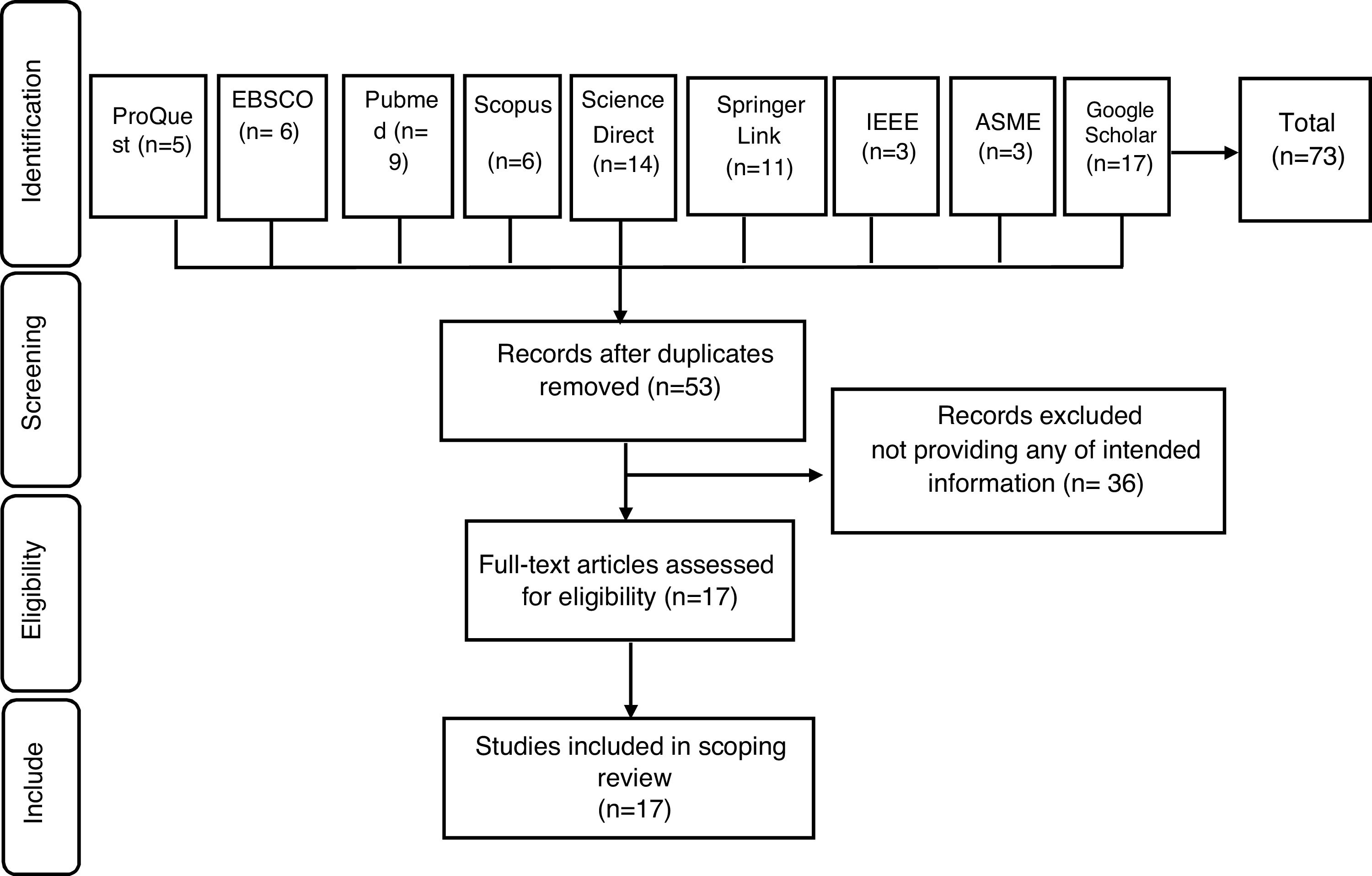
In the second stage, involving identification of relevant studies, we searched for research evidence using Medline with the full-text EBSCO, Scopus, Science Direct, ProQuest, PubMed, Springer Link, IEEE, AMSE, and Google Scholar databases. Only articles written in English and Indonesian and published between January 2008 and July 2020 were included. Bibliographies were searched by hand to include other studies that related to our topic. This searching mechanism produced a total of 161 references. These articles were then screened and were included in the study if they met the following criteria: a) the documents were published in an academic journal or proceedings; b) they described at least one of the following: KMC, Kangaroo care, appliances, products, or equipment; c) they were conducted anywhere around the world; and d) they were either quantitative or qualitative studies. This screening yielded 73 articles for possible inclusion in the study.
In the data charting stage, we recorded information about the author(s), country, study design, setting, subject (sample), intervention, and outcome. In the collating, summarizing, and reporting stage, we provided an overview of the reviewed material that related to devices that supported KMC.
ResultsStudy search and selectionOur search of the literature identified 73 studies in the identification step. After duplicates were removed, only 53 studies remained. Of these, 36 articles were excluded because they did not provide information on the topic of interest. Ultimately, 17 studies met all the inclusion criteria and were selected for data extraction (Fig. 1).
Effect of devices on the support of KMC
Most of the studies showed a positive effect of the equipment that supported KMC. Some equipment was meant to improve the comfort of the mothers in performing KMC 12–18Some equipment designs were aimed at monitoring the health and development of the infants.19–23 Some equipment also serves as therapy for infants.24,25 Three other studies showed less significant effects in supporting KMC 26–28(Table 1).
Outcomes for equipment designed to support Kangaroo Mother Care (KMC).
| Author, country | Setting, subject (sample) | Equipment | Outcome |
|---|---|---|---|
| Schets et al. (2015),Netherlands | Hospital,preterm infants | Breathing mattress | The mattress is easy to clean, comfortable, and mimics the breathing movements of the parent's chest |
| Thapa et al. (2018),Nepal | Hospital and post discharge (home),mother | Ergonomic baby wrap | Ergonomic wrap is easy to use without assistance, safe and flexible to movements in the KMC positions |
| Kommers et al. (2017),Netherlands | Hospital,preterm infant | Heart rate variability (HRV) features | Feature of heart rate variability (HRV) is useful for knowing the response of dynamic changes to KMC and to other changes in various conditions |
| Kommers et al. (2018),Netherlands | Hospital,preterm infants | BabyBe GMBH, Stuttgart, Germany | Mattress products that mimic the breathing movements and the sound of the mother's heartbeat do not affect the baby's HRV |
| Norouzi et al. (2013),Iran | Hospital,mothers who were delivered by C-section | Music for maternal anxiety state | The music intervention during KMC had no significant effect on maternal anxiety states |
| Joglekar et al. (2018),India | Hospital,mother, caregiver, and neonates | Wearable sensor | Wearable sensor as a device to measures the temperature and relative position of neonates during KMC. It is equipped with a skin touch sensor to meet the requirements of temperature reading |
| Jimenez et al. (2016),Peru | Hospital,mannequins of neonates | Blue light emitting diode phototherapy device | Device with blue light diode phototherapy can be used for phototherapy. To facilitate contact between mother and infants, a mattress with LEDs should be placed on the infant's back |
| Rao et al. (2018),India | Hospital,mothers and neonates | Wearable sensor | The sensors can be used to track KMC compliance and newborn temperature in a safe manner for a few days or during hospitalization and the home phase |
| Milette et al. (2015),Canada | Hospital,mothers | Zero gravity chairs | The use of zero gravity chairs has good impact to increase frequency and duration of KMC, by increasing the mothers’ comfort. In addition, the use of this chair allows better blood flow to the extremities and reduces edema |
| Weber and Clarke-Sather (2019), USA | Hospital, mothers and infants | Sensor for tracking of infant-mother during KMC | The sensor can accurately measure the duration of KMC implementation. It is estimated that this technology can be utilized to track and map KMC in NICU room |
| Clarke-Sather and Naylor (2019) | Hospital,mothers | breastfeeding wearables | Equipment such as pumping bras make it easier for mothers to pump breast milk and even increase milk production because it massages the breast when pumping |
| Kommers et al. (2019), Netherlands | Hospital,mothers and infants | Swaddling Device for Baby (Hugsy) | A swaddling device (Hugsy) has the ability to absorb the warmth and scent of parents during KMC and is then transferred back to the incubator. However, this device did not show any increase in neonatal autonomous regulation measured in the form of vital signs and heart rate variability |
| Jimenez et al. (2017), Peru | Hospital,mothers and infants | Phototherapy mattress with bluelight emitting diodes (LEDs) | Phototherapy mattress is intended for jaundice therapy for neonates. This device has an effective thermal capacity of 6.4W. The thermal conductivity of this device has been calculated through limited experiments in a polystyrene spheroid |
| Jagadish et al. (2018), India | Hospital,mothers and infants | Hypothermia alert device | Hypothermia alert is an effective device for increasing parental adherence to KMC and supporting neonatal weight gain |
| Sari and Listiarini (2018), Indonesia | Mothers and infants | Support binder (long cloth of batik/jarik) | The effectiveness of KMC with a support binder (a long cloth of batik/jarik) is proportional to the use of incubators in increasing low birthweight babies |
| Chavula et al. (2020), Malawi | Hospital,mothers and infants | Customized Baby Wrap | This device contributes to support better skin-to-skin contact between mothers and infants. In practicing Kangaroo care, the use of a customized wrap is one mechanism in addition to other treatments |
| Cavallin et al. (2018), Mozambique-Ethiopia-Uganda | Hospital,mothers and infants | Woolen Cap | Although the use of a woolen cap is safe for neonates, it does not make a significant contribution to maintenance of the normal thermal range in low birthweight infants. During KMC, low birthweight babies spend only half their time in the normal temperature range |
The basic KMC unit must meet a minimum number of requirements, namely the availability of space for beds or armchairs for mothers or families, good sanitation and hygiene, clean water facilities, environmental modifications to facilitate the transition from hospital to home, nurse or midwife rooms for documentation, and equipment that supports breastfeeding.9 However, one of the barriers in the implementation of KMC is a lack of facility readiness, including supporting devices for practicing KMC.29–31
The results shown in the selected articles indicate that the availability of support equipment increases the effectiveness and efficiency of KMC implementation. Most of the equipment had a positive impact on mothers, babies, and nurses. However, little is known about the ergonomic aspects of this equipment. Ergonomics in health care, and especially in KMC, is pivotal. Numerous health care studies have shown a positive impact on the quality of patient safety and quality of care following the application of ergonomic interventions32–36
The ergonomic aspect of the equipment can help mothers maintain their normal and comfortable posture, which can extend the duration of the KMC and thereby support the growth and development of the low-birthweight infants. This certainly supports continuous KMC, because the longer a person maintains skin-to-skin contact, the faster is the growth and development of low-birthweight infants.37
Ergonomics is the scientific discipline concerned with the understanding of interactions among humans and other elements of a system.38 In health care settings, ergonomics consists of three areas. First is physical ergonomics, which is concerned with physical activity and includes the design of health care facilities, equipment used in health care, and patient spaces that consider the patients’ physical strength and limitations. The second is cognitive ergonomics, which is related to psychological processes, including interface designs that can be used for health information technologies and other programs, such as training. The third is organizational ergonomics, which is related to the overall work design system in an organization or a sociotechnical system and the interaction of various elements in the system, including the working hours of health care workers.39
Health equipment with a physical ergonomic approach is needed to avoid various health complaints of mothers and of health care workers. One issue is musculoskeletal complaints experienced by health care workers when conducting medical interventions on patients. Musculoskeletal complaints also can be felt by mothers, caused by factors such as the unnatural position of the mother and the health care staff during KMC. The body position when performing KMC activities is analogous to that when working. The unnatural body position is generally due to the demands of the task and to the use of equipment, including chairs or sofas, that is not suitable for mothers doing KMC.40,41 Ergonomics is therefore very useful for analyzing, preventing, and mitigating medical errors. An ergonomic work style is recommended to reduce musculoskeletal complaints,42,43 included those occurring during KMC.
In KMC, the design of equipment can facilitate or simulate various aspects of KMC by exposing infants to parental stimuli or parents and infants to familiar stimuli, and through designs that facilitate communication between the parent and the infant. KMC is beneficial for enhancing the bonding between the parent and infant.10,44
Limitations of the StudyThis study only considered the equipment developed over the past 10 years. The search was limited to English and Indonesian languages, so other research that relates to the devices that support KMC may also be present in other databases.
ConclusionsThis study provides information about equipment that supports KMC. Most of the equipment is effective and efficient and improves the quality of KMC.
RecommendationsFurther research into the use of an ergonomic sofa to improve the sitting posture and reduce the risk of musculoskeletal complaints among mothers performing KMC is urgently needed to extend the duration of KMC and maintain the mother's comfort.
Ethical approvalThe study design and procedures were approved by the Research Ethics Committee of the Faculty of Public Health, Universitas Indonesia (Approval number: 668/UN2.F10//PPM.00.02/2019).
Conflicts of interestThe authors declare that they have no conflicts of interest in this study.
We thank the Directorate of Research and Community Engagement of Universitas Indonesia for providing funds for this study. (Grant No: NKB-0140/UN2.R3.1/HKP.05.00/2019).
Peer-review under responsibility of the scientific committee of the 1st International Conference on Safety and Public Health (ICOS-PH 2020). Full-text and the content of it is under responsibility of authors of the article.











