




To measure and assess differences by educational level in the place of death for cancer patients, and to determine whether patterns of geographical disparities are associated with access to palliative care services in the municipality of residence.
MethodWe analysed the death certificates of adults (older than 24) who died of cancer (ICD-10 C00 to C97) in Spain during 2015, either at home, in hospital or in a long-term care centre. Of the 105,758 individuals included in the study population, 75.2% lived in one of the 746 identifiable municipalities (more than 10,000 inhabitants). This individual database was combined with three economic databases at municipal level and with a directory of palliative care resources published by the Sociedad Española de Cuidados Paliativos. Multilevel models were estimated to predict the place of death according to individual characteristics. Generalised least squares regression models were then applied to the municipal effects estimated in the first stage.
ResultsThe probability of dying in long-term care centre decreases as levels of education increase; the probability of dying at home, rather than in hospital, is higher for patients with higher education. Dying in hospital is an urban phenomenon. There are large differences between Spanish regions. Access to palliative services is only of marginal significance in accounting for the systematic differences observed between municipalities.
ConclusionsDeveloping specific plans for palliative care, with an active role being played by primary care teams, may help improve end-of-life care in Spain.
Medir y evaluar las diferencias por nivel educativo respecto al lugar de muerte de pacientes con cáncer en España, y determinar si los patrones de desigualdad geográfica están asociados con el acceso a servicios de cuidados paliativos en el municipio de residencia.
MétodoAnalizamos los certificados de defunción de mayores de 24 años que murieron de cáncer (CIE-10 C00-C97) en España durante 2015, en el hogar, en el hospital o en una residencia sociosanitaria. Sobre una población total de 105.758 personas, el 75,2% vivía en uno de los 746 municipios identificables (más de 10.000 habitantes). La base de datos individual se combina con datos económicos de ámbito municipal y con el directorio de recursos de cuidados paliativos publicado por la Sociedad Española de Cuidados Paliativos. Se estiman modelos multinivel para predecir el lugar de la muerte de acuerdo con las características individuales. A continuación, se estiman modelos de regresión por mínimos cuadrados generalizados sobre los efectos municipales estimados en el modelo anterior.
ResultadosLa probabilidad de morir en casa, frente al hospital, es mayor en los pacientes con educación superior. Morir en el hospital resulta un fenómeno urbano. Hay grandes diferencias entre regiones. El acceso a los servicios paliativos solo tiene una importancia marginal en la explicación de las diferencias entre municipios.
ConclusiónEl desarrollo de planes específicos para cuidados paliativos, con un papel más activo de los equipos de atención primaria, puede ayudar a mejorar la atención sanitaria al final de la vida en España.
Very few studies have addressed the question of the quality of death, despite the fact that this is, and has always been, a major concern to humanity.1–3 When an incurable disease is diagnosed, as well as treating the symptoms presented, plans should be made for providing health care in the terminal phase. There is evidence that factors such as early palliative care and the control of symptoms are strongly associated with a better quality of death.4
It is known that most patients with advanced cancer prefer to die at home.5–17 In Europe, according to a random sampling study of the general population of seven countries,8 more than half would prefer to die at home (in Spain, 66%). There is no evidence that the educational level of patients with terminal cancer is associated with their preference for the place of death. In this respect, preferences are associated with other factors, such as religious beliefs, personal values or the duration of the illness.8
Nevertheless, the majority of deaths by cancer patients occur in hospitals,9,10 where the quality of death may be worse.11 Many patients whose death was foreseeable on admission die after invasive diagnostic and therapeutic actions, while psychological, social and family needs, which can be as important as physical ones, or even more so, are ignored.12
There are three main places of death: at home, in hospital and in a long-term care centre (LTCC). Among them, the distribution of cancer deaths presents large variations between and within countries. A study conducted in six European countries reported that better chances of dying at home are associated with solid cancers, being married, higher educational attainment and living in less urbanised areas.10 Many studies have identified predictors of death at home, of which the most influential is the presence of an informal caregiver. In addition, the accessibility of palliative care services in the community at affordable cost is a significant prognostic factor, which might account for the large differences found between countries.14 Access to community palliative services is not homogeneous by socioeconomic groups: thus, it has been reported that “patients in higher socioeconomic groups were both more likely to die at home and to access home care”.15 Since the 1980s, the highest frequencies of deaths at home have corresponded to patients with higher levels of education;16 similar findings have been reported in Spain.17 One explanation for this could be that areas with higher socioeconomic status have more palliative care services available.18–20 In Italy, the territorial differences between 13 provinces in the proportions of deaths at home persist even after adjusting for individual characteristics and context, which suggests there are systematic differences in access to palliative services.21,22
Spain provides an interesting case study. It has a universal, free-of-charge national health system and an expanding specialised network of palliative care, following a national palliative care strategy that has been updated for the period 2010-2014. Accordingly, it might be expected that there would be no major personal or territorial differences in the quality of death or systematic differences in the place of death due to cancer, among patients or municipalities. But as a matter of fact, the development of palliative care differs substantially between regions.23,24. The Spanish Society for Palliative Care (SECPAL) produces a standardised, detailed record of available infrastructure, human and organisational resources, providing a basic source of information.24 There are important differences between autonomous communities in Spain in the allocation, organisation and management of palliative care resources.25 Some regions have special plans for socio-health care and/or palliative care, following the guidelines of the National Strategy for Palliative Care that was launched nationally in 2006. That is the case of Catalonia, where palliative care is integrated in the strategy of social and long term care26 and Basque Country, which have defined a plan coordinating primary and specialized resources.27 Palliative medicine is not a medical specialty and the variability among health areas and regions in the organization of end-of-life care is noticeable, particularly regarding the role of primary care versus hospital care.
The main study aim is to examine individual and territorial variations in relation to the place of death due to cancer in Spain. To our knowledge, no previous studies have been conducted to analyse territorial variations in the place of death (home, hospital or LTCC) due to cancer using population data, including education among individual determinants.
MethodsStudy design, sources of information and variablesThis is a retrospective, cross-sectional, observational study. We used the nationwide register of death certificates issued in Spain during the period January to December 2015. The data are structured in two levels: individual (level 1) and the municipality of residence (level 2). At the individual level, we analysed the anonymised data from the population cause of death register in Spain during 2015 (National Institute of Statistics). We included all patients older than 25 years who died of cancer (ICD-10 codes C00 to C97) in a stated place (hospital, home or LTCC) in Spain, and lived in a municipality with more than 10,000 population (n=79,506). The individual database contains the detailed cause of death (ICD-10), place of death, educational level, sex, age, marital status and municipality of residence. Municipalities with fewer than 10,000 inhabitants were censored to guarantee anonymity (it is only known that the decedent lived in a small municipality, not in which one). Patients whose place of death were not stated or were other than the home, a hospital or a LTCC were also excluded (n=4964). Of the remaining 105,758 individuals, 79,506 (75.2%) lived in an identifiable municipality (of over 10,000 inhabitants) among the 746 municipalities comprising those included in level 2 (see Fig. I in the Appendix online). The models are estimated for these 79,506 individuals. The analysis of robustness included all individuals who died of cancer, whether or not the municipality of residence was known.
The above-mentioned register of deaths was combined with three economic databases for municipalities and a fourth database created from the directory of palliative care resources. The economic databases were obtained from the following sources: 1) social security archives: monthly data of the number of affiliates, averaged for the year, by type of affiliation (agriculture, see workers, social security general scheme); 2) Tax agency files: highly detailed tax data, including income tax; 3) Ministry of Public Administration files: detailed municipal budgets. The latter two databases exclude the municipalities of the Basque Country, which has a special fiscal regime.
Based on the 2015 Directory of Palliative Care Resources in Spain, published by SECPAL,24 we constructed a municipal database describing the physical, human and organisational resources available in the municipality, including public and private facilities: number of units and personnel, by type, of palliative care, providing services at home, in hospital and/or in a LTCC. The location and characteristics of each resource or care unit were recorded.
To measure the difficulties of access to palliative care at home, data for travel time were obtained from the Google Maps Distance Matrix Application Program Interface (Google Maps API) using the R package googleway,28 calculating the distance in travel time by car from the headquarters of the palliative home-care facility closest to the centre of the municipality of residence of the dying patient. A lack of access to palliative home-care services is defined as residence in a municipality without palliative home-care when the nearest resource, according to the SECPAL directory, is more than an hour's drive away. The study variables are defined in Table 1.
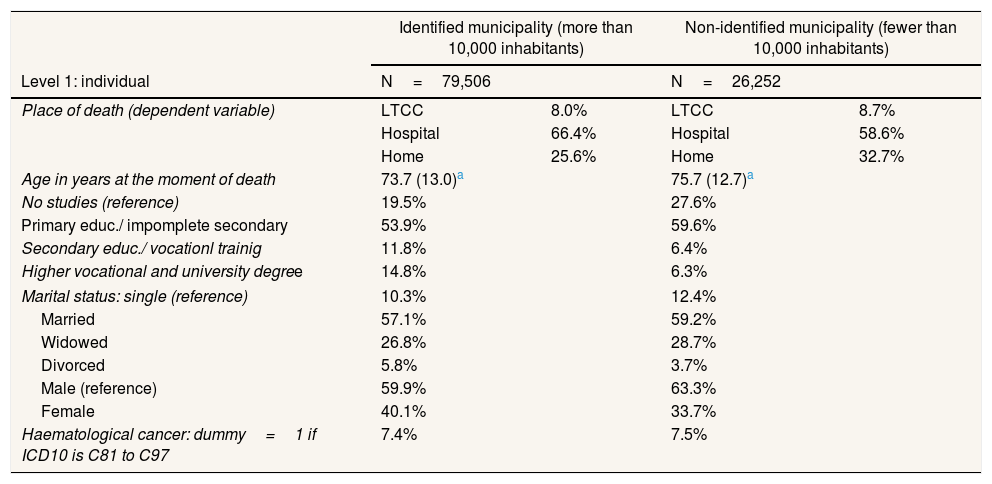
Univariate statistical description and frequencies of the variables in identified and non-identified municipalities.
| Identified municipality (more than 10,000 inhabitants) | Non-identified municipality (fewer than 10,000 inhabitants) | |||
|---|---|---|---|---|
| Level 1: individual | N=79,506 | N=26,252 | ||
| Place of death (dependent variable) | LTCC | 8.0% | LTCC | 8.7% |
| Hospital | 66.4% | Hospital | 58.6% | |
| Home | 25.6% | Home | 32.7% | |
| Age in years at the moment of death | 73.7 (13.0)a | 75.7 (12.7)a | ||
| No studies (reference) | 19.5% | 27.6% | ||
| Primary educ./ impomplete secondary | 53.9% | 59.6% | ||
| Secondary educ./ vocationl trainig | 11.8% | 6.4% | ||
| Higher vocational and university degree | 14.8% | 6.3% | ||
| Marital status: single (reference) | 10.3% | 12.4% | ||
| Married | 57.1% | 59.2% | ||
| Widowed | 26.8% | 28.7% | ||
| Divorced | 5.8% | 3.7% | ||
| Male (reference) | 59.9% | 63.3% | ||
| Female | 40.1% | 33.7% | ||
| Haematological cancer: dummy=1 if ICD10 is C81 to C97 | 7.4% | 7.5% | ||
| Level 2: municipality | N=746 | |
|---|---|---|
| Persons affiliated to the agricultural Social security system as a percentage of total affiliates | 6.5% | _ |
| Capital: dummy=1 for provincial or island capital | 7.1% | _ |
| Dummies for the autonomous communities with over 40 municipalities | _ | |
| Andalusia | 20.6% | |
| Canary Islands | 5.6% | |
| Catalonia | 16.0% | |
| Valencia | 13.1% | |
| Galicia | 7.5% | |
| Madrid | 6.6% | |
| Basque Country | 5.4% | |
| Dummy = 1 if the municipality provides palliative services in LTCCsb | 10.7% | _ |
| Dummy = 1 if the municipality provides palliative services in hospitalsb | 11.3% | _ |
| Dummy = 1 if the municipality provides palliative services in patients’ homesb | 13.5% | _ |
| Dummy = 1 if the municipality provides palliative services only in LTCCsb | 0.3% | _ |
| Dummy = 1 if the municipality provides palliative services only in hospitalsb | 2.3% | _ |
| Dummy = 1 if there is no access to home-based palliative services less than one hour's drive awayb | 6.8% | _ |
LTCC: long-term care centre.
The econometric analysis consisted of two separate, sequential regression models. In the first stage of the analysis, we created multilevel linear probability models to estimate the probability of a person dying in a LTCC vs. at home or in hospital (model 1, M1), dying in hospital vs. at home or in a LTCC (model 2, M2) and dying at home vs. in hospital (model 3, M3):

In equation [1] the dependent variable Y is a dummy 0/1 variable identifying the place of death (= 1 for LTCC in M1,=1 for hospital in M2 and=1 for home in M3) of individual i living in municipality j. M3 excludes from sample those persons dying in a LTCC. The individual explanatory variables (X) are the personal characteristics identified in the literature, age, sex, haematological cancer, educational level (in four ordinal categories, from no studies to higher education) and marital status. The error has two components, the municipality effect γj, which represents the difference in the probability of dying in the place tagged with Y=1 between the municipality j and the global sample, and the individual error ɛij, which is assumed to be independent of γj.
An advantage of the probability model is its metric, since it directly supplies the estimated average probability of a patient dying at home for each municipality, which will be used as the endogenous variable of the second regression. Table I in Appendix online contains the result of the multinomial logistic regression model for dying at home and in a LTCC with the most frequent category (hospital) as reference.
From models in equation [1] we estimate the intra-group correlation, which approximates the proportion of the error variance that is attributable to the municipality.
The next step in the process is to calculate the posteriori Bayesian predictor for each municipality, γˆj (municipality effect) and its estimated standard deviation (sd_municipality effect).
In the second stage of the analysis, the municipality effect is regressed against relevant socioeconomic characteristics of the municipality and variables for accessibility to palliative care services (equation [2]). In addition, fixed effects are included for the autonomous communities that contain more than 40 municipalities in the sample. We use weighted least squares regression, defining the weights with the sd_municipality effect estimated in stage 1. In the robustness analysis, the weights are defined alternately with the number of cancer deaths in the municipality.

The strategy in two steps allows us to separate the individual factors from the territorial factors influencing the place of death.
As an additional proof of robustness, we evaluated the same models for 2014 and compared the results.
ResultsTable 1 presents the descriptive statistics for the total number of deaths due to cancer, differentiating according to whether the municipality of residence is identified or not. It also describes the municipal variables finally included in the models.
In large and medium-sized municipalities, 25.6% of deaths caused by cancer die at home, compared to 32.7% in small municipalities. Dying in hospital is more frequent in municipalities of more than 10,000 inhabitants (66.4% vs. 58.6%), while dying in a LTCC is very uncommon in Spain, the incidence being slightly higher among residents of small municipalities. There are other differences by size of place of residence: decedents in small municipalities tend to be older, there is a higher proportion of men and widowers in the population and a lower proportion of residents have higher education qualifications.
There are also large variations among identifiable municipalities in the percentage of cancer deaths at home. Counting only the municipalities that recorded more than 100 deaths from cancer in 2015, the raw data show an enormous range of variation, from 6.7% to 57.0% in the proportion of home deaths. Deaths in LTCCs range from 0% to 33.1% of the total, and those in hospital, from 39.3% to 90.5%.
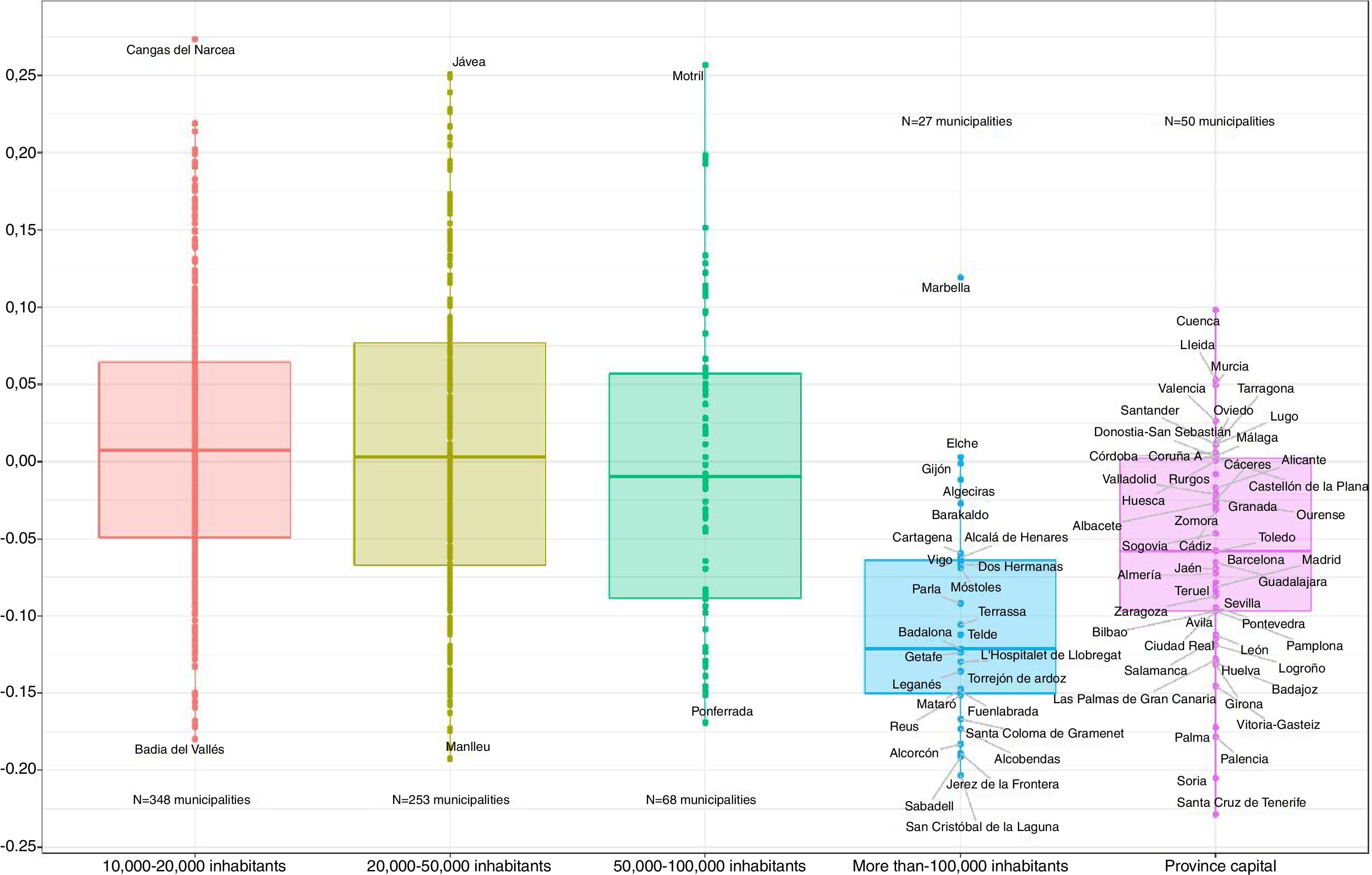
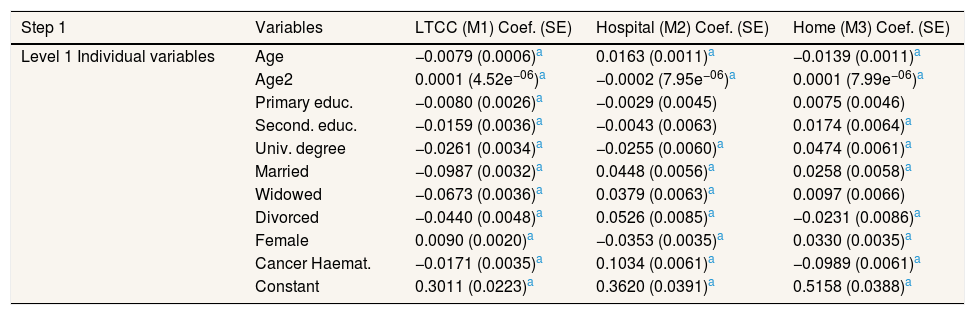
The multilevel models with individual data and municipality effects clearly show that education is a very significant prognostic factor of the place of cancer death (Table 2). Thus, when the patient has higher education qualifications, the probability of dying at home vs. in hospital is increased by 0.047 compared with individuals without studies. The probability of dying in a LTCC decreases monotonically by education level. The other explanatory variables are very significant, in particular haematological cancer, but also sex and marital status, with the expected signs: female have a higher probability to die at home than male as the mainstream of the literature finds; the same stands for married patients. It is more probable for a female to die at home than for a male (0.033). Figure 1 represents the estimated municipal effects by size of population (10,000-20,000, 20,000-50,000, 50,000-100,000, larger than 100,000 and capitals of province irrespectively their population size). The municipal effects are very significant and represent 8.6% of the residual variance for death in LTCCs, 6.23% for death at home and 5.97% for death in hospital. That means that some characteristics of the municipality are influencing systematically the place of death even though it may be not possible to identify those characteristics to include them explicitly in the model. The municipality effects account for the “unobserved heterogeneity” among municipalities.
Estimation results. Step 1. Multilevel linear probability model for place of death in 2015.
| Step 1 | Variables | LTCC (M1) Coef. (SE) | Hospital (M2) Coef. (SE) | Home (M3) Coef. (SE) |
|---|---|---|---|---|
| Level 1 Individual variables | Age | −0.0079 (0.0006)a | 0.0163 (0.0011)a | −0.0139 (0.0011)a |
| Age2 | 0.0001 (4.52e−06)a | −0.0002 (7.95e−06)a | 0.0001 (7.99e−06)a | |
| Primary educ. | −0.0080 (0.0026)a | −0.0029 (0.0045) | 0.0075 (0.0046) | |
| Second. educ. | −0.0159 (0.0036)a | −0.0043 (0.0063) | 0.0174 (0.0064)a | |
| Univ. degree | −0.0261 (0.0034)a | −0.0255 (0.0060)a | 0.0474 (0.0061)a | |
| Married | −0.0987 (0.0032)a | 0.0448 (0.0056)a | 0.0258 (0.0058)a | |
| Widowed | −0.0673 (0.0036)a | 0.0379 (0.0063)a | 0.0097 (0.0066) | |
| Divorced | −0.0440 (0.0048)a | 0.0526 (0.0085)a | −0.0231 (0.0086)a | |
| Female | 0.0090 (0.0020)a | −0.0353 (0.0035)a | 0.0330 (0.0035)a | |
| Cancer Haemat. | −0.0171 (0.0035)a | 0.1034 (0.0061)a | −0.0989 (0.0061)a | |
| Constant | 0.3011 (0.0223)a | 0.3620 (0.0391)a | 0.5158 (0.0388)a |
| Random effects parameters | Estimate (SE) | |||
|---|---|---|---|---|
| Municipal effects variance | 0.0061 (0.0004) | 0.0127 (0.0009) | 0.0123 (0.0009) | |
| Individual error variance | 0.0649 (0.0003) | 0.2007 (0.0010) | 0.1847 (0.0010) | |
| Intraclass correlation (%) | 8.60% | 5.97% | 6.23% | |
| N°. of obs. | Level 1 | 79,506 | 79,506 | 73,126 |
| N°. of groups | Level 2 | 746 | 746 | 746 |
LTCC: long-term care centre; SE: standard error.

Municipality effects estimated with multilevel model M3 dying at home vs. in hospital by size of municipality. The average of all municipalities in sample is 0. In municipalities with positive sign dying at home is more frequent than for average, in municipalities with negative sign dying in hospital is more frequent than for average. Province capital includes all capitals irrespective of their population size.
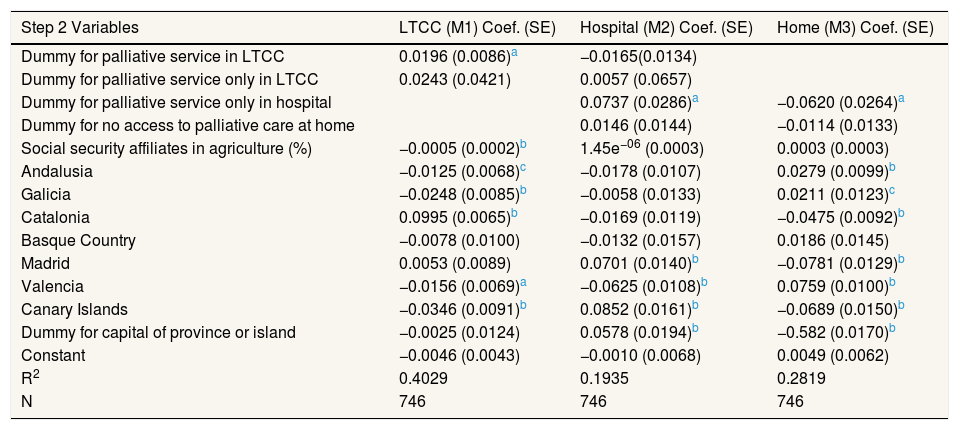
The second-stage models (Table 3) find that dying in hospital is more likely in provincial or island capital cities. Significant effects, which provide the highest standardised coefficients, were recorded for some of the 17 autonomous communities; especially noteworthy were the facts that death in a LTCC is associated with Catalonia, death in a hospital, with Madrid and the Canary Islands, and death at home, with Andalusia and Valencia.
Estimation results. Step 2. Modelling municipal effects in 2015, weighted least squares estimation.
| Step 2 Variables | LTCC (M1) Coef. (SE) | Hospital (M2) Coef. (SE) | Home (M3) Coef. (SE) |
|---|---|---|---|
| Dummy for palliative service in LTCC | 0.0196 (0.0086)a | −0.0165(0.0134) | |
| Dummy for palliative service only in LTCC | 0.0243 (0.0421) | 0.0057 (0.0657) | |
| Dummy for palliative service only in hospital | 0.0737 (0.0286)a | −0.0620 (0.0264)a | |
| Dummy for no access to palliative care at home | 0.0146 (0.0144) | −0.0114 (0.0133) | |
| Social security affiliates in agriculture (%) | −0.0005 (0.0002)b | 1.45e−06 (0.0003) | 0.0003 (0.0003) |
| Andalusia | −0.0125 (0.0068)c | −0.0178 (0.0107) | 0.0279 (0.0099)b |
| Galicia | −0.0248 (0.0085)b | −0.0058 (0.0133) | 0.0211 (0.0123)c |
| Catalonia | 0.0995 (0.0065)b | −0.0169 (0.0119) | −0.0475 (0.0092)b |
| Basque Country | −0.0078 (0.0100) | −0.0132 (0.0157) | 0.0186 (0.0145) |
| Madrid | 0.0053 (0.0089) | 0.0701 (0.0140)b | −0.0781 (0.0129)b |
| Valencia | −0.0156 (0.0069)a | −0.0625 (0.0108)b | 0.0759 (0.0100)b |
| Canary Islands | −0.0346 (0.0091)b | 0.0852 (0.0161)b | −0.0689 (0.0150)b |
| Dummy for capital of province or island | −0.0025 (0.0124) | 0.0578 (0.0194)b | −0.582 (0.0170)b |
| Constant | −0.0046 (0.0043) | −0.0010 (0.0068) | 0.0049 (0.0062) |
| R2 | 0.4029 | 0.1935 | 0.2819 |
| N | 746 | 746 | 746 |
LTCC: long-term care centre; SE: standard error.
Note: weights defined by standard deviation of the municipal effects obtained in step 1.
According to the results of the models, the availability of palliative care services is only marginally significant, but always with the expected signs: the more availability of home services, the higher the probability to die at home. Death in a LTCC is more likely if palliative care services are provided at LTCCs in the municipality, while death at home is less likely if the only palliative services available are hospital-based. The lack of access to palliative services at home is not significant in the model.
The robustness tests with data for 2014 and identical models show similar results. The municipal effects obtained in the first stage in both years independently show a linear correlation of over 0.7 in all cases (0.81, 0.73 and 0.72 for models 1, 2 and 3 respectively).
DiscussionAccording to our results the place of death for patients suffering cancer is related to the municipality of residence, education and gender. Dying of cancer in hospital is an urban phenomenon while home deaths are more frequent in rural municipalities.
Male die more frequently in hospitals, women do it at home. This result is in accordance with the mainstream of the literature, which systematically finds a higher diagnostic and therapeutic intensity for male.29 Our results coincide with those obtained for other countries, such as France,30 on the influence of education and marital status on the place of death. Some studies conducted in countries where there is universal free-of-charge access to the public health service suggest that more highly educated patients may obtain a better quality of death, perhaps due to their greater competence in navigating the system.31,32 If this were so, there could be a need for measures to facilitate access to the system and to eliminate non-monetary barriers. These barriers might be due to the fact that the homes of people with low educational level do not meet the minimum conditions to receive palliative care in them. If that is the case, the barriers might be counteracted by the intervention of social-health liaison officers. More highly educated people might obtain greater access to home-based palliative care at the end of life either because they reside in areas with better provision, or because they are better equipped to navigate through the administrative system or because the conditions of their homes facilitate it. Such inequalities would occur even within public, universal, free of charge health systems. Thus, the barriers are not institutional.
The finding that dying of cancer in hospital is an urban phenomenon while home deaths are more frequent in rural municipalities is robust. Both the provincial capital (and island capital) dummy variable and the dummy for large municipalities (over 100,000 inhabitants), which are included in some tests, are highly significant. Our model finds that the lack of access to palliative services at home is not significant in the model.
This unexpected result may be due to the high number of municipalities without such access in a specific region (Canary Islands), which is also included as a dummy in the model. When this dummy is excluded from the model, the lack of access is very significant at 1%, with a coefficient of −0.045 (result not shown).
Some autonomous communities, particularly Madrid and the Canary Islands, have extremely low percentages of home deaths compared with deaths in hospitals. This finding should be interpreted with caution. While in the Canary Islands it could be due to lack of access to palliative services at home, in Madrid it could be a consequence of hospital-centeredness derived from a hospital supply that is substantially greater than in others autonomous communities. At the other extreme, Valencia has a higher prevalence of home death, which may be associated with cultural and supply factors: it is the second region in the ranking of palliative care staff endowment (2.9 doctors per 100,000 inhabitants vs. 1.7 for Spain as a whole).
In economically depressed areas of the United Kingdom, terminal cancer patients have a lower probability of dying at home than in other locations.20 However, our study found no evidence that the economic level of the municipality influences the probability of dying in one place or another. Although we analysed a comprehensive economic database of municipal information, including tax bases, social security affiliation data and detailed municipal budgets, the only clear conclusion to be drawn is that we cannot affirm the existence of such an association. As we used data from external sources and they showed no significant results, they are not shown in paper.
This study, which uses cross-information from various sources, such as the invaluable Directory of Palliative Care Resources, is the first to conduct an in-depth examination with population data on differences in the place of death in Spain, and it provides valuable information for cancer treatment plans and for palliative care.
However, it has limitations. The first is that small municipalities (fewer than 10,000 inhabitants) had to be excluded, for reasons of anonymity. Secondly, the fact of dying at home does not necessarily imply a good death, if the decedent failed to request palliative care services from the primary care physician or from specialised palliative care services. The lack of real measures of the quality of death is a limitation of the study. Another limitation is the fact that we are not able to know which resources have public or private ownership or which resources are accessible to publicly insured patients with no charge.
Taking into account the greater frequency of deaths in hospitals than in patients’ homes, and the ease of access to hospitals, at least in urban areas, it is to be assumed that a large proportion of home deaths are accompanied by the provision of palliative services. On the other hand, some patients and family members prefer death to take place in the hospital, because this environment offers the reassurance that unnecessary pain and suffering will be avoided.33 In the autonomous communities in Spain there are different levels of implementation of the advance directives, which report the preferred place of death. Unfortunately, individual data are not available in the registry of death certificates. An acute care hospital, in many cases, is not the most appropriate place in which to die. In addition, a significant number of patients die in the emergency department, where staff focus more on trying to prolong life than in the palliative approach (approximately 20% of in-hospital deaths occur in this situation).34,35
Developing specific plans for palliative care, with an active role being played by primary care teams, may help improve the situation. Therefore, health care policies should take account of the need to ensure access to palliative services in the home. On the other hand, there is an active debate on the complementary versus substitutive role of primary care and hospital care in the optimum palliative care provision. Professional specialization in palliative care lacks regulation. Specific training in the skills for palliative care must be a part of the core curriculum of all accredited training programs in different professions (physicians, nurses and others).
About two third of the Spanish population prefer dying at home, but the majority of deaths (52%) occur in hospital (around two thirds for cancer patients).
What does this study add to the literature?In Spain, there are large territorial variations in the place of death (home, hospital or long-term care centre due to cancer, but the existance of home palliative care is not a clear factor. Dying in hospital is an urban phenomenum, and having higher education increases the probability of home death while death at a long-term care centre is more frequent as one does down in the educational level. Dying of cancer in hospital is an urban phenomenon while home deaths are more frequent in rural municipalities.
David Epstein.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsB.G. López-Valcárcel, J. Pinilla and P. Barber conceptualised and designed the study. B.G. López-Valcárcel, J. Pinilla and P. Barber oversaw data collection and performed the statistical analysis. B.G. López-Valcárcel drafted the manuscript and all co-authors participated equally in the revision and final approval of the manuscript. B.G. López-Valcárcel is the guarantor for the study. All authors had full access to all the data in the study (including statistical analysis, tables and figures) and can take responsibility for the integrity of the data and the accuracy of the data its analysis.
FundingAuthors gratefully acknowledge the financial support received from the ECO2013-48217-C2-1-R project funded by the Spanish State Programme of R+D+I (http://invesfeps.ulpgc.es/en).
Conflicts of interestNone.












