




To analyse health differences among partnered individuals in Spain aged 65-81 considering their combined (education of both partners and age gap) and household (economic capacity of the household) characteristics.
MethodA cross-sectional study of the 2015 Spanish sample of the European Union Statistics on Income and Living Conditions survey (EU-SILC) on partnered individuals aged 65-81 years (N=1787). Using logistic regression models separately for women and men we obtained odds and predicted probabilities of having less than good health (95% confidence intervals) according to combined information from both partners on education and age, the household's economic capacity and partner's health status.
ResultsProbabilities of not having good health are significantly less among lower educated women whose partners are more highly educated (compared to both partners being lower educated) and among women whose partner is younger or has good health status. The latter also applies to men. Living in a household without economic difficulties also favours health (both sexes).
ConclusionsFor both sexes a partner's health status is the variable that shows the largest effect on elderly partnered Spanish people's health but women's health appears to be more sensitive to their partner's educational attainment and the household's economic situation.
Analizar las diferencias de salud entre la población española de 65 a 81 años de edad que vive en pareja, considerando características individuales, combinadas de ambos miembros y generales de la pareja.
MétodoEstudio transversal de la muestra española del año 2015 de la Encuesta Europea de Condiciones de Vida de personas mayores (edades 65-81 años) que conviven en pareja (N=1787). Mediante modelos de regresión logística independientes para mujeres y hombres se obtuvo la estimación de las probabilidades de no tener buena salud autopercibida (intervalos de confianza del 95%) según la combinación del nivel de estudios y la edad de ambos miembros de la pareja, así como la capacidad económica del hogar y el estado de salud del cónyuge.
ResultadosLas probabilidades de no tener buena salud son significativamente menores entre las mujeres con menor nivel de educación cuyas parejas son más educadas (en comparación con las que tienen menos educación) y entre las mujeres cuya pareja es más joven o tiene un buen estado de salud. Esto último también se aplica a los hombres. Vivir en un hogar sin dificultades económicas también favorece la salud en ambos sexos.
ConclusionesPara ambos sexos, el estado de salud de la pareja es la variable que muestra el mayor efecto sobre la salud de la población mayor española que vive en pareja, aunque la salud de las mujeres parece ser más sensible al nivel educativo de su pareja y a la situación económica general del hogar.
The protective health effect of living with a partner is well-known,1–3 but we know less about health differences among partnered individuals. Although the link between health and individual socio-economic information from each partner member has already been studied,4,5 such research tested the effect of the partner's socio-economic characteristics in addition to the ego's characteristics rather than combining the socio-economic characteristics of both partners. The latter is the aim of the present study.
The health advantage of people co-residing with a partner has been extensively explained by a set of benefits related to living with a partner: first, being subjected to social control, particularly from partners. Especially partnered men may be more often encouraged to abandon risky behaviours than single individuals.3 Second, the combination of both partners’ social nets creates a wider source of possible resources to reduce the impact of events that may negatively impact health, such as becoming unemployed or widowed.6 And third, the optimization of common resources through economies of scale and specialization of tasks within the household enhances the socioeconomic status of both partners.6 The latter two health benefits also have a socio-economic gradient.7
When measuring socioeconomic status of individuals, education is a frequently used indicator of adult socioeconomic status in studies on health differences because of its stability over time (unlike income or employment status) given that it is typically completed early in adulthood.8 Using education also avoids problems of reverse causation when linking it with health outcomes in older ages.9 It also has a well-established negative association with long-term risky health behaviours like smoking or drinking10 and facilitates the effective use of health services.11 According to the social causation hypothesis, an individual's educational level is also assumed to affect material and psychosocial factors that in turn have effects on health. In this study, we extent this assertion by purporting that partner's education has an additional effect on health.
Indeed, previous studies have found positive associations between partner's educational attainment and individual's health, including self-perceived health,5 risky behaviour12 as well as mortality.4 All studies stated that the inclusion of partner's education adds meaningful information to better understand health inequalities, even after controlling for own educational level. A common explanation was that couples usually pool their resources (material and non-material).
In line with the latter, previous studies on health inequalities have indicated household capacity to make ends meet to be an accurate indicator of poverty as it summarises the economic context of a household.13 This is of special interest to our study as relatively few elderly Spanish women participated in the labour market, meaning that their socioeconomic status is dependent on their partner's labour trajectory. Moreover, household income is known to be associated with individual mental and self-perceived health.14,15
There are also other partner's features that can modify individual health and mortality risks. The spousal age gap has been associated with survival probabilities, although differently by gender: having a younger spouse is beneficial for men but detrimental for women, whereas having an older spouse is detrimental for both.16 Positive effects include psychological improvements of having a younger partner as well as selection effects (healthier individuals have higher chances of attracting younger partners).16 Conversely, being the caregiver of one's partner is a known risk factor for physical and mental health,17 a task that women fulfill more often than men due to their higher life expectancy and the traditional gender role norms roles.18 Partner's health status is another characteristic of the partner affecting individual health. Reasons that have been linked to this include shared living conditions,19 similar health-related behaviour20 and the already mentioned health risks when caring for an ill partner.21
Why study Spain? While studies on the relationship between joint (partner and own) education profiles and health status have focused on the United States or northern, western and central European countries, no country from southern Europe has yet been analysed. Moreover, Spain is an especially interesting case study because during the last half-a-century it experienced a process of rapid political and social change, transitioning from an ultra-conservative dictatorship (1939-1975) to a democracy-based market economy. The educational expansion and the massive insertion of women into the labour market started later in Spain than in other Western European countries.22 Accordingly, the productive and reproductive roles are still very much gendered for the older cohorts studied here, whereby the female socio-economic status is almost totally determined by their partners’ status.23
Within these socioeconomic, gender and cohort specificities of Spain, the study's aim is to determine whether, besides own educational attainment also characteristics of the partner (educational attainment and health status) and union (household capacity to make ends meet and the spousal age gap) affect individual health status among co-residing individuals aged 65 years and older. We contextualize our results within the high level of gender inequality typical of older Spanish cohorts. Our research questions are: 1) do partner and couple features complement what we currently know about health status variability of the Spanish older population? and 2) how does this vary by sex?
MethodData come from the Spanish cross-sectional sample of the European Union Statistics on Income and Living Conditions (EU-SILC) survey (2015 wave). Our target population are partnered Spaniards where both members of the couple are aged 65-81 (N=6569). The lower age boundary was fixed at 65 because this was the legal age at retirement at the time of the interview; 81 is the age of the oldest respondents. EU-SILC has information on socioeconomic status and health from all members living in a private household, although 32 couples which accomplished the age criteria were discarded because of incomplete data. Only native Spaniards who live with a partner were analysed (56% of the age-specific sample), irrespective of their marital status (due to the low (<1%) prevalence of marital statuses other than married). Given our interest in possible sex differences in the effect of partner characteristics on individual health, same sex couples were also removed from the analysis. This left us with 1787 couples with complete information on all variables.
Our dependent variable is individual self-reported health status, measured by the survey question ‘How is your health in general?’. The possible answers were dichotomised into good health (“good” and “very good” health) and less than good health (“fair”, “bad” and “very bad” health).
The co-variables are:
- •
Educational attainment of both partners: low or no education (ISCED 0); medium education (ISCED 1-2); and high education (ISCED 3-6). Information from both partners were then combined into seven categories: both partners low education; ego low education-partner medium or high education; ego medium education-partner low education; both partners medium education; ego medium education-partner high education; ego high education-partner low or medium education; and both partners high education (see Table I in online Appendix for further detail).
- •
Household ability to make ends meet: “easily or very easily”, “fairly easily”, “with some difficulty” and “with difficulty or great difficulty”.
- •
Age gap between partners: wife older than husband; no age gap (0 to 2-years older husband); husband moderately older (3-5 years); and husband much older (6+years).
- •
Partners’ health status: this information is obtained from the interviewee's partner's answer to the same question as the dependent variable and contains the same two categories.
The possible effects of the variables of interest on individuals’ health status were assessed by separate logistic regression models for men and women to assess possible gender differences. We present predicted probabilities of poor health with 95% confidence intervals that include all variables. Predicted probabilities allow the direct comparison of results from different models24 (odds ratios are reported in Table II in online Appendix). We additionally conducted a dominance analysis to determine the relative contribution from each variable in the total explained variance.25 Besides education and household ability to make ends meet, we also tested the effect of overall household income and the individual relative contribution to the overall household income. However, they were excluded from the final model because they did not produce a significant contribution (see Table III in online Appendix). To check the robustness of our results, we replicated our models for two other health outcomes available in EU-SILC (suffer from any chronic [long-standing] illness or condition; limitation in activities because of health problems). Both outcomes were operationalized as a dichotomous variable (1=yes; 0=no) and results are provided in Tables IV and V in online Appendix, and are briefly commented on in the discussion.
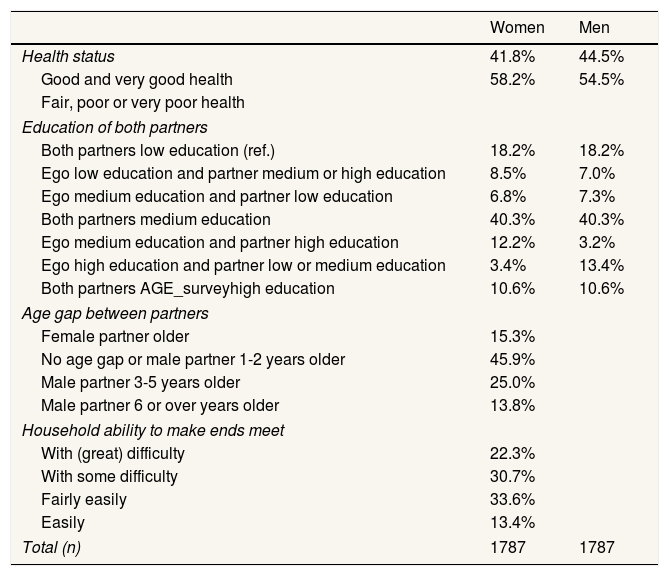
ResultsDescriptive analysisTable 1 displays the characteristics of our working sample. As common information is analysed for both partners, the sex-specific values are either the same for both sexes (e.g., household ability to make ends meet) or in reverse order (e.g., the combined educational level of each partner and the age gap between partners). Regarding health status, the values for the other sex in the table correspond to the results for the variable “health status of partner”.
Sample characteristics of partnered individuals aged 65-81 years by sex. Spain, 2015.
| Women | Men | |
|---|---|---|
| Health status | 41.8% | 44.5% |
| Good and very good health | 58.2% | 54.5% |
| Fair, poor or very poor health | ||
| Education of both partners | ||
| Both partners low education (ref.) | 18.2% | 18.2% |
| Ego low education and partner medium or high education | 8.5% | 7.0% |
| Ego medium education and partner low education | 6.8% | 7.3% |
| Both partners medium education | 40.3% | 40.3% |
| Ego medium education and partner high education | 12.2% | 3.2% |
| Ego high education and partner low or medium education | 3.4% | 13.4% |
| Both partners AGE_surveyhigh education | 10.6% | 10.6% |
| Age gap between partners | ||
| Female partner older | 15.3% | |
| No age gap or male partner 1-2 years older | 45.9% | |
| Male partner 3-5 years older | 25.0% | |
| Male partner 6 or over years older | 13.8% | |
| Household ability to make ends meet | ||
| With (great) difficulty | 22.3% | |
| With some difficulty | 30.7% | |
| Fairly easily | 33.6% | |
| Easily | 13.4% | |
| Total (n) | 1787 | 1787 |
Note: Data weighted by the survey's personal cross-sectional weight.
Source: Spanish sample EU-SILC 2015.
As expected, women report worse health than men (58% of women reported to have less than good health vs. 55% of men), even though they were on average 2.1 years younger. 39% of women had at least a three-year older partner, while 15% were older themselves. Regarding educational attainment, homogamy was high among the studied cohort (70%). The most frequent situation was both partners with medium education (40%), followed by both with low education (18%) and couples where the male partner is high educated and the female partner medium educated (12%). The least frequent situation was the opposite (3%). With regard to the household's ability to make ends meet, 53% declared to have financial difficulties.
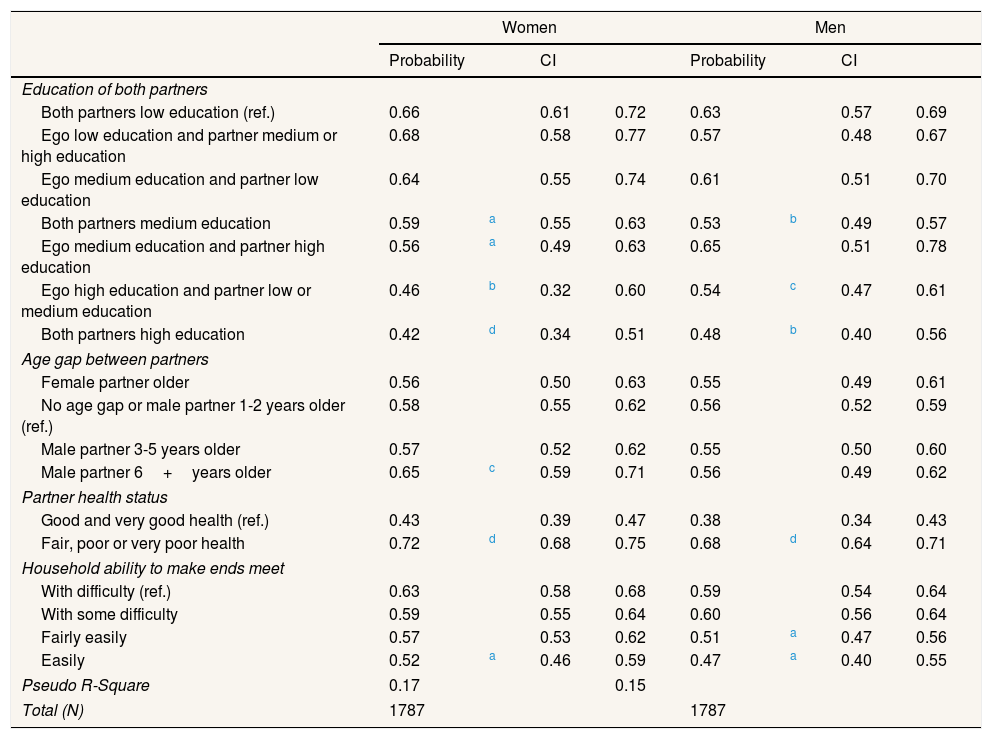
Multivariate analysisTable 2 displays the predicted probabilities of having less than good health. Only the results for the final model which includes all variables of interest and controls for age are shown here. In general, the female model that includes common features of the couple explains variability in self-perceived health in Spain better than the male model (r2=0.18 vs. 0.15). This is therefore consistent with two earlier studies by the authors that considered the middle-aged adult population.26,27 In addition, the obtained predicted probabilities are generally higher for women than for men for all variable categories, although not statistically significant (p>0.05).
Predicted probabilities of having less than good health from the logistic regression models for partnered individuals aged 65-81 by sex. Spain, 2015.
| Women | Men | |||||||
|---|---|---|---|---|---|---|---|---|
| Probability | CI | Probability | CI | |||||
| Education of both partners | ||||||||
| Both partners low education (ref.) | 0.66 | 0.61 | 0.72 | 0.63 | 0.57 | 0.69 | ||
| Ego low education and partner medium or high education | 0.68 | 0.58 | 0.77 | 0.57 | 0.48 | 0.67 | ||
| Ego medium education and partner low education | 0.64 | 0.55 | 0.74 | 0.61 | 0.51 | 0.70 | ||
| Both partners medium education | 0.59 | a | 0.55 | 0.63 | 0.53 | b | 0.49 | 0.57 |
| Ego medium education and partner high education | 0.56 | a | 0.49 | 0.63 | 0.65 | 0.51 | 0.78 | |
| Ego high education and partner low or medium education | 0.46 | b | 0.32 | 0.60 | 0.54 | c | 0.47 | 0.61 |
| Both partners high education | 0.42 | d | 0.34 | 0.51 | 0.48 | b | 0.40 | 0.56 |
| Age gap between partners | ||||||||
| Female partner older | 0.56 | 0.50 | 0.63 | 0.55 | 0.49 | 0.61 | ||
| No age gap or male partner 1-2 years older (ref.) | 0.58 | 0.55 | 0.62 | 0.56 | 0.52 | 0.59 | ||
| Male partner 3-5 years older | 0.57 | 0.52 | 0.62 | 0.55 | 0.50 | 0.60 | ||
| Male partner 6+years older | 0.65 | c | 0.59 | 0.71 | 0.56 | 0.49 | 0.62 | |
| Partner health status | ||||||||
| Good and very good health (ref.) | 0.43 | 0.39 | 0.47 | 0.38 | 0.34 | 0.43 | ||
| Fair, poor or very poor health | 0.72 | d | 0.68 | 0.75 | 0.68 | d | 0.64 | 0.71 |
| Household ability to make ends meet | ||||||||
| With difficulty (ref.) | 0.63 | 0.58 | 0.68 | 0.59 | 0.54 | 0.64 | ||
| With some difficulty | 0.59 | 0.55 | 0.64 | 0.60 | 0.56 | 0.64 | ||
| Fairly easily | 0.57 | 0.53 | 0.62 | 0.51 | a | 0.47 | 0.56 | |
| Easily | 0.52 | a | 0.46 | 0.59 | 0.47 | a | 0.40 | 0.55 |
| Pseudo R-Square | 0.17 | 0.15 | ||||||
| Total (N) | 1787 | 1787 | ||||||
CI: confidence interval.
Regarding the observed difference in each sex-specific model, the variable that combines the educational attainment of both partners showed significantly higher predicted probabilities of having less than good health among low-educated women with low-educated partners (the reference category) compared to medium-educated women with equal or higher educated partners as well as higher-educated women irrespective of their partner's educational level. Regarding men, coresiding with a higher-educated partner did not influence their health. Only having the same educational level as their partner (medium or high) was associated with better health than the reference category.
Turning to the age gap between both partners, the only observed difference (albeit at the 0.1 level) was for women whose partner was at least 6 years older. They had a higher probability of having less than good health than the reference category (no age gap).
Partner's health status is the variable that showed the largest effect on one's health: the proportion of women with less than good health equals 0.72 when the partner has the same health status, but just 0.43 if his health is good. Similar results are observed for men (respectively, 0.68 and 0.38).
The last tested variable, household capacity to make ends meet, was also significant for both sexes, although the only difference with the reference category (with (great) difficulty) was for those who have it easy to make ends meet.
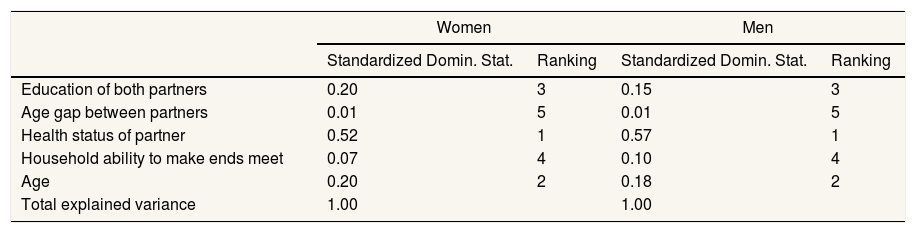
In terms of the relative explanatory capacity of the independent variables (Table 3), results are very similar for both sexes. Partner's health status explains the most, contributing to the 47% of the explanatory capacity of the female and 52% of the male model, followed by ego's age (18% for both sexes) and education of both partners (14% for women and 11% for men). Economic capacity of the household and former occupation of the ego and partner explain between 4% and 8% of the variance in both models. The couple's age gap has the least explanatory power (1% in each case).
Dominance analysis of the logistic regression models of having less than good health from the sex-specific logistic regression models for partnered individuals aged 65-81. Spain, 2015.
| Women | Men | |||
|---|---|---|---|---|
| Standardized Domin. Stat. | Ranking | Standardized Domin. Stat. | Ranking | |
| Education of both partners | 0.20 | 3 | 0.15 | 3 |
| Age gap between partners | 0.01 | 5 | 0.01 | 5 |
| Health status of partner | 0.52 | 1 | 0.57 | 1 |
| Household ability to make ends meet | 0.07 | 4 | 0.10 | 4 |
| Age | 0.20 | 2 | 0.18 | 2 |
| Total explained variance | 1.00 | 1.00 | ||
Data weighted by the survey's personal cross-sectional weight.
Source: Spanish sample EU-SILC 2015.
Our study contributes to the growing body of research on health among partnered individuals. Moreover, we did this by also including characteristics from both partners combined rather than that from each partner separately. Results showed for Spanish elderly aged 65-81 that women's health is more sensitive to the characteristics of the partner and household as more of the variability in female health status was explained by the tested variables. Co-residing with a partner not in good health is associated with almost double the probability of not having good health. One possible reason for this association is selective mating as two individuals with similar behaviour are more likely to match up, irrespective of socioeconomic status.2 Partners also influence each other's lifestyle during their relationship (for instance, it is more difficult to quit smoking if one's partner also smokes) and partner resemblance in health increases with relationship duration.21 This implies that assortative mating at younger ages (when couples are established) may have a cumulative effect on health as a consequence of behavioural factors (smoking, diet, alcohol consumption, etc.).
There are also gender implications from having a partner in poor health. When the husband is in poor health, the wife's health is likely to deteriorate due to the increase in their domestic workload.28 This might explain why, according to our results, living with a much older husband penalised female health. Conversely, the additional workload is lower for husbands when their wives have poor health as this is usually shared with other, mainly female, relatives, particularly daughters or daughters-in-law.29
Women's health was slightly more sensitive to their own and partner's educational level than men. First, their health was significantly (p <0.01) better if their educational level was higher than their partner's, a result that was less significant (p <0.1) in the case of men. Second, in the context of the known educational gradient in health, there is some suggestion that risk factors leading to health deterioration among women are also mediated through the educational status of their partner. However, this is mainly observed among women with medium education (the probability of having less than good health declines as the educational level of the partner becomes higher). The lower level of association for men in this case is consistent with results for the Netherlands5 and accords with the gendered social roles that typifies this Spanish generation where few women contributed financially to household income30 and were therefore dependent on the socioeconomic status of their partner.
Repeating the analysis for the two other health indicators included in EU-SILC led to similar results, thus confirming the importance of combining the educational attainments from both partners to better explain health inequalities among partnered older Spaniards. The only exception was the male model for chronic conditions and limitations, as results were not statistically significant. This seems to support results from elsewhere that show an educational gradient in chronic conditions and limitations among older women but not among men where the effect of education is less strong or significant in fewer chronic conditions.31,32 It would certainly be interesting for future research to explore these sex differences further as well as consider different types of chronic diseases.
Our study has shown that within an apparently advantageous population group in terms of health status, namely married or cohabiting couples, there are significant socioeconomic differences as higher educated individuals and those without economic problems have better heath than their lower educated and poorer counterparts. Therefore, a relevant contribution for public policy is that not only typical vulnerable groups like single-person, single-parent or low-income households should be targeted, but also retired low-educated partnered individuals, even if their partner is higher educated. This is not only because their probability of not having good health does not improve if the latter is the case, already 44% of 65-81 year-olds do not live with a partner, among whom health is significantly worse.3 Better targeted health education and health promotion33 and ensuring adequate income in old age for low-educated individuals are thus pertinent in the quest to reduce social health inequalities. Also noteworthy is the effect of partner's health on own health. This result is particularly relevant for health professionals who are in daily contact with patients as health inequalities are larger at the household level than at the individual level.21 The Spanish Society for Family and Community Medicine already recommends through their regularly updated Programme of Preventive and Health Promotion Activities (PAPPS in its Spanish acronym) general practitioners to assess the motivation and availability of the patient and his or her partner or other family members to change health-damaging behaviour and establish a joint action plan.34 Our result therefore reinforces the importance of involving the patient's partner as this would ease implementing specific interventions to achieve moderate habit changes (and may also benefit from it).
One weakness of our study is the lack of long-term longitudinal information about individuals’ trajectories to study possible mechanisms of selection prior to partner co-residence. The data source (EU-SILC) also lacks information on health behaviour, including fruit, vegetable, smoking and alcohol consumption, and physical activity, that may provide additional clues as to why higher educated individuals have better health than their lower educated counterparts. Additionally, combining individual and partner categories reduced the number of cases in each combination of educational level, resulting in fewer significant associations, an issue that would be resolved with a larger sample size. We must also keep in mind possible long-term influences of the economic crisis in Spain (2008-2014) at the time of the study (2015), as this may have amplified the sex-differences we found in the influence of the partner's socio-economic profile on individual's health. Finally, we cannot disclose whether the results for Spain are transferable to other countries as only one country was analysed. A comparative study for this age cohort between European countries characterised by different levels of gender inequality is therefore another recommendation for future study.
Previous studies have found a complementary explanatory effect of the inclusion of partner's characteristics to better understand health inequalities among individuals who live with a partner, even after controlling for own characteristics.
What does this study add to the literature?We contribute to this existing body of research by testing the effect of combining information from both partners (educational level and age) rather than analysing individual and partner's characteristics separately. We recommend targeting besides vulnerable groups like single-person or -parent households in health policy also couples (and their families) from low socioeconomic status groups.
María del Mar García-Calvente.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsThe first author conceived and designed the study and analysed the data. The second author contributed to the literature review and the methodology used in the analysis. Both authors interpreted the results and drafted and revised the manuscript and approved the final version for publication.
FundingThis study belongs to the multi-country project “Care, Retirement & Wellbeing of Older People Across Different Welfare Regimes” (CREW), founded from the Spanish Ministry of Economy, Industry and Competitiveness (PCINN-2016-005). This manuscript is also part of the project INTERSOC-HEALTH (RTI2018-099875-J-I00; PI: JG) founded by the Spanish Ministry of Science, Innovation and Universities. This work was supported by the Spanish Ministry of Economy and Competitiveness under the “Ramón y Cajal” program (RYC-2013-14851) for Jeroen Spijker and the “Juan de la Cierva” program (FJCI-2015-25066) for Jordi Gumà. Financial support was also received from the Catalan Government under the CERCA Program.
Conflicts of interestNone.












