



To systematically review guidance documents for the estimation of the social cost of illegal drugs, and to define standards for this estimation.
MethodA systematic literature search was conducted between April and May 2015 and updated in November 2015. Pubmed, Scopus, and Google Scholar were searched. Studies were included only if they provided indications of analytical methods for calculating the social cost of illegal drugs consumption.
ResultsA total of 21 papers were selected for a final review. Four main areas of discussion were identified: a) alternative theories for the framework design; b) basic concepts definition; c) theoretical issues in the application of the framework and; d) definition of the cost matrix and its elements. The review exercise enabled the definition of two analytical approaches, which are proposed as references for estimation in the field.
Conclusionsalthough social cost is a well-established method in the literature, there is a lack of agreement on the most appropriate approaches in the area of estimation of the social cost of illegal drugs consumption. Moreover, the two analytical approaches proposed are aimed at promoting more research focused at sophisticating the methodology in the field.
Revisar sistemáticamente las guías para la estimación del coste social del consumo de drogas ilegales y definir estándares para su estimación.
MétodoLa búsqueda sistemática de la literatura se realizó entre abril y mayo de 2015, y se actualizó en noviembre de 2015. Se realizaron búsquedas en Pubmed, Scopus y Google Scholar. Los estudios se incluyeron solo si explicitaban los métodos analíticos para calcular el coste social del consumo de drogas ilegales.
ResultadosSe seleccionaron 21 trabajos para su revisión final. Se identificaron cuatro áreas principales de discusión: a) teorías alternativas para el diseño del marco; b) definición de conceptos básicos; c) aspectos teóricos en la aplicación del marco; y d) definición de la matriz de costes y sus elementos. El ejercicio de revisión permitió la definición de dos enfoques analíticos, que se proponen como referencia para estimación en este campo.
ConclusionesAunque el coste social es un método bien establecido en la literatura, existe falta de acuerdo sobre los enfoques más apropiados en su aplicación al consumo de drogas ilegales. Los dos enfoques analíticos propuestos tienen como objetivo promover una mayor investigación enfocada a mejorar la metodología en este campo.
Drug addiction directly accounted for 20 million disability adjusted life years (DALY) in 2010, accounting for 0.8% of global all-cause DALY.1 The proportion attributed to drug dependence is increased in countries with the highest income. Therefore, knowing the social costs that illegal drugs impose on society is key in policy planning and evaluation.
However, from its early beginning,2,3 the literature on estimates of social costs of illegal drugs has been characterized by an intense dispute regarding which can be considered the most appropriate method of analysis. The theoretical debate is based mainly on the controversy regarding the definition of some of the basic concepts, as “social cost” and the counterfactual and the complexity regarding the nature of the causal relationships between the consumption of illegal drugs and their negative effects on individuals and society.4–7
A rich breadth of literature has focused at both estimating the social costs and at systematizing these open issues and providing guidance to properly address them. In our context, interesting and promising exercises have been made to estimate the social cost of illegal drug use and discussing about the needed elements to build calculations.8,9
Recently, the LEADER project10 aimed at contributing to this exercise by conducting a state-of-the art analysis regarding the achievements and challenges for future research in the field of estimating the social cost of illegal drugs.11
In particular, the objective of this work in the context of the LEADER project is to review published guidelines for the estimation of the social costs of illegal drugs, identify the main controversies and the differences between the proposed approaches, discuss on the impact of adopting one or another and to provide a framework for future studies.
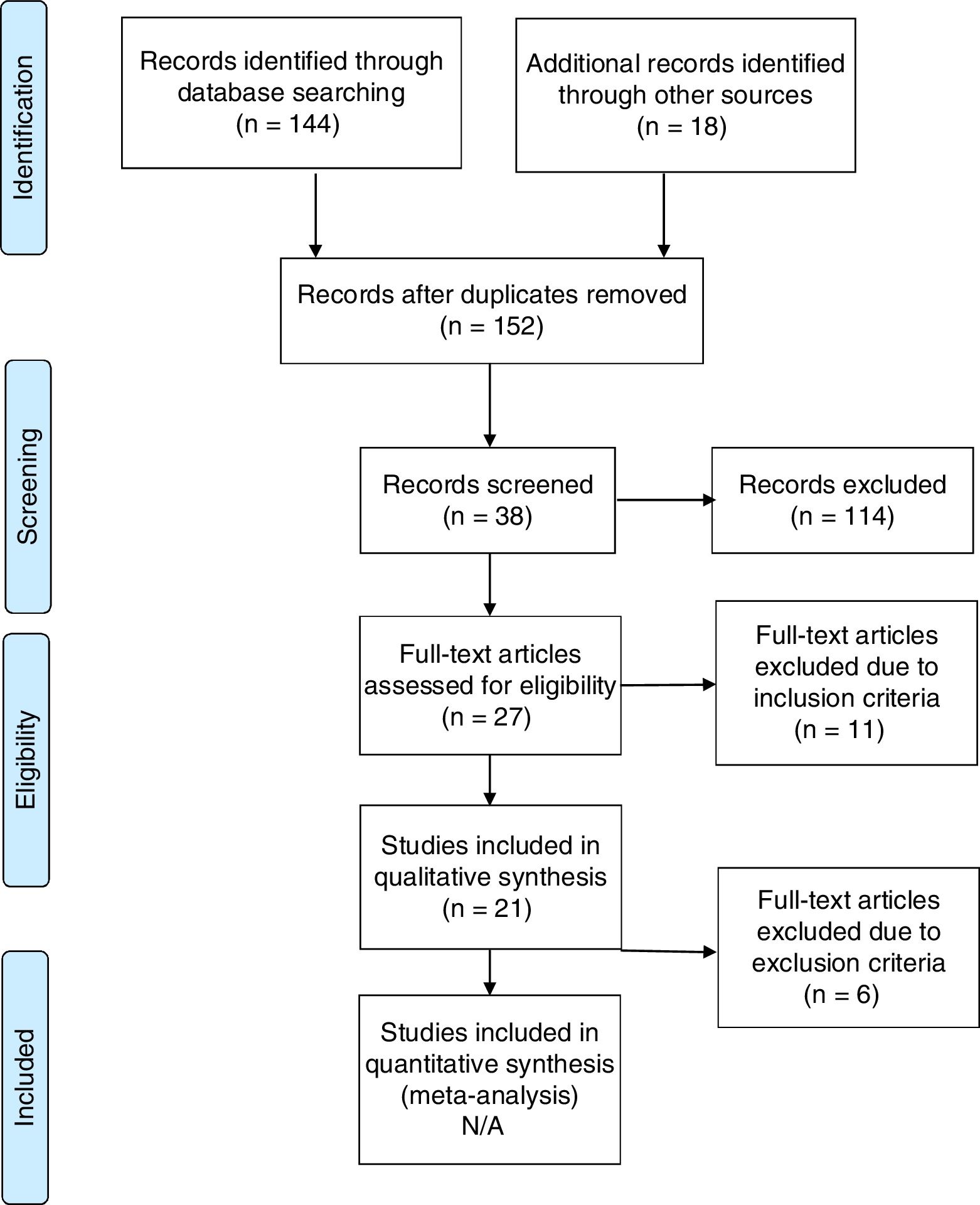
MethodsOnline databases (Scopus, PubMed and Google Scholar for the grey literature) were searched for published articles on guidelines for estimating the social cost of illegal drug consumption (see Annex 1 for the search strategy). The search generated 162 references. After the exclusion of 10 duplicates, a total of 152 papers were identified. Only those papers whose abstract seemed aligned with the review purpose were selected. After this review, 38 papers were selected and read in their entirety. At this stage, three inclusion criteria were used: 1) the study provides guidance regarding the estimation of social cost of illegal drugs and/or a related theoretical issue; 2) the study was published between 1990 and 2015; and 3) the study is written in English. After this review, 27 papers were discarded and 11 excluded. For the final review, two exclusion criteria were used: 1) the paper includes only primary data analysis, thus did not provide theoretical explanations on the method/s adopted; and 2) for each component of its framework, the paper did not compare available methodological alternative and doesn’t explicit the rationale for adopted approach. After this final stage, 21 papers were finally selected.
The final systematic review was conducted in line with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines12 (Fig. 1).
Results
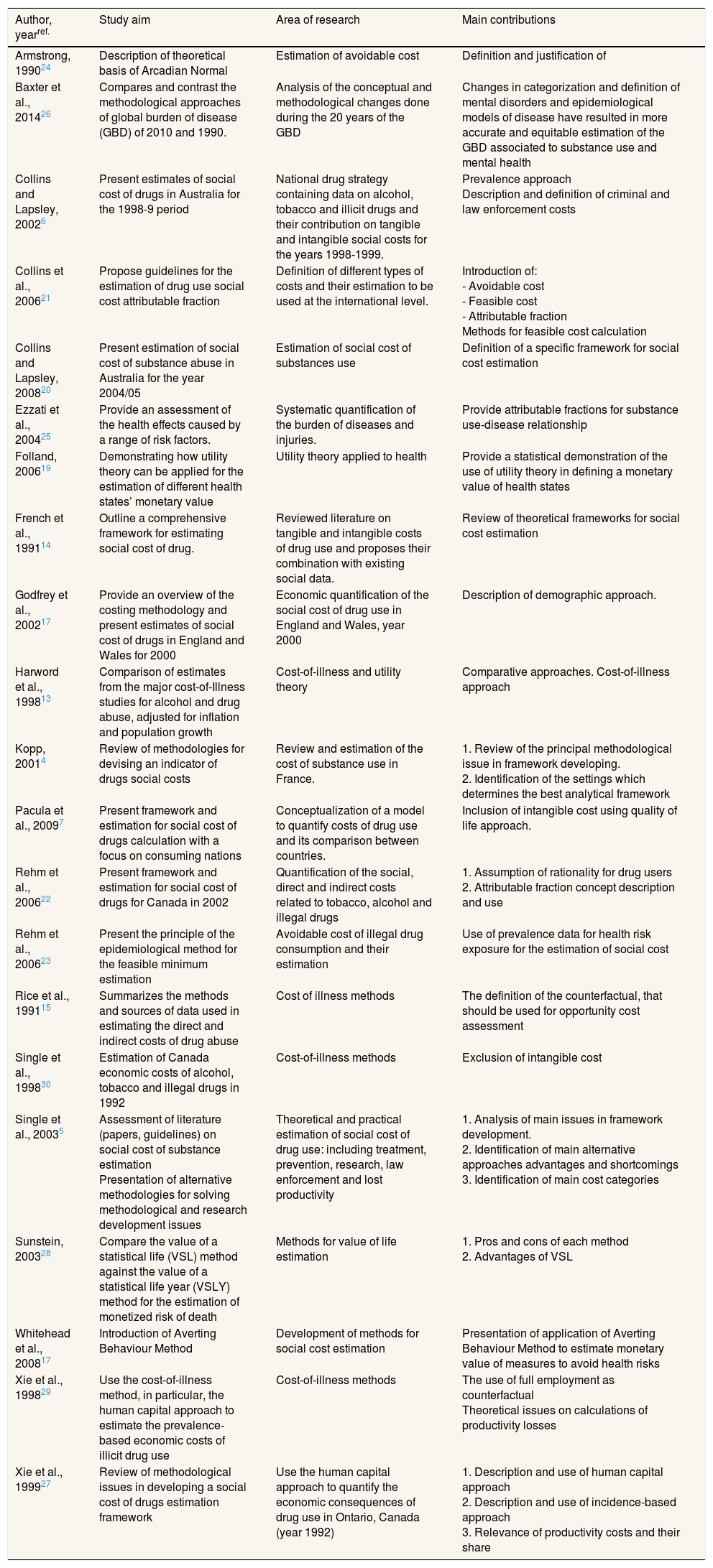
The 21 articles included are listed in Table 1, and their main contributions to the debate are listed. The results of the review are described below grouped in the four areas of debate that have been identified as crucial in field of the estimation of the social cost of illegal drugs.
Main contributions from the included articles.
| Author, yearref. | Study aim | Area of research | Main contributions |
|---|---|---|---|
| Armstrong, 199024 | Description of theoretical basis of Arcadian Normal | Estimation of avoidable cost | Definition and justification of |
| Baxter et al., 201426 | Compares and contrast the methodological approaches of global burden of disease (GBD) of 2010 and 1990. | Analysis of the conceptual and methodological changes done during the 20 years of the GBD | Changes in categorization and definition of mental disorders and epidemiological models of disease have resulted in more accurate and equitable estimation of the GBD associated to substance use and mental health |
| Collins and Lapsley, 20026 | Present estimates of social cost of drugs in Australia for the 1998-9 period | National drug strategy containing data on alcohol, tobacco and illicit drugs and their contribution on tangible and intangible social costs for the years 1998-1999. | Prevalence approach Description and definition of criminal and law enforcement costs |
| Collins et al., 200621 | Propose guidelines for the estimation of drug use social cost attributable fraction | Definition of different types of costs and their estimation to be used at the international level. | Introduction of: - Avoidable cost - Feasible cost - Attributable fraction Methods for feasible cost calculation |
| Collins and Lapsley, 200820 | Present estimation of social cost of substance abuse in Australia for the year 2004/05 | Estimation of social cost of substances use | Definition of a specific framework for social cost estimation |
| Ezzati et al., 200425 | Provide an assessment of the health effects caused by a range of risk factors. | Systematic quantification of the burden of diseases and injuries. | Provide attributable fractions for substance use-disease relationship |
| Folland, 200619 | Demonstrating how utility theory can be applied for the estimation of different health states’ monetary value | Utility theory applied to health | Provide a statistical demonstration of the use of utility theory in defining a monetary value of health states |
| French et al., 199114 | Outline a comprehensive framework for estimating social cost of drug. | Reviewed literature on tangible and intangible costs of drug use and proposes their combination with existing social data. | Review of theoretical frameworks for social cost estimation |
| Godfrey et al., 200217 | Provide an overview of the costing methodology and present estimates of social cost of drugs in England and Wales for 2000 | Economic quantification of the social cost of drug use in England and Wales, year 2000 | Description of demographic approach. |
| Harword et al., 199813 | Comparison of estimates from the major cost-of-Illness studies for alcohol and drug abuse, adjusted for inflation and population growth | Cost-of-illness and utility theory | Comparative approaches. Cost-of-illness approach |
| Kopp, 20014 | Review of methodologies for devising an indicator of drugs social costs | Review and estimation of the cost of substance use in France. | 1. Review of the principal methodological issue in framework developing. 2. Identification of the settings which determines the best analytical framework |
| Pacula et al., 20097 | Present framework and estimation for social cost of drugs calculation with a focus on consuming nations | Conceptualization of a model to quantify costs of drug use and its comparison between countries. | Inclusion of intangible cost using quality of life approach. |
| Rehm et al., 200622 | Present framework and estimation for social cost of drugs for Canada in 2002 | Quantification of the social, direct and indirect costs related to tobacco, alcohol and illegal drugs | 1. Assumption of rationality for drug users 2. Attributable fraction concept description and use |
| Rehm et al., 200623 | Present the principle of the epidemiological method for the feasible minimum estimation | Avoidable cost of illegal drug consumption and their estimation | Use of prevalence data for health risk exposure for the estimation of social cost |
| Rice et al., 199115 | Summarizes the methods and sources of data used in estimating the direct and indirect costs of drug abuse | Cost of illness methods | The definition of the counterfactual, that should be used for opportunity cost assessment |
| Single et al., 199830 | Estimation of Canada economic costs of alcohol, tobacco and illegal drugs in 1992 | Cost-of-illness methods | Exclusion of intangible cost |
| Single et al., 20035 | Assessment of literature (papers, guidelines) on social cost of substance estimation Presentation of alternative methodologies for solving methodological and research development issues | Theoretical and practical estimation of social cost of drug use: including treatment, prevention, research, law enforcement and lost productivity | 1. Analysis of main issues in framework development. 2. Identification of main alternative approaches advantages and shortcomings 3. Identification of main cost categories |
| Sunstein, 200328 | Compare the value of a statistical life (VSL) method against the value of a statistical life year (VSLY) method for the estimation of monetized risk of death | Methods for value of life estimation | 1. Pros and cons of each method 2. Advantages of VSL |
| Whitehead et al., 200817 | Introduction of Averting Behaviour Method | Development of methods for social cost estimation | Presentation of application of Averting Behaviour Method to estimate monetary value of measures to avoid health risks |
| Xie et al., 199829 | Use the cost-of-illness method, in particular, the human capital approach to estimate the prevalence-based economic costs of illicit drug use | Cost-of-illness methods | The use of full employment as counterfactual Theoretical issues on calculations of productivity losses |
| Xie et al., 199927 | Review of methodological issues in developing a social cost of drugs estimation framework | Use the human capital approach to quantify the economic consequences of drug use in Ontario, Canada (year 1992) | 1. Description and use of human capital approach 2. Description and use of incidence-based approach 3. Relevance of productivity costs and their share |
- 1)
Cost-of-illness
This approach was the first theoretical framework adopted for the estimation of substance abuse social cost.13 According to it, the estimation of the social cost of illegal drugs is calculated as the sum of the discounted value of resources used to diagnose and treat the illness and productivity losses due to related mortality and morbidity (productivity, use of resources, property destruction and losses, etc.).14 Cost-of-illness (COI) can be prevalence based, aiming at estimates the economic burden of a condition over a specific period, usually a year, or incidence based. In this last case, COI focus on the new cases of a conditions emerged during a specific year. For these, it estimates the lifetime costs from the illness onset until its disappearance. Incidence-based COI studies are designed to assess all future costs that are amenable to preventive policies. Prevalence-based studies, instead, picture the burden of a disease in a given time and represents a tool for defining the social and healthcare measures for tackling current substance abuse consequences and their related impact on public finance.6
One of the COI's main controversies is the definition of the counterfactual, i.e., the alternative scenario that should be used for opportunity cost assessment.15 The cases of a world with no drug or a switch towards either a lower level of consumption or other substances are equally plausible in theory.5 The use of “zero consumption” as a counterfactual is the most common choice. Another point of debate regarding COI is that uncertainty is not adequately accounted for,16 so different counterfactual scenarios have been defined for three types of illegal drug users: recreational users, older regular users, and problematic users.17 Additionally, sensitivity analysis has been adopted as a method for taking into account uncertainty.
- 2)
Averting behaviour method
Averting behaviour method aims at calculating expenditures individuals would make to protect them from and mitigate negative effects of risks.14 It assumes that a rational individual will use defensive behaviour as long as the value of the damage avoided exceeds the costs of the protective action.18 No examples are available in the literature, mainly because there is not a reliable calculation of averting behaviour cost.14
- 3)
Utility theory
Approaches based on utility theory aim at associating economic values with individuals’ preferences. In health economics studies, these approaches are used to estimate the value that individuals put on changes in mortality and morbidity probability,19 and they represent the base of the quality adjusted life years (QALY) measurement. Though utility theory is widely used, it has been criticized because it relies on probabilities of adverse health rather than real consequences generated by cases of adverse health effects.14
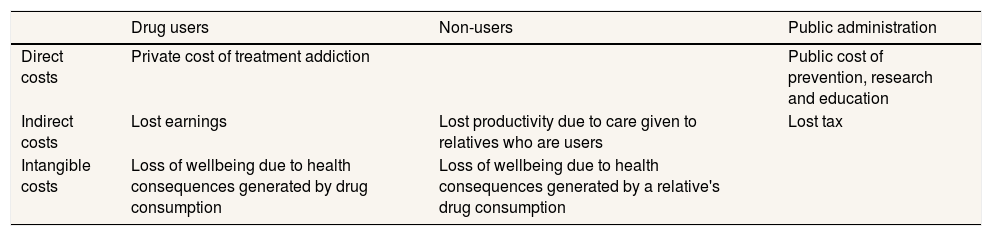
Basic concepts definitionOne of the most widespread categorisations of the social cost of drugs is represented by the dichotomy between tangible and intangible cost.20 When reduced, tangible costs yield new available resources; Intangible costs don’t. Intangible costs include items such as pain and suffering. Due to their nature, they are difficult to quantify and they are rarely included in the estimation. Within tangible cost, one can distinguish between direct and indirect costs.4 The first category includes costs which are clearly and directly associated with illegal drug consumption, as healthcare costs for treating addiction; the second is related to consequences that are not directly connected with consumption, as productivity losses (Table 2).
Categories of social cost of drugs: direct, indirect and intangible costs.
| Drug users | Non-users | Public administration | |
|---|---|---|---|
| Direct costs | Private cost of treatment addiction | Public cost of prevention, research and education | |
| Indirect costs | Lost earnings | Lost productivity due to care given to relatives who are users | Lost tax |
| Intangible costs | Loss of wellbeing due to health consequences generated by drug consumption | Loss of wellbeing due to health consequences generated by a relative's drug consumption |
Another criterion for social cost categorisation identifies three main categories.4,5 Private costs, as the costs borne only by an individual, in this case the illegal substance user (e.g., money spent for buying substances); public costs, i.e. expenditures incurred by central and local government in relation to psychotropic substances use, as is the case of healthcare and treatment costs in universalistic national health services; and external costs or externalities, referring to those public costs that are generated by the individual making the consumption decision but external to the same individual.
While the pertinence of the last two categories is acknowledged, inclusion of private cost has been highly debated. Its exclusion has been justified by the assumption of the rationality of drug users, and criticized given that drug users’ behaviour may be determined by the irrationality produced by addictions, thus violating the rationality postulate.5 Moreover, private decisions within the drug consumption and addiction context do have consequences and generate costs that are not limited to consumers themselves.5 This would justify the inclusion of part of the private cost in social cost, but it remains unclear which part of it and how it should be calculated.
Avoidable cost and methods for their estimationThe cost related to substance use can be divided in two groups. Unavoidable costs, generated from already existing drug-related diseases and new cases due to prior consumption, plus cases due to continued, irreducible consumption; And avoidable costs, those that are amenable to interventions and behaviour changes. This last category is the one that really provides information regarding the benefits that interventions which reduce drug use can generate.21
A method for identifying avoidable cost is attributable fraction.22 Together with attributable fractions, the estimation of the potential impact of policies around illegal drugs must take into account the lowest achievable level of substance use that policies should be expected to realistically aim for, which the literature terms the feasible minimum.19 Given its objective, feasible minimum can be of help in the execution of cost-benefit analysis, as it provides a method for better defining the cost and consequences that an addiction policy aims to contrast.
Authors identify four alternative methods for calculating it:
- 1)
Epidemiological method
This method has two alternative approaches23:
- •
The classical approach, which derives feasible minimum from each population's exposure to an illness-specific risk factor. This approach is retrospective, as it is based on population exposure in the past, and uses the hypothesis of no exposure. as the counterfactual.
- •
The distributional approach is a prospective analysis which entails the assessment of changes in the risk factor exposure distribution. To select realistic distribution changes, scholars have considered the experience of comparable countries or followed historical trends.23
- 2)
The Arcadian normal
It is based on the assumption that, for each population, “a level of disease that might be reasonably achieved if only we all know that which might be reasonably known about the causes of the disease in question” can be identified.24 Groups of countries with genetically similar populations and comparable living standards share the same Arcadian normal, defined as the within-group lowest age-standardised mortality rate for each cause of death. From this, potentially avoidable mortality and feasible minimum can be estimated.
The main shortcomings of this approach are21: it does not take into account each country's exposure-specific profile, it is not disease-specific, and it groups countries according to a non-comprehensive approach (only genetic profile and living standards), not considering differences regarding other relevant factors.
- 3)
Exposure-based comparators
For countries that do not have a long tradition of healthcare data collection, an alternative is the use of prevalence data as a proxy for attributable fraction.21 This method relies on World Health Organisation (WHO) estimations of relative risks, which are performed grouping countries by sub-region.25
- 4)
Using evidence on interventions’ effectiveness
Avoidable cost estimation can be supported by evidence generated by the literature on drug use interventions and policies, although with limitations.25
For future research on this topic, it would be of interest that new approaches were developed as a combination of the four above mentioned methods, for example using specific relative risk of the WHO sub-regions together with a gross domestic product (GDP)-based country selection.
Theoretical issues in the framework application- 1)
Incidence vs. prevalence perspective
The literature indicated a large consensus towards the prevalence based approach.4,26,27 As for the human capital and demographic approach dichotomy, the two methods should be considered as complementary rather than alternative.4,5
- 2)
Intangible costs
The most debated aspect related to the inclusion of intangible costs is their conversion to monetary value. Two methodologies has been proposed for their estimation5: the human capital approach, described in the previous section, and willingness to pay, which involves calculating intangible costs by identifying the amount of money that would be spent by an individual on reducing the risk of death associated with an illness, using this as an instrument for calculating the value of life.28
Studies that tried to estimate intangible costs have been published only recently.6,17,19 Others have preferred to not include intangible costs in their estimation.7,23 A less demanding and more flexible and much more widespread approach is to convert the various health impacts into a common health unit, and then apply a fixed monetary value to each unit. QALY have been proposed as such a measure7, but it does not exist such a general agreement on the appropriate monetary value of QALY (WHO 2009). More details on both the revealed valuation and the stated preference approaches, as well as on the value of QALY can be found on cost-benefit and cost-utility analysis literature.
- 3)
Productivity losses
They represent all those losses of production or productivity at work connected to the consumption of illegal drugs, due to premature death, disability, absenteeism or others.5 Two main methods have emerged in the review. The first one is the human capital approach, described in the previous section. While using this method, authors have adopted the case of full employment, thus no loss of productivity due to drug consumption, as counterfactual.29,30 An alternative is represented by the friction cost method, which is based on the time and related cost that is connected with the replacement of the workers whose absent due to illness by another coming from the pool of unemployed.22 While friction allows for a more exact calculation of real cost sustained by an employer in substituting a worker, it's application is limited, as it requires data on disease-specific employment rate and job vacancy duration.22
The matrix of costs and its elementsThe literature on the social costs of illegal drugs contains a wide variety of proposals regarding the categories and sub-categories that should be included in the matrix of costs. The most common types of costs included are5: healthcare and welfare costs, productivity costs, criminal justice costs, and other costs.
Healthcare costs can be divided into three main subcategories: cost for substance use treatment; cost for co-morbidity treatment; prevention, education and research programmes.29,30 For productivity losses, three sub-categories of cost can be identified: premature mortality, which can be generally retrieved from national databases; morbidity-lost work time or lower productivity, connected to events like days of work or work time lost due to harms, disabilities or negative impact on workers productivity generated by consumption of illegal drugs; and non-workforce productivity losses, related to production lost from unemployed people, retired people or individuals outside the workforce, who can still produce output through unpaid work. The approach is to assign a value to those activities from equivalent services purchased from outside sources.29,30
Criminal justice costs due to drug use refer to a broad and complex domain, although two sub-categories can be identified5: those that are directly related to the activities aimed at combating and preventing criminal activities connected to illegal drug use; And drug crime victims’ losses, which are mainly connected to the time lost, and related loss in work productivity, experienced by those who are victims of drug-related crime.
Other costs include the costs which are not strictly related to those previously described, such as property losses due to crime caused by substance use.
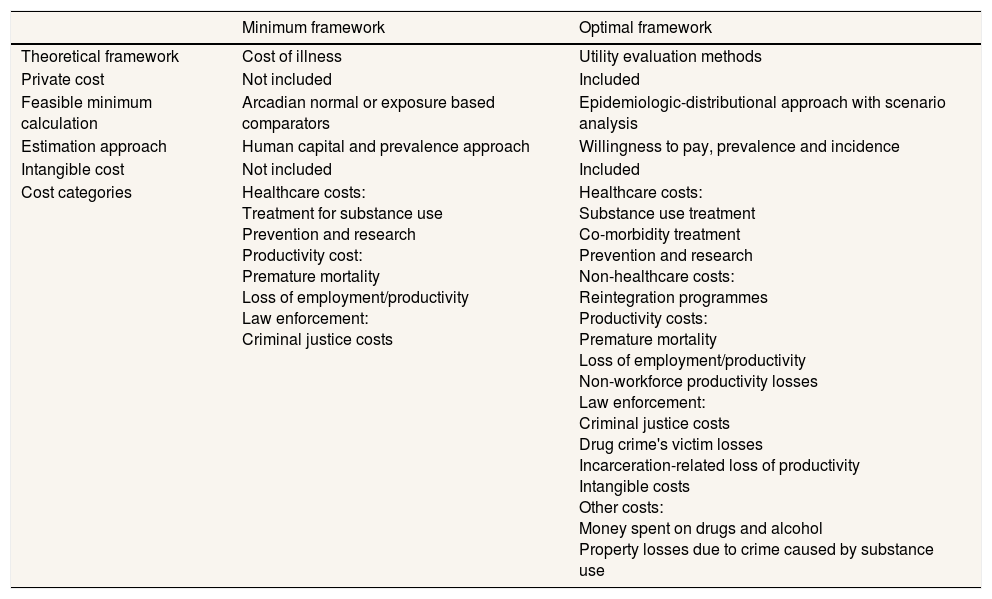
DiscussionThis overview has allowed the analysis of the advantages and shortcomings of this domain's most diffuse methods and highlights the absence of a comprehensive approach in this field. The current debate on methods for assessing drugs’ social cost would significantly benefit from the identification of new estimation frameworks that, taking into account the mentioned shortcomings, can represent standards for guaranteeing reliability and rigour of future illegal drugs’ social cost estimation. With this regard, two analytical frameworks for the estimation of the social cost of drugs for future research are provided (Table 3).
Proposed frameworks for the estimation of the social cost of drugs.
| Minimum framework | Optimal framework | |
|---|---|---|
| Theoretical framework | Cost of illness | Utility evaluation methods |
| Private cost | Not included | Included |
| Feasible minimum calculation | Arcadian normal or exposure based comparators | Epidemiologic-distributional approach with scenario analysis |
| Estimation approach | Human capital and prevalence approach | Willingness to pay, prevalence and incidence |
| Intangible cost | Not included | Included |
| Cost categories | Healthcare costs: Treatment for substance use Prevention and research Productivity cost: Premature mortality Loss of employment/productivity Law enforcement: Criminal justice costs | Healthcare costs: Substance use treatment Co-morbidity treatment Prevention and research Non-healthcare costs: Reintegration programmes Productivity costs: Premature mortality Loss of employment/productivity Non-workforce productivity losses Law enforcement: Criminal justice costs Drug crime's victim losses Incarceration-related loss of productivity Intangible costs Other costs: Money spent on drugs and alcohol Property losses due to crime caused by substance use |
The first proposed framework can be considered as minimum standard which researchers should refer to for calculating social cost of illegal drugs. It sets a level of estimation quality that all future research in the field should at least meet in order to be reliable. Its main components are the following:
- •
COI as the reference conceptual framework.
- •
Arcadian normal or exposure-based comparator methods for feasible minimum.
- •
Human capital approach.
- •
Prevalence approach.
- •
Treatment for substance use and prevention and research costs (healthcare costs), premature mortality and loss of employment/productivity (productivity costs), and criminal justice costs (law enforcement costs).
This framework includes non-controversial costs, using data generally available in public datasets. Existing research that does not comply with this framework should be carefully revised.
The second proposed framework represents an ideal approach for estimating the social cost of illegal drugs, as its application would produce the most comprehensive estimations. The higher level of comprehensiveness comes at the price of a higher risk of error, as the framework requires additional assumptions with respect to the previous approach. For this reason, this second framework can also be considered as a guide for methodological and data collection improvements in the field.
The ideal framework components are the following:
- •
Utility valuation methods as the conceptual framework, which would allow the most reliable calculation of direct costs, intangible costs and relevant private costs.
- •
Epidemiological-distributional approach, which allows the most reliable calculation of feasible minimum.
- •
“Willingness to pay” approach for the calculation of intangible costs and other cost categories for which there is lack of available data.
- •
Both prevalence and incidence-based approaches. If taken as complementary, they would offer a comprehensive time horizon perspective, including past, present and future costs.
- •
All the cost categories presented above.
A relevant topic for all studies of social cost estimation is data presentation and comparison with standard measures of economic activity. Different approaches have been suggested for tangible and intangible cost: while for the first gross domestic product should be use, for the latter that social costs of illegal drugs should be presented with respect to GDP.4
ConclusionsThe literature on the social cost of illegal drugs is characterized by a lack of agreement regarding the most appropriate methods for addressing the estimation.5,7,21 The review confirms the spectrum of methodological opportunities available.30 Researchers must take into account the benefits and shortcomings of each component and decide on a framework according to the research purposes and data availability.
The LEADER project aims at contributing to developments in illegal drugs social cost estimation methodologies.10 More than merely filling a theoretical gap, the project is aimed at strengthening current practices in the field in order to support the role of social cost as a tool for policy-makers. In fact, a practical problem that is directly related to the absence of an established methodology is the variability of estimations regarding the social cost of drugs and the impossibility of defining a reliable estimation, neither at the single drug, class of drug or at a country level. This has implications regarding the definition and prioritization of the interventions aimed at reducing the impact of illegal drugs. Until an illegal drug consumption cost exercise uses a reliable theoretical framework in order to identify and place value on all relevant costs, the possibility of comparing interventions in this field will be limited. The objective of this paper is to shed some light on this field, and to propose frameworks that could be helpful and informative tools for policy-makers.
Editor in chiefMiguel Ángel Negrín Hernández.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsVincenzo Alberto Vella was the person who conceived the work, carried out the review and critically reviewed the writing of the article. Anna García-Altés assisted in the review and has critically reviewed the writing of the article. Lidia Segura and Nuria Ibáñez interpreted the results and helped with the writing. Joan Colom has led the project and the conception of the article.
FundingNone.
Conflicts of interestNone.
Pubmed
((((econom*[ti] OR cost[ti] OR costs*[ti]) AND (drug*[ti] OR substance*[ti]) AND (illegal[ti] OR illicit[ti] OR abus*[ti] OR misuse[ti]) AND (guideline*[ti] OR method*[ti] OR theor*[ti]))) OR (Substance-Related Disorders/economics[majr] AND (guideline*[ti] OR concept*[ti] OR method*[ti] OR theoret*[ti] OR estimat*[ti]))) OR (Substance-Related Disorders[majr] AND (framework*[ti] OR guideline*[ti] OR concept*[ti] OR method*[ti] OR theoret*[ti] OR estimat*[ti]) AND (cost[ti] OR costs[ti] OR econom*[ti]))+
Scopus
(((TITLE (“social cost” OR “social costs”) OR TITLE (cost* OR econom* OR expenditur* OR calculat* OR burden))) AND ((TITLE((illegal OR illicit OR abus* OR depend* OR disord* OR addict*) W/1 drug*)) OR (TITLE ((illegal OR illicit OR abus* OR depend* OR disord* OR addict*) W/1 substan*)) OR (TITLE (cocaine* OR heroine* OR morphine* OR opioid* OR “street drugs”)))) AND (TITLE (guideline* OR guidance OR method* OR frame OR framing OR theor* OR concep*))
Google scholar
“social cost” AND (guidance OR guidelines) AND “illegal drugs”











