




To study the association between mobility restriction and mental health outcomes among Ecuadorian young adults.
MethodThe present is a cross-sectional study that included a non-probabilistic sample of mostly highly educated young adults. Socio-demographic and mental health data were collected through an online survey, between May and June 2020, when confinement was mandatory in Ecuador. Data on mobility was extracted from Google Community Mobility Reports. Four aspects of the participants’ mental health were evaluated: eating behavior (emotional eating), depression, sleep quality and sense of coherence as a proxy of resilience, using previously validated instruments. Data were analyzed using multiple linear regression models in R.
ResultsSample included 8426 young adults, with a mean age of 22.85 (standard deviation: 4.43), most of whom were women (n=5943, 70.53%). During mandatory confinement, in Ecuador mobility in general was reduced by nearly 50% in comparison to January/February, 2020. Less healthy eating behavior, depression, worse sleep quality and lower sense of coherence were associated with higher mobility restriction to workplaces and groceries/pharmacies. Women and youngsters more often showed depression, less healthy eating behavior, worse quality of sleep and lower sense of coherence in comparison with men and older respondents.
ConclusionsMobility restrictions during COVID-19 pandemic were associated with worse self-reported mental health in a sample of young highly-educated Ecuadorian adults. Women and youngsters were the most affected. Our findings highlight the need of implementing health promotion measures directed to ameliorate the effects of confinement on mental health, focusing on women and youngsters.
Estudiar la asociación entre la restricción de movilidad y la salud mental en personas adultas jóvenes de Ecuador.
MétodoEstudio transversal que incluyó una muestra no probabilística de personas adultas jóvenes con alto nivel de educación. Los datos sociodemográficos y de salud mental se recolectaron entre mayo y junio de 2020, cuando el confinamiento fue obligatorio, usando una encuesta en línea. Los datos sobre movilidad se extrajeron de Google Community Mobility Reports. Se evaluaron cuatro aspectos de la salud mental: alimentación emocional, depresión, calidad de sueño y sentido de coherencia como proxy de resiliencia, usando instrumentos previamente validados. Los datos se analizaron con modelos de regresión lineal múltiple usando R.
ResultadosLa muestra incluyó 8426 jóvenes, con una edad media de 22,85 años (desviación estándar: 4.43), mujeres en su mayoría (n=5943, 70.53%). Durante el confinamiento obligatorio, la movilidad se redujo aproximadamente un 50%. Comportamientos alimentarios menos saludables, depresión, peor calidad del sueño y menor sentido de coherencia se asociaron con mayor restricción de movilidad a lugares de trabajo y pequeños comercios o farmacias. Mujeres y jóvenes mostraron con mayor frecuencia depresión, conductas alimentarias menos saludables, peor calidad del sueño y menor sentido de coherencia.
ConclusionesLas restricciones de movilidad durante la pandemia de COVID-19 se asociaron con una peor salud mental en personas adultas jóvenes con alto nivel de educación. Mujeres y jóvenes fueron los más afectados. Es necesario implementar medidas de promoción de la salud dirigidas a paliar los efectos del confinamiento en la salud mental, especialmente en mujeres y jóvenes.
In March 2020 COVID-19 caused by the SARS-CoV-2 virus was declared global pandemic. Since then, COVID-19 has generated multiple public health concerns around the world, particularly due to the easiness of the virus transmission and disease morbidity and mortality.1 Given the emergency situation, government authorities have imposed closure measures and restrictions in order to reduce mobility and therefore physical contact in order to reduce the rate of infection. Although lock-down measures have helped to prevent the spread of the virus and control the pandemic, they have also negatively impacted mental health of people.2,3
COVID-19 pandemic has been associated with considerable psychological distress in terms of anxiety, depression, post-traumatic stress disorder, among others, which on the other hand are known triggers of unhealthy eating behaviors and poor sleep quality.4–6 Moreover, it has been observed that the frequency of unhealthy eating behaviors and altered sleeping patterns have increased during COVID-19 pandemic.5,7,8 Such deleterious consequences on mental health could be countered by resilience, which refers to the ability to overcome adverse situations, as those we have been experiencing from the start of the pandemic.9,10 A relevant construct within the notion of resilience is sense of coherence, which can be measure by the sense of coherence scale and seeks to assess an individual's ability to perceive life experiences in a way that allows constructively face adversity.9,10
Previous literature suggest that some population groups are more vulnerable to suffer mental health issues than others.6,11,12 In fact, in comparison to men, women show higher rates of stress-related psychiatric disorders, such as depression and anxiety, which has also been true during the pandemic.11,12 Higher vulnerability of women is probably related to their predominant role as family caregivers and their greater susceptibility to social isolation, which can trigger stress and exhaustion. Furthermore, there is evidence of sex differences in stress response, which can determinate the onset of mental disorders.13 From a public health policy perspective, identification of groups with lower capability of adaptation might help prioritizing attention to vulnerable groups and therefore, facing the pandemic more efficiently.
The present study aimed to study the association between mobility restriction and mental health outcomes of Ecuadorian young male and female adults. Four aspects of mental health were analyzed including, emotional eating, sleep quality, depression, and sense of coherence.
MethodStudy design and settingAn observational cross-sectional study design was implemented. An open, on-line, self-administered survey was used to collect data on socio-demographics and mental health. Data on mobility was collected from Google Community Mobility Reports.14 Data collection took place between May and June 2020, at that time confinement in Ecuador was mandatory.15
SamplingOur targeted population were young adults that is, individuals between 18 and 35 years old, men and women. Invitations to participate in the study were published in platforms and social networks (i.e. Facebook, Instagram, Twitter and WhatsApp) of several Ecuadorian universities. In this way, the study population came from a non-probabilistic sampling and was mostly composed by university students and teachers. From the 9582 responses received, we exclude people younger than 18 or older than 35 years old, whose age was not recorded or whom selected “other” as their gender (n=1156). The final sample included 8426 young adults.
SurveyThe survey was reviewed by four experts and first applied to 30 adults as a pilot study. After corrections were implemented, it was then distributed through social networks using Google Forms. It was mandatory that participants filled out some of the questions and no incentive was offered for answering the survey. Participants could review their responses and change their answers through a back button. Duplicate entries were avoided by preventing users access twice.
Variables1) Emotional eatingEmotional eating was evaluated using a validated questionnaire.16 The emotional eating questionnaire included 10 questions with four possibly answers: never, sometimes, frequently and always, which were graded 0, 1, 2 or 3, respectively. Each participant could obtain a score between 0 and 30. The lower the score, the healthier the behavior. Subjects were classified in four groups according to their score: 0-5 non-emotional eater; 6-10 low emotional eater; 11-20 emotional eater; and 21-30 very emotional eater.
2) Sleep qualitySleep quality was evaluated using the Spanish version of the Pittsburgh Sleep Quality Index (PSQI).17 PSQI consists of 19 self-evaluated items, grouped into seven components, each one receiving a score from 0 to 3: Subjective sleep quality, sleep latency, sleep duration, sleep efficiency, presence of sleep disorders, hypnotic medication use, and daytime dysfunction. The total score is equal to the sum of the seven components with a maximum of 21 points. Higher scores suggest worse sleep quality. Sleep quality can be classified as “good” (<5 points) or “poor” (≥ 5).
3) DepressionSymptoms of depression were evaluated using the Patient Health Questionnaire 9 (PHQ9).18 While the first eight items ask about frequency of depression symptoms, item nine asks over thoughts of dead or auto-mutilation. Response options for each item are as follows: “not at all” (0 points), “several days” (1 point), “more than half the days” (2 points) or “nearly every day” (3 points). PHQ9 total score ranges from 0 to 27. Scores of 1–4 indicate minimal, 5–9 mild, 10–14 moderate, 15–19 moderately severe, and 20+severe symptoms of depression.
4) Sense of coherenceSense of coherence scale developed by Antonovsky was applied to measure general ability to cope with stressful life situations.19 In this study, a reduced format with 15 items was used. The instrument was previously validated in Ecuadorian population.9 Respondents were asked to mark their response to each item on a scale of five alternatives: never, almost never, sometimes, almost always, and always, which received scores from 0 to 5, respectively. The final score ranges on a scale from 0 to 75 points 9. The higher the score, the higher the sense of coherence.19
5) MobilityMobility during the confinement was measured using Google Community Mobility Reports, which are publicly available and can be accessed via https://www.google.com/covid19/mobility/.14 Google Community Mobility Reports show movement trends by regions across different categories of places including, retail and recreation, grocery and pharmacy, parks, transit stations, residential and workplaces.14 Reports are created with aggregated, anonymized sets of data from users.14
Data show how visits to places or time spent in places change compared to baseline days, which represent normal values of mobility for a typical day of the week. The baseline day is the median value form the five-week period between January 3 and February 6, 2020.14 Change of mobility with respect to the baseline day is calculated as the percentage difference between mobility at a specific day and its corresponding baseline day.14 We extracted data for mobility for day during 2020 and matched it to the date the participant answered the survey.
6) GenderGender was defined by the question “How do you identify yourself?”. This question had three possible answers: woman, men, other. As few persons answered “other” (n=26), we did not include this category in the analysis.
Statistical analysesWe implemented four linear multiple regression models, one for each of the mental health aspects that were evaluated. In this way, scores for emotional eating, sleep quality, depression and sense of coherence were included in the regression models as dependent variables. Our main predictors were percentage of mobility change, gender and age. From the six aspects of mobility initially considered, we included two in the models in order to avoid collinearity, since most of them were highly correlated (Supplementary Fig. I). These included mobility to workplaces and to groceries/pharmacies, which were of interest for our purpose.
All analyses were conducted using R version 3.6.3 (2020-02-29),20 RStudio version 1.3.1093,21 and the package rms to implement the regression models.22 Adjusted predicted means with 95% confidence intervals (95%CI) were calculated for each of the scores. Predicted means were adjusted by living with a partner, taking sleeping pills, area of residence (urban vs. rural), occupation (student, working or unemployed), and auto-report of times per week of leaving home. Age was included in the model as a linear predictor with restrictive cubic splines using the function “rcs”. Bootstrap estimates of the covariance matrix of coefficients were calculated using the function “bootcov” to obtain unconditional estimates. We applied 500 repetitions. Bootstrap estimates were corrected for intra-cluster correlation. A cluster was considered to be the province the respondents reported to be living in.
Ethics approval and related considerationsThe present study was carried out following the Declaration of Helsinki to work with human beings and in accordance with the Singapore Declaration on Integrity in Research. It was approved by the Scientific Committee of the School of Medicine and Instituto de Investigación (IDI) of the Escuela Superior Politécnica de Chimborazo. Participants who voluntarily accepted to participated, filled out an informed consent form, which was included at the beginning of the survey. We did not collect any personal information that allowed identification.
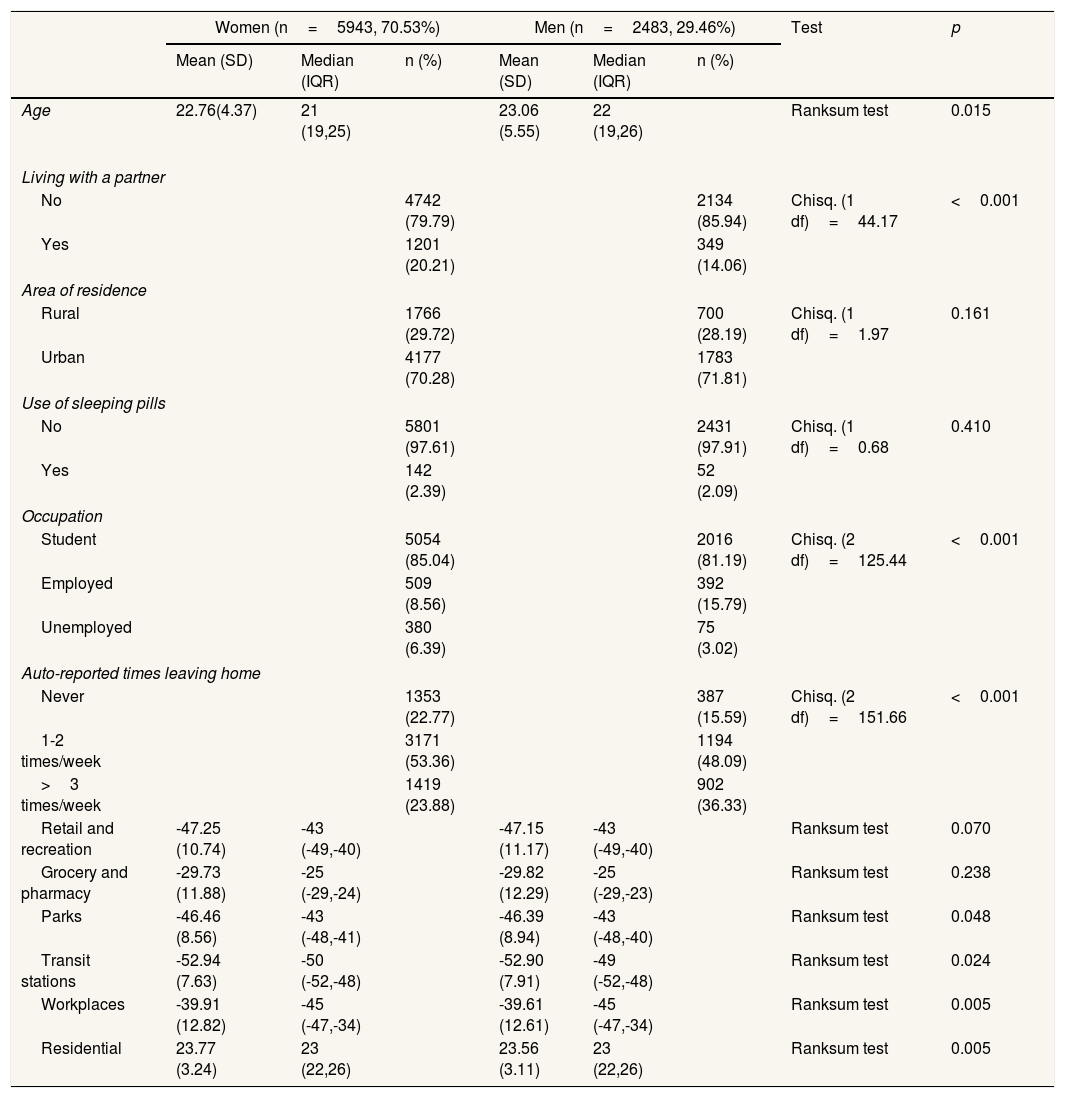
ResultsSample included 8426 individuals. Mean and median age of participants were 22.85 (standard deviation: 4.43) and 21 (interquartil range: 6), respectively. The majority of respondents were women (n=5943, 70.53%). Among women and men, the majority reported living without a partner, residing in urban areas, and not needing medication to sleep (Table 1). More than 80% of respondents among women and men were university students. Only few respondents among women and men reported never leaving home during mandatory confinement (Table 1). Women respondents were younger than men. In comparison to men, more women were students or unemployed and reported living with a partner. Women reported leaving home less often than men during the mandatory confinement (Table 1).
General characteristics of the sample. Sample included 8426 individuals, most of whom were women.
| Women (n=5943, 70.53%) | Men (n=2483, 29.46%) | Test | p | |||||
|---|---|---|---|---|---|---|---|---|
| Mean (SD) | Median (IQR) | n (%) | Mean (SD) | Median (IQR) | n (%) | |||
| Age | 22.76(4.37) | 21 (19,25) | 23.06 (5.55) | 22 (19,26) | Ranksum test | 0.015 | ||
| Living with a partner | ||||||||
| No | 4742 (79.79) | 2134 (85.94) | Chisq. (1 df)=44.17 | <0.001 | ||||
| Yes | 1201 (20.21) | 349 (14.06) | ||||||
| Area of residence | ||||||||
| Rural | 1766 (29.72) | 700 (28.19) | Chisq. (1 df)=1.97 | 0.161 | ||||
| Urban | 4177 (70.28) | 1783 (71.81) | ||||||
| Use of sleeping pills | ||||||||
| No | 5801 (97.61) | 2431 (97.91) | Chisq. (1 df)=0.68 | 0.410 | ||||
| Yes | 142 (2.39) | 52 (2.09) | ||||||
| Occupation | ||||||||
| Student | 5054 (85.04) | 2016 (81.19) | Chisq. (2 df)=125.44 | <0.001 | ||||
| Employed | 509 (8.56) | 392 (15.79) | ||||||
| Unemployed | 380 (6.39) | 75 (3.02) | ||||||
| Auto-reported times leaving home | ||||||||
| Never | 1353 (22.77) | 387 (15.59) | Chisq. (2 df)=151.66 | <0.001 | ||||
| 1-2 times/week | 3171 (53.36) | 1194 (48.09) | ||||||
| >3 times/week | 1419 (23.88) | 902 (36.33) | ||||||
| Retail and recreation | -47.25 (10.74) | -43 (-49,-40) | -47.15 (11.17) | -43 (-49,-40) | Ranksum test | 0.070 | ||
| Grocery and pharmacy | -29.73 (11.88) | -25 (-29,-24) | -29.82 (12.29) | -25 (-29,-23) | Ranksum test | 0.238 | ||
| Parks | -46.46 (8.56) | -43 (-48,-41) | -46.39 (8.94) | -43 (-48,-40) | Ranksum test | 0.048 | ||
| Transit stations | -52.94 (7.63) | -50 (-52,-48) | -52.90 (7.91) | -49 (-52,-48) | Ranksum test | 0.024 | ||
| Workplaces | -39.91 (12.82) | -45 (-47,-34) | -39.61 (12.61) | -45 (-47,-34) | Ranksum test | 0.005 | ||
| Residential | 23.77 (3.24) | 23 (22,26) | 23.56 (3.11) | 23 (22,26) | Ranksum test | 0.005 | ||
IQR: interquartil range; SD: standard deviation.
During the time the survey took place (May-June 2020), mobility due to retail and recreation was reduced by 47.22%, mobility to grocery and pharmacy was reduced by 29.75%, to parks by 46.44%, to transit stations by 52.93%, and to workplaces to 39.83%. In contrast, time spent in residential places increased by 23.71%. Mean and median change percentages for different aspects of mobility by sex are showed in Table 1.
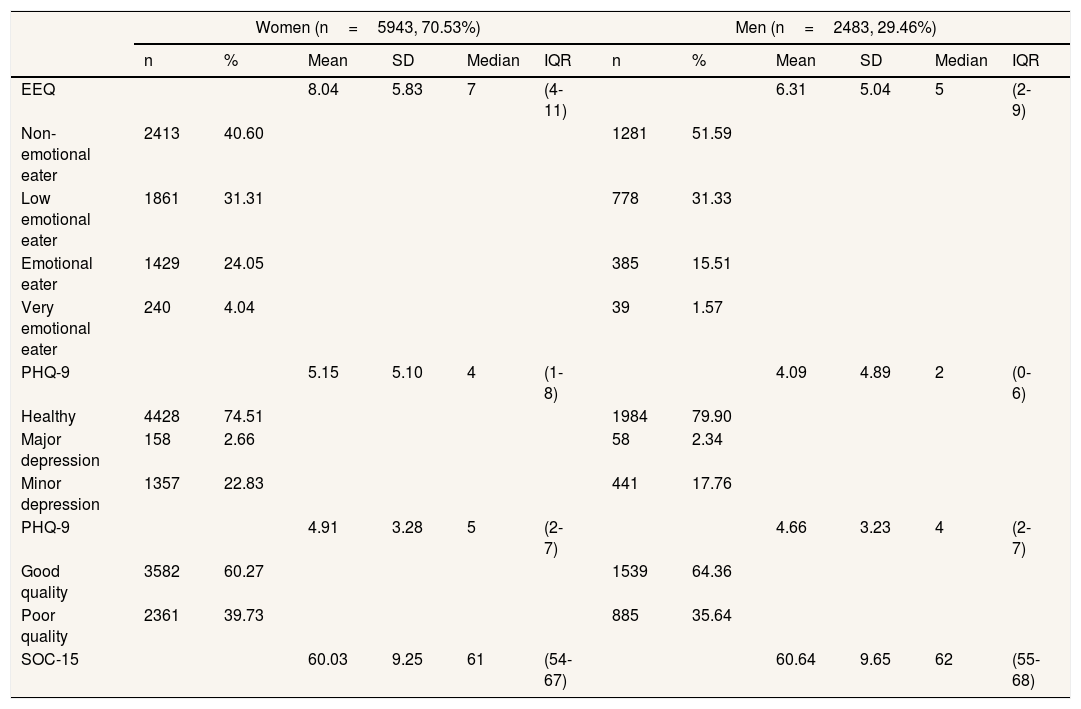
In comparison to men, women showed worst scores for emotional eating, PHQ-9 and PSQI (Supplementary Table I). On the other hand, sense of coherence was higher for men in comparison to women (Table 2). Percentage of emotional eaters or very emotional eaters were higher among women in comparison to men (29.09% vs. 17.08%) (Supplementary Table I). Additionally, women more often showed signs of depression (Table 2). Finally, in comparison to men, women more often reported having poor sleep quality (Table 2).
Mental health scores by gender.
| Women (n=5943, 70.53%) | Men (n=2483, 29.46%) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | Mean | SD | Median | IQR | n | % | Mean | SD | Median | IQR | |
| EEQ | 8.04 | 5.83 | 7 | (4-11) | 6.31 | 5.04 | 5 | (2-9) | ||||
| Non-emotional eater | 2413 | 40.60 | 1281 | 51.59 | ||||||||
| Low emotional eater | 1861 | 31.31 | 778 | 31.33 | ||||||||
| Emotional eater | 1429 | 24.05 | 385 | 15.51 | ||||||||
| Very emotional eater | 240 | 4.04 | 39 | 1.57 | ||||||||
| PHQ-9 | 5.15 | 5.10 | 4 | (1-8) | 4.09 | 4.89 | 2 | (0-6) | ||||
| Healthy | 4428 | 74.51 | 1984 | 79.90 | ||||||||
| Major depression | 158 | 2.66 | 58 | 2.34 | ||||||||
| Minor depression | 1357 | 22.83 | 441 | 17.76 | ||||||||
| PHQ-9 | 4.91 | 3.28 | 5 | (2-7) | 4.66 | 3.23 | 4 | (2-7) | ||||
| Good quality | 3582 | 60.27 | 1539 | 64.36 | ||||||||
| Poor quality | 2361 | 39.73 | 885 | 35.64 | ||||||||
| SOC-15 | 60.03 | 9.25 | 61 | (54-67) | 60.64 | 9.65 | 62 | (55-68) | ||||
EEQ: Emotional Eater Questionnaire; IQR: interquartil range; PHQ-9: Patient Health Questionnaire 9; PSQI: Pittsburgh Sleep Quality Index by sex; SD: standard deviation; SOC-15: Sense of Coherence 15.
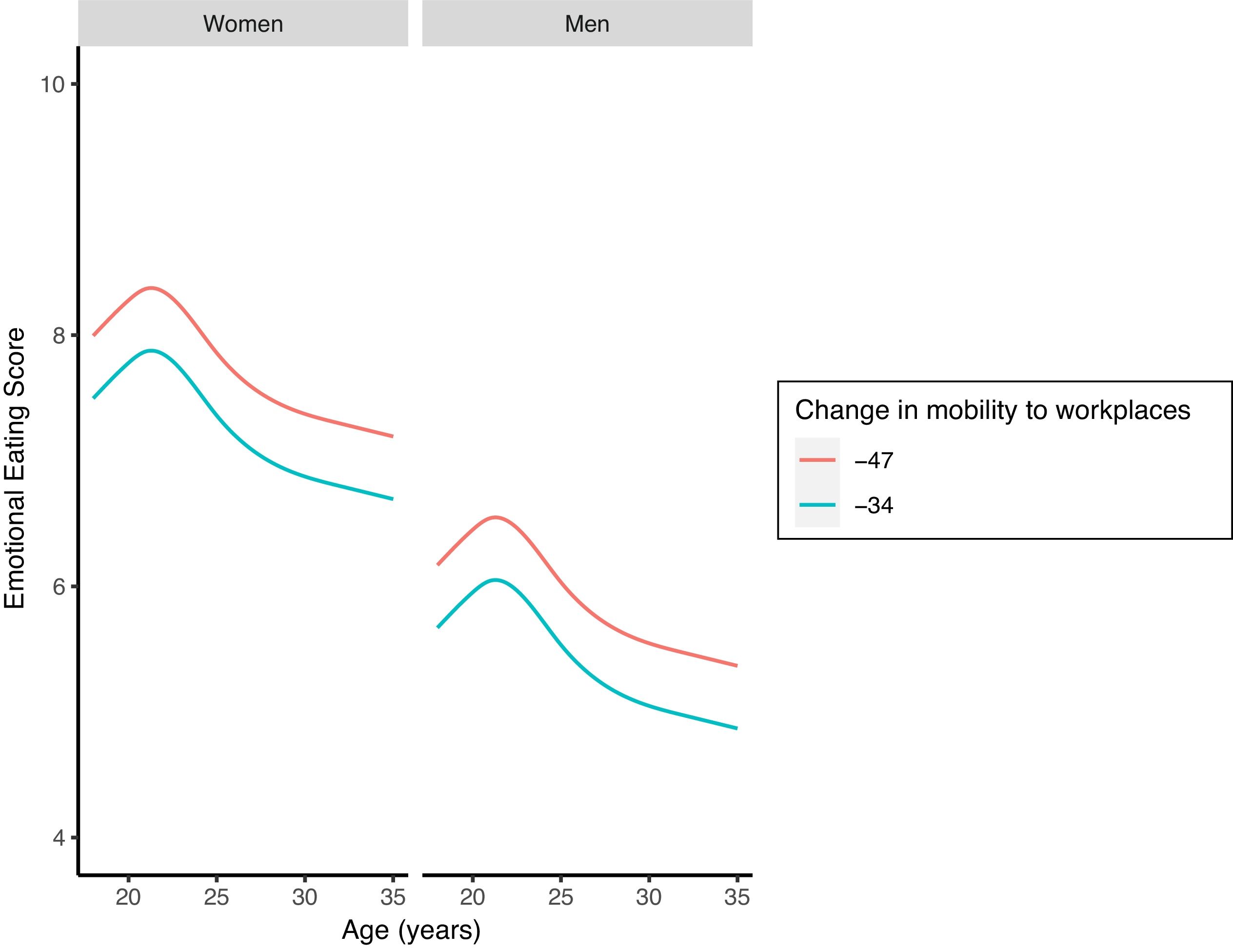
Both, mobility change to workplaces (df=1, F=16.40, p<0.001) and groceries/pharmacies (df=1, F=4.64, p=0.031) were significantly associated to emotional eating behavior. In this way, a higher restriction of mobility for both places was associated with less healthy eating behavior. Emotional eating behavior was also significantly associated to gender (df=1, F=186.67, p <0.001) and age (df=4, F=25.24, p <0.001). For instance, women as well as youngsters showed significantly less healthy eating behavior than men and older respondents (Fig. 1 and Supplementary Fig. II). Model information, adjusted predicted emotional eating behavior scores and their 95% confidence intervals for predictors are showed in Supplementary Table I.

Eating behavior by age, gender and mobility. Predicted means are showed for mobility to workplaces. Red line indicates higher restriction (3rd quantile) and the blue lower restriction (1st quantile). Confidence intervals were omitted to facilitate visualization, but can be consulted in Supplementary Table I.
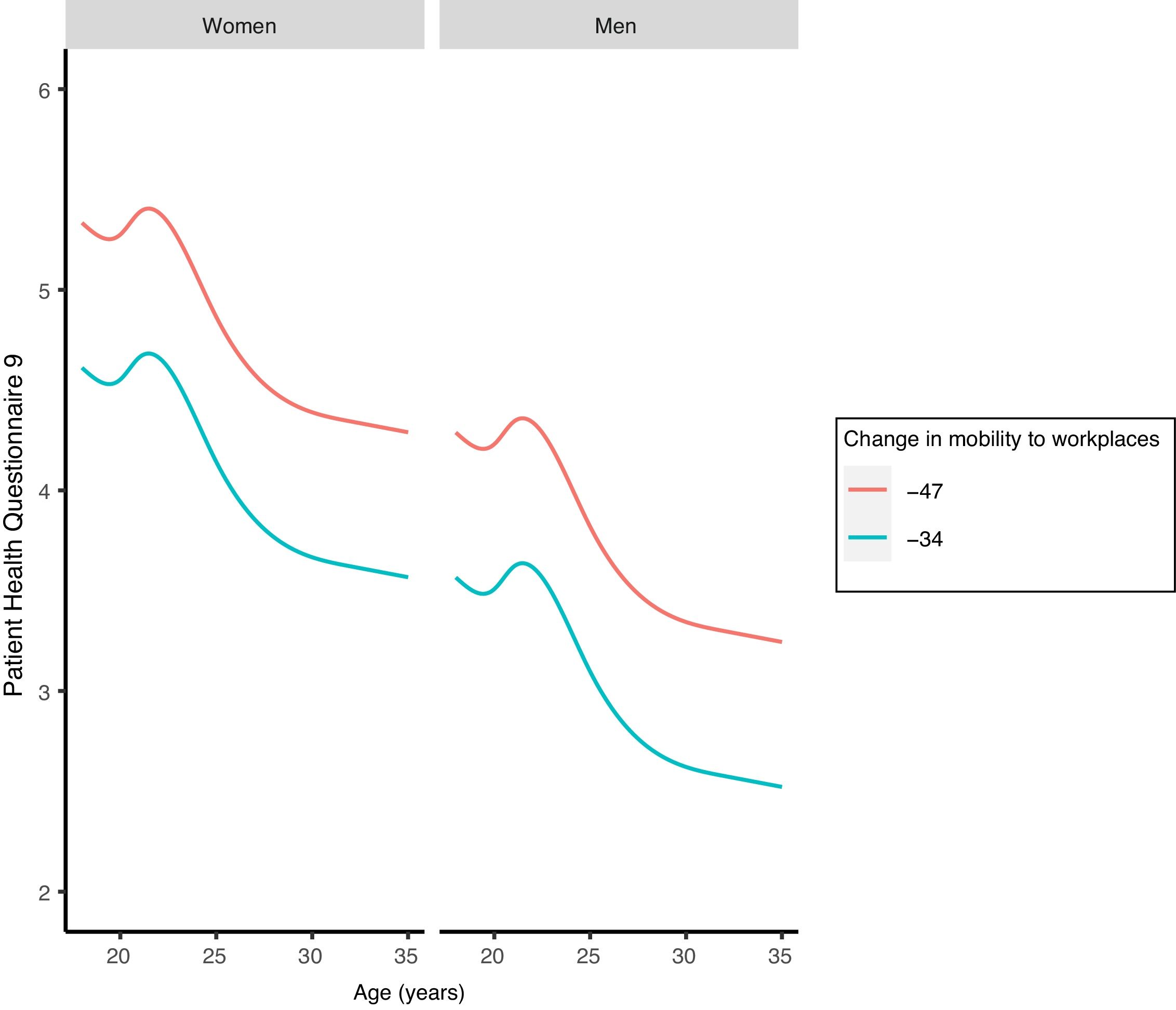
Both, mobility change to workplaces (df=1, F=13.41, p <0.001) and groceries/pharmacies (df=1, F=7.93, p=0.005) were significantly associated to depression. In this way, a higher restriction of mobility for both places was associated with a higher score for depressive symptoms. Depressive symptoms were also significantly associated to gender (df=1, F=69.10, p <0.001) and age (df=4, F=10.78, p <0.001). For instance, women as well as youngsters more often showed depressive symptoms than men and older respondents (Fig. 2 and Supplementary Fig. III). Model information, adjusted predicted PHQ-9 scores and their 95% confidence intervals for predictors are showed in Supplementary Table I.

Depression by age, gender and mobility. Predicted means are showed for mobility to workplaces. Red line indicates higher restriction (3rd quantile) and the blue lower restriction (1st quantile). Confidence intervals were omitted to facilitate visualization, but can be consulted in Supplementary Table I.
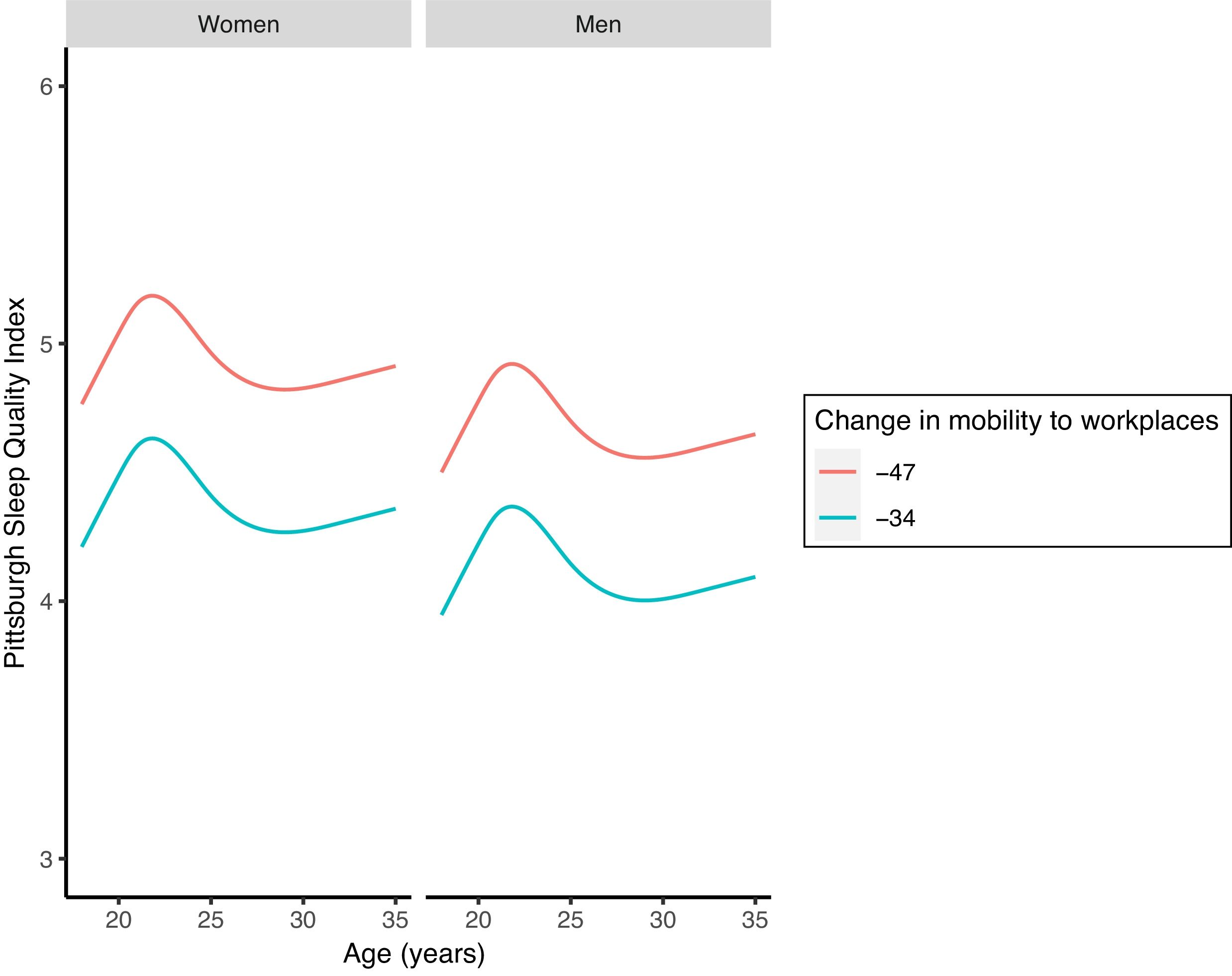
Both, mobility change to workplaces (df=1, F=13.41, p <0.001) and groceries/pharmacies (df=1, F=7.93, p=0.005) were significantly associated to sleep quality. In this way, a higher restriction of mobility for both places was associated with a worse sleep quality. Sleep quality was also significantly associated to gender (df=1, F=7.48, p=0.006), but not to age (df=4, F=1.98, p=0.094). In comparison to men, women showed higher PSQI than men, suggesting worse sleep quality (Fig. 3 and Supplementary Fig. IV). Model information, adjusted predicted PSQI scores and their 95% confidence intervals for predictors are showed in Supplementary Table I.

Sleep quality by age, gender and mobility change. Predicted means are showed for mobility to workplaces. Red line indicates higher restriction (3rd quantile) and the blue lower restriction (1st quantile). Confidence intervals were omitted to facilitate visualization, but can be consulted in Supplementary Table I.
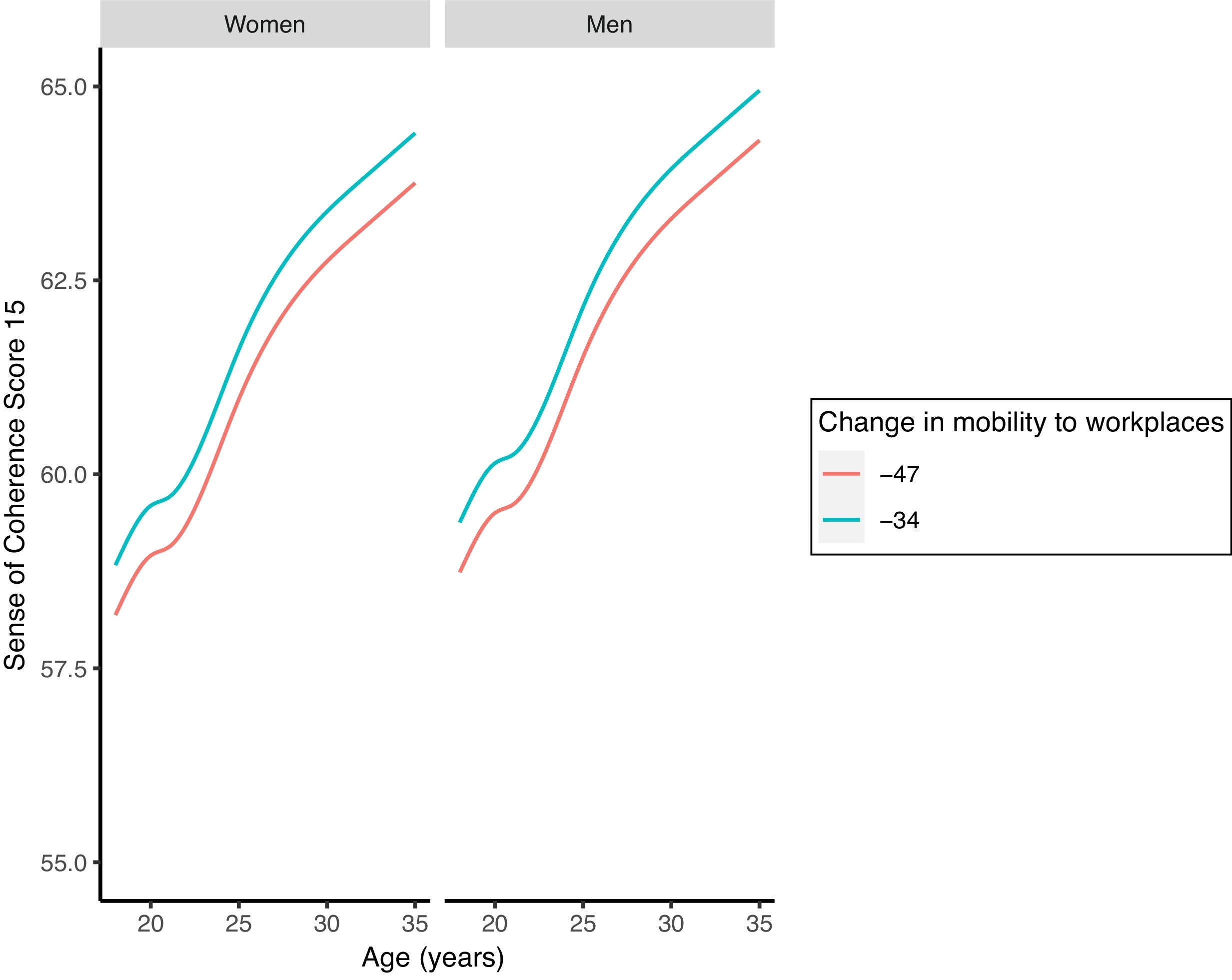
Both, mobility change to workplaces (df=1, F=4.31, p=0.038) and groceries/pharmacies (df=1, F=4.03, p=0.045) were significantly associated to sense of coherence. In this way, a higher restriction of mobility for both places was associated with a lower score for sense of coherence. Sense of coherence was also significantly associated to age (df=4, F=67.79, p <0.001) but not to gender (df=1, F=1.57, p=0.210). Youngsters showed significantly lower sense of coherence than older respondents (Fig. 4 and Supplementary Fig. V). Model information, adjusted predicted SOC-15 scores and their 95% confidence intervals for predictors are showed in Supplementary Table I.

Sense of coherence by age, gender and mobility change. Predicted means are showed for mobility to workplaces. Red line indicates higher restriction (3rd quantile) and the blue lower restriction (1st quantile). Confidence intervals were omitted to facilitate visualization, but can be consulted in Supplementary Table I.
This is the first study to evaluate mental health in Ecuadorian young adults during the COVID-19 pandemic, addressing four aspects of mental health: emotional eating, sleep quality, depression and sense of coherence as a proxy of resilience. We found that emotional eating, poor sleep quality, depression and a low sense of coherence were related to higher mobility restriction. Women and youngsters were more vulnerable to the detrimental effects of confinement on mental health.
Mental health and mobility restrictionThe fact that lock-down measures negatively influence mental health is supported by previous evidence.23,24 However, the present is one of the few that took into account compliance to confinement, although indirectly measured. Among young adults, factors associated with higher mental distress due the confinement might be related not only to their inner psychological characteristics but also to adverse socioeconomic circumstances derived from the pandemic.24–26 In this line, previous research showed that individuals who perceive COVID-19 as emotionally threatening, feel lonely or are less resilient exhibit higher mental distress.24
On the other hand, it is also likely that mental distress emerges as result of the damaging effects of distancing measures and stay-at-home orders on the economic situation of families.27 Indeed, economic crisis may affect mental health either by increasing risk factors (i.e., unemployment, indebtedness, loss of socioeconomic position) or by weakening protective factors (i.e., job security and welfare programs).24 Moreover, economic crisis has been associated to increased need for general help sought for mental health problems, higher use of prescription drugs and increased hospital admissions for mental disorders.24
Mental health of women and youngstersOur findings and those of other studies suggest that women are in greater risk of suffering depression, as well as sleep and eating disorders in comparison to men.7,23,24,28,29 Higher vulnerability of women to experience mental distress is not well understood, but it probably relates to gender differences regarding access to health care and gender expected roles in society and economic production.30 In comparison to men, women generally have less access to health care and their diseases diagnosed later, which as a result cause them to be treated less successfully. Additionally, women usually have to balance work and household tasks being more vulnerable to suffer psychological burden.30 On the other hand, it is also know the influence of sex-based differences on certain mental health outcomes, which are not taken into account to provide medical treatment to women.30,31
Similarly to other studies, we also found an association between mental health distress and age during the COVID-19 pandemic.7,32,33 In general, it seems that youngsters had suffered higher mental health burden due to social isolation than did older people during confinement. In the context of the pandemic youngster's vulnerability might be explained by the abrupt and drastic change in their daily life-style. Sudden isolation and disintegration of their social networks could have prompted feelings of loneliness, which has been linked to mental health problems such as stress and anxiety in the future.34 Moreover, during the lock-down youngsters, who already are at higher risk of mental health problems and self-harm than other age groups, have been exposed to situations that exacerbate self-harm and suicide ideation, including feeling trapped, defeated and hopeless.34
Implications strengths and limitationsThe analyzes carried out in the population regarding health-disease phenomena derived from confinement require the attention of the scientific community for the formulation of adequate health policies. In this way, our findings highlight the need of promoting resilience specially among the most vulnerable population, i.e. women and youngsters in order to help them overcome the devastating consequences of the pandemic.35 Moreover, our study confirms the importance of discussing the implementation of gender-specific health measures to monitor and address the negative effects of the pandemic.
Our study is important because it is the first one conducted in Ecuador including near 9000 participants. Moreover, it provides for the first time an insight on the association of lock-down and mental health of young adults and differences among women and men. However, our study has several limitations: first, although we evaluated changes in mobility for the population in general, we failed to extract information on personal compliance to the mandatory confinement; second, our study lacks of external validity since participants came from a non-probabilistic sampling, and therefore our findings can not be generalized to the general population; and finally, due to our study design we were not able to establish a causal relationship between mobility restrictions, nor to address the impact of other important factors such as environmental context.
Data availabilityData will be available upon request to the corresponding author.
Mental health has been seriously affected by the COVID-19 pandemic.
What does this study add to the literature?Emotional eating, poor sleep quality, depression and a low sense of coherence are associated to higher mobility restriction. Women and youngsters are more vulnerable to the effects of confinement.
What are the implications of the results?Health policies sensitive to gender differences should be implement to strength resilience among young adults.
Leila P. García.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsT.V. Carpio-Arias: conceptualization, methodology, formal analysis, investigation, data curation, writing, original draft, writing, review and editing. J.S. Piedra-Andrade: formal analysis, data curation, writing original draft, review and editing. T.M. Nicolalde-Cifuentes: conceptualization, data curation, writing original draft, review and editing. M.V. Padilla-Samaniego: conceptualization, writing original draft, review and editing. E.C. Tapia-Veloz: design of the study, acquisition and interpretation of the data. M.F. Vinueza-Veloz: conceptualization, methodology, formal analysis, investigation, data curation, writing, original draft, writing, review and editing. All authors were involved in drafting of the work or revising it critically for important intellectual content. All authors approved the final version to be published and agree to be accountable for all aspects of the work.
AcknowledgmentsThe authors thank the ESPOCH Research Institute (IDI) for the support provided. Special thanks also to Dr. Maria Paulina Robalino Valdivieso and Dr. Hugo Moreno for their support.
FundingNone.
Conflicts of interestNone.












