



To determine whether an intervention based on patient-practitioner communication is more effective than usual care in improving diabetes self-management in patients with type 2 diabetes with low educational level.
Methods12-month, pragmatic cluster randomised controlled trial. Nine physicians and 184 patients registered at two practices in a deprived area of Granada (Andalusia, Spain) participated in the study. Adult patients with type 2 diabetes, low educational level and glycated haemoglobin (HbA1c) > 7% (53.01 mmol/mol) were eligible. The physicians in the intervention group received training on communication skills and the use of a tool for monitoring glycaemic control and providing feedback to patients. The control group continued standard care. The primary outcome was difference in HbA1c after 12 months. Dyslipidaemia, blood pressure, body mass index and waist circumference were also assessed as secondary outcomes. Two-level (patient and provider) regression analyses controlling for sex, social support and comorbidity were conducted.
ResultsThe HbA1c levels at 12 months decreased in both groups. Multilevel analysis showed a greater improvement in the intervention group (between-group HbA1c difference= 0.16; p=0.049). No statistically significant differences between groups were observed for dyslipidaemia, blood pressure, body mass index and waist circumference.
ConclusionsIn this pragmatic study, a simple and inexpensive intervention delivered in primary care showed a modest benefit in glycaemic control compared with usual care, although no effect was observed in the secondary outcomes. Further research is needed to design and assess interventions to promote diabetes self-management in socially vulnerable patients.
Determinar si una intervención basada en la comunicación médico-paciente es más efectiva que la atención habitual en la mejora del autocontrol de la diabetes en pacientes con diabetes tipo 2 con bajo nivel educativo.
MétodosEnsayo controlado aleatorizado pragmático por agrupación de 12 meses. Participaron en el estudio nueve profesionales médicos y 184 pacientes registrados/as en dos centros de salud en una zona pobre de Granada (Andalucía, España). Criterios de inclusión: adultos/as con diagnóstico de diabetes tipo 2, con bajo nivel educativo y hemoglobina glucosilada (HbA1c) >7% (53,01mmol/mol). Los/las sanitarios/as del grupo de intervención recibieron entrenamiento en las habilidades de comunicación y en el uso de una herramienta para la monitorización del control glucémico y proporcionar información a los/las pacientes. El grupo control continuó la atención estándar. La medida de resultado fue la diferencia en la HbA1c después de 12 meses. Otras medidas de resultado fueron la dislipidemia, la hipertensión arterial, el índice de masa corporal y la circunferencia abdominal. Se realizó una regresión con dos niveles (paciente y proveedor) controlando por sexo, apoyo social y comorbilidad.
ResultadosLa HbA1c a los 12 meses disminuyó en ambos grupos. El análisis multinivel mostró una mayor mejoría en el grupo de intervención (diferencia entre grupos HbA1c=−0,16; p=0,049). No se observaron diferencias estadísticamente significativas entre los grupos para la dislipidemia, la hipertensión arterial, el índice de masa corporal y la circunferencia abdominal.
ConclusionesEste estudio pragmático mostró que una intervención sencilla y de bajo coste ofrecida en atención primaria alcanzó un modesto beneficio en el control glucémico en comparación con la atención habitual, aunque no se observó ningún efecto en los resultados secundarios. Se necesita más investigación para diseñar y evaluar intervenciones para promover el autocontrol de la diabetes en pacientes socialmente vulnerables.
The prevalence of type 2 diabetes mellitus (T2DM) rapidly rose over the past three decades worldwide.1 In Spain, the prevalence of T2DM (2012) is 14%,2 and the mortality rate associated with the condition is 18.3/100,000 men and 24.9/100,000 in women.3
T2DM does not impact all population groups equally, existing important differences according to sex, socioeconomic status and ethnicity.3–5 Socially disadvantaged groups are more exposed to obesogenic environments, and experience more difficulties in adopting healthy lifestyles (i.e. eating habits, physical activity, etc.), caused by social determinants of health.5–12 Several studies have observed an inverse association between educational level and worse prognosis of T2DM,3–5 which has been attributed to increased difficulties in processing oral communication,13 less awareness of the importance of diabetes self-management14 and less cohesive support networks14,15 in patients with a lower educational level.
A number of studies have examined the effectiveness of different types of interventions specially designed to improve diabetes self-management in socially vulnerable patients.15–19 Most of these interventions consisted in the use of psychoeducational strategies and targeted ethnic minorities or groups with lower socioeconomic status. Although, there was a great diversity of procedures and type of interventions, a moderate reduction of HbA1c outcome were observed in these systematic reviews.15–19
Evidence suggests that adequate patient-practitioner communication has a number of different benefits, including positive effects on patients’ compliance with medical recommendations.20 However, there is a scarce evidence available regarding the potential of interventions based on improving patient-practitioner communication to improve diabetes self-management in patients with low educational levels, much more if the intervention was performed by a medical doctor. Thus, Chapin et al.21 evaluated the effectiveness of an intervention consisting in the use of a visual tool to provide feedback to patients by displaying glycosylated haemoglobin values graphically over time, and relating them to the patients’ self-reported self-management activities. The authors observed that after the intervention 51% of the patients achieved adequate glycaemic control (HbA1c <7%, 53.01mmol/mol). Because its low cost of the intervention and easy transferability to routine clinical practice, we decided to adapt this intervention, implement it in a primary care setting in Spain, and evaluate its impact on patients’ health.
The aim of this study was to test whether an intervention based on improving patient-practitioner communication, compared with standardised usual care can improve diabetes self-management in patients with a low educational level.
MethodsA detailed description of the methodology used of this study is available elsewhere.22
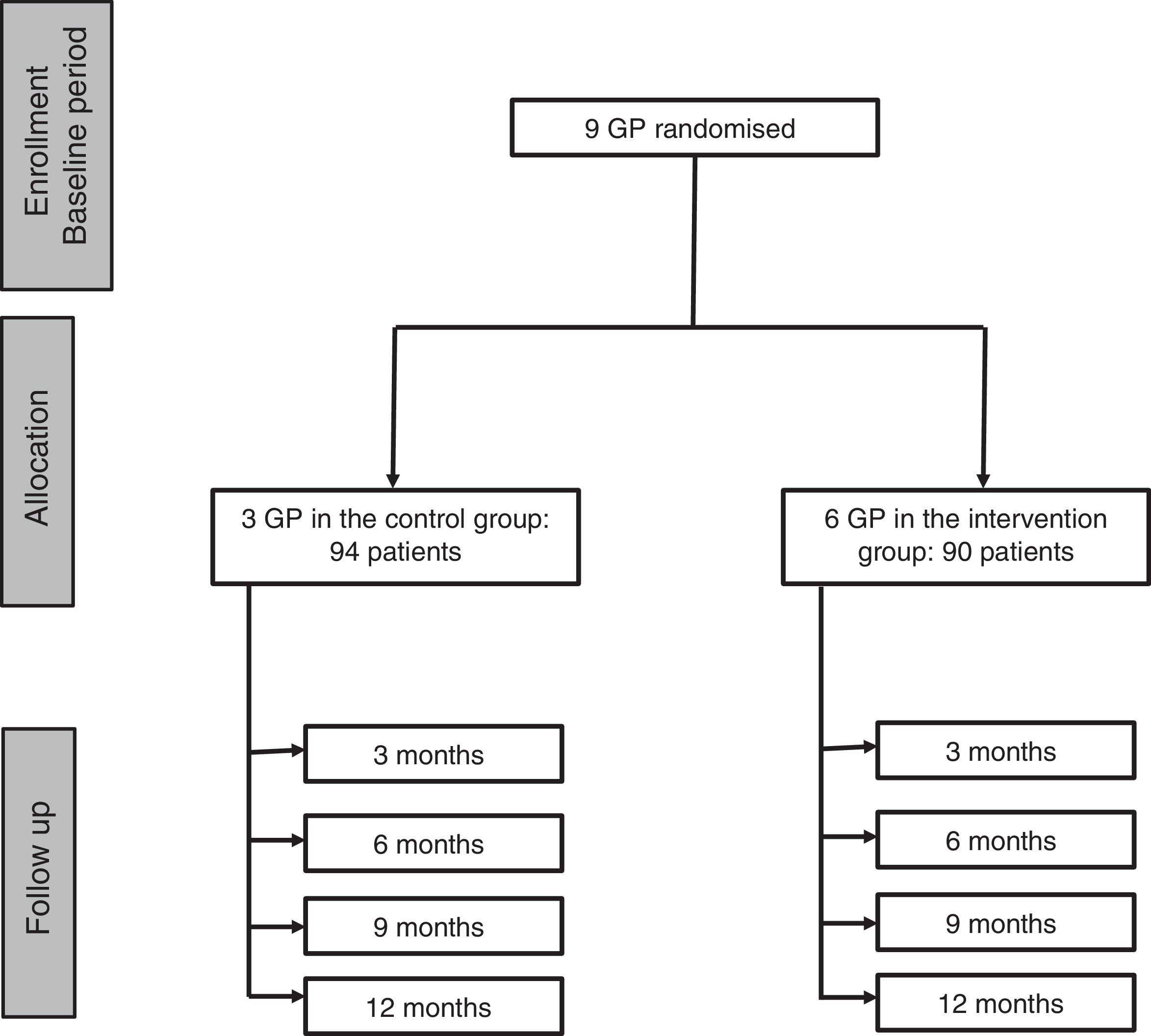
Study designPragmatic cluster randomised controlled trial (Fig. 1).
Setting
The study was conducted in two general practices in the city of Granada (Andalusia, Spain). A total of nine general practitioners (GPs) in the two practices participated in this study, those practices were selected because they were located in a highly deprived area. We used computerised randomisation to allocate the GPs to the intervention or control group.
ParticipantsPatients were eligible if they had T2DM, were aged ≥18 years, had and HbA1c level >7% (53.01mmol/mol) at the assessment visit, and had a low educational level (no studies or only primary school education). Exclusion criteria were having a serious physical or mental health condition that would prevent to follow trial procedures or being taking part in a different study.
Sample sizeThe sample size was calculated assuming that at the end of the intervention 10% of the control group and 30% of intervention group A would achieve improved diabetes control (with HbA1c values falling to below 7%). So initially, we attempted to achieve a sample size of 90 patients in each group (control and intervention) in order to provide a statistical power of 89.4% to detect significant differences in the percentage of controlled diabetic patients in both groups.
InterventionThe intervention, performed by participant practices, consisted in using a diabetes self-management record sheet (DSMRS) as part of the consultation. GPs and patients work together to complete the DSMRS, which included two parts: 1) a graph showing the patient's previous HbA1c levels, and 2) five patient-reported items on self-management activities.21 The aim of the DSMRS was to prompt discussions/reflections about the importance of adequate diabetes self-management and its impact on glycaemic control and in turn on diabetes-related complications. At the end of the session, patients were offered a take home copy of the DSMRS and encouraged discuss it with their relatives. The intervention was delivered every 3 months, during the course of a year (i.e. four sessions by the end of the study period). To standardise the intervention style, the GPs received training in cognitive, emotional and communication aspects. In addition, every six months a joint meeting of researchers and GPs was held to address potential problems, monitor the progress of the study and ensure adherence to the study protocol.
A subgroup of patients received telephone reinforcement, which specifically focused on physical activity and healthy eating and was based on psycho-educational and problem-solving strategies. Telephone reinforcements were carried out by a member of the research team who was previously trained in behaviour change techniques and motivational interviewing skills.
Control groupGPs allocated to the control group provided standard care, which included regular follow-up appointments every 3 months.
ProcedureAll stages of this study (recruitment, baseline measurements, interventions and final measurements) were carried out at the routine three-monthly appointments. This approach was used to minimise the cost of the study and to reduce the burden for patients.
Demographics and outcome measures: participants self-reported their sex, date of birth, ethnicity, number of children, educational level, and social support, which was measured using a validated instrument.23 The primary outcome variable was HbA1c; LDL and HDL cholesterol, triglycerides, blood pressure, body mass index (BMI) and abdominal circumference were examined as secondary outcomes. Outcome measures were collected at baseline, every 3 months during the intervention period, and post-intervention. All biochemical assays adhered to Spanish national guidelines. Laboratory personnel were blinded to group assignment. The source of this information was the digital clinical record (Diraya).
This study was approved by the Andalusian School of Public Health Ethics Committee. Written informed consent was obtained from all patients who met the eligibility criteria and agreed to participate in the study.
AnalysisDescriptive statistics were calculated. Continuous variables were expressed as mean and standard deviation; categorical variables were expressed as counts and percentages. A bivariate analysis was carried out to analyse the effect of the intervention according to the different sociodemographic variables studied, using logistic regression analysis with HbA1c <7% (53.01mmol/mol) and ≥7% (53.01mmol/mol) as the dependent variable.
Missing data were assessed by examining patterns in the main variables. No pattern was found, so we concluded that the missing data could be random and used the “last observation carried forward” procedure, assuming that the last observation is representative of the missing value. Individuals with missing values did not improve nor deteriorate.
Our analytical approach made use of all available data, making this an intention-to-treat analysis. Full information maximum likelihood estimation was used. This form of estimation provides unbiased estimates under the less restrictive assumption of data missing at random, which allows the probability of data being missing to be dependent of outcome and predictors. To take missing data further into account, we performed additional analyses where informativeness of missing data patterns were investigated as potential confounding factors. As formal dropout was not recorded, we treated post-treatment data missing due to dropout and data missing for other reasons as equivalent.
Due to the hierarchical nature of data and characteristics of the panel data (four measurements of the dependent variable), two levels (patient and provider) mixed effect models were used to examine whether the two groups of patients had differential rates of change over time for HbA1c and secondary outcomes (i.e. time by group interactions). This analyses was also repited for other variables (HDL-c (mg/dL), LDL-c (mg/dL), triglycerides (mg/dL), systolic blood pressure (mmHg), diastolic blood pressure (mmHg), body mass index and abdominal circumference (cm), which were also controlled for comorbidity, sex and social support. Finally, to evaluate a possible dosage effect, the number of sessions attended was examined as a predictor of HbA1c. The level of significance was set at 5% (p <0.05), and all statistical analyses were performed using Stata.v13.
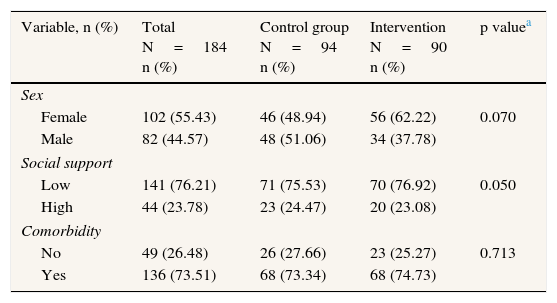
ResultsParticipant characteristicsBetween January and October 2012, 200 patients were invited to take part in the study, of them 184 (92%) accepted and were recruited (90 in the intervention and 94 in the control group) and 108 (58.69%) participants ended the follow-up. Baseline personal and clinical characteristics were well balanced between the groups (Table 1). 55.4% of the participants were women (mean age=62; mean number of children=3.2). Almost three quarters of the patients had low social support (74.9%) and at least one comorbidity (73.91%). Mean HbA1c was 8.77% (72.35mmol/mol), whereas mean LDL and HDL were 115.72mg/dL and 45.37mg/dL, respectively. Mean systolic and diastolic pressure were 130.25mmHg and 77.17mmHg. Mean BMI was 33.7.
Baseline characteristics of participants, by study group.
| Variable, n (%) | Total N=184 n (%) | Control group N=94 n (%) | Intervention N=90 n (%) | p valuea |
|---|---|---|---|---|
| Sex | ||||
| Female | 102 (55.43) | 46 (48.94) | 56 (62.22) | 0.070 |
| Male | 82 (44.57) | 48 (51.06) | 34 (37.78) | |
| Social support | ||||
| Low | 141 (76.21) | 71 (75.53) | 70 (76.92) | 0.050 |
| High | 44 (23.78) | 23 (24.47) | 20 (23.08) | |
| Comorbidity | ||||
| No | 49 (26.48) | 26 (27.66) | 23 (25.27) | 0.713 |
| Yes | 136 (73.51) | 68 (73.34) | 68 (74.73) | |
| Mean (SD) | Mean (SD) | Mean (SD) | p valueb | |
|---|---|---|---|---|
| Number of children | 3.22 (0.16) | 2.92 (0.18) | 3.54 (0.27) | 0.973 |
| Age (years) | 61.67 (0.91) | 62.27 (1.17) | 61.04 (1.41) | 0.253 |
| HbA1c (%) | 8.77 (0.11) | 8.93 (0.14) | 8.89 (0.18) | 0.292 |
| HDL (mg/dL) | 45.37 (2.02) | 51.47 (3.38) | 42.42 (2.37) | 0.358 |
| LDL (mg/dL) | 115.72 (5.01) | 122.53 (7.90) | 112.53 (6.36) | 0.357 |
| Triglycerides (mg/dL) | 112.62 (4.93) | 106.51 (6.35) | 119.15 (7.58) | 0.201 |
| Systolic blood pressure (mmHg) | 130.25 (2.48) | 125.36 (4.37) | 132.26 (2.98) | 0.209 |
| Diastolic blood pressure (mmHg) | 77.17 (1.30) | 75.14 (2.84) | 78.00 (1.42) | 0.324 |
| Body mass index (kg/m2) | 33.71 (0.72) | 33.51 (1.40) | 33.81 (0.85) | 0.851 |
| Abdominal circumference (cm) | 107.51 (1.22) | 106.17(1.50) | 110.41 (2.02) | 0.106 |
HbA1c: glycated haemoglobin; HDL: high density lipoprotein; LDL: low density lipoprotein; SD: standard deviation.
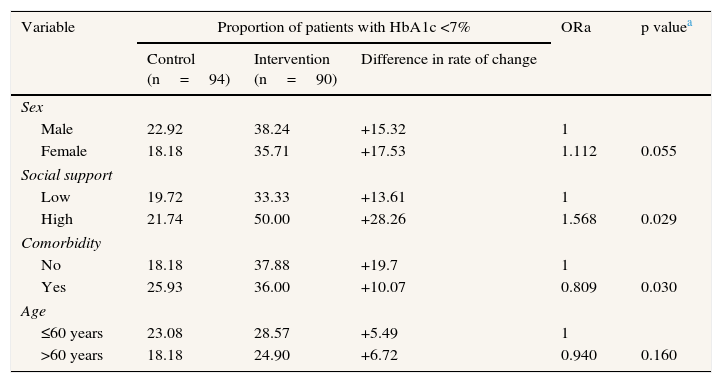
All participants completed at least one of the four sessions. At the end of the study 34.2% of patients in the intervention group and 23.2% in the control group achieved adequate glycaemic control (HbA1c <7%, 53.01mmol/mol) (Table 2). Subgroup analysis revealed that patients with higher social support (odds ratio [OR]=1.57) and without comorbidities (OR=1.24) were significantly more likely to achieve adequate glycaemic control. No statistically significant differences between sex and age groups were observed.
Proportion of patients who achieved adequate glycaemic control at the end of the study.
| Variable | Proportion of patients with HbA1c <7% | ORa | p valuea | ||
|---|---|---|---|---|---|
| Control (n=94) | Intervention (n=90) | Difference in rate of change | |||
| Sex | |||||
| Male | 22.92 | 38.24 | +15.32 | 1 | |
| Female | 18.18 | 35.71 | +17.53 | 1.112 | 0.055 |
| Social support | |||||
| Low | 19.72 | 33.33 | +13.61 | 1 | |
| High | 21.74 | 50.00 | +28.26 | 1.568 | 0.029 |
| Comorbidity | |||||
| No | 18.18 | 37.88 | +19.7 | 1 | |
| Yes | 25.93 | 36.00 | +10.07 | 0.809 | 0.030 |
| Age | |||||
| ≤60 years | 23.08 | 28.57 | +5.49 | 1 | |
| >60 years | 18.18 | 24.90 | +6.72 | 0.940 | 0.160 |
ORa: adjusted odds ratio.
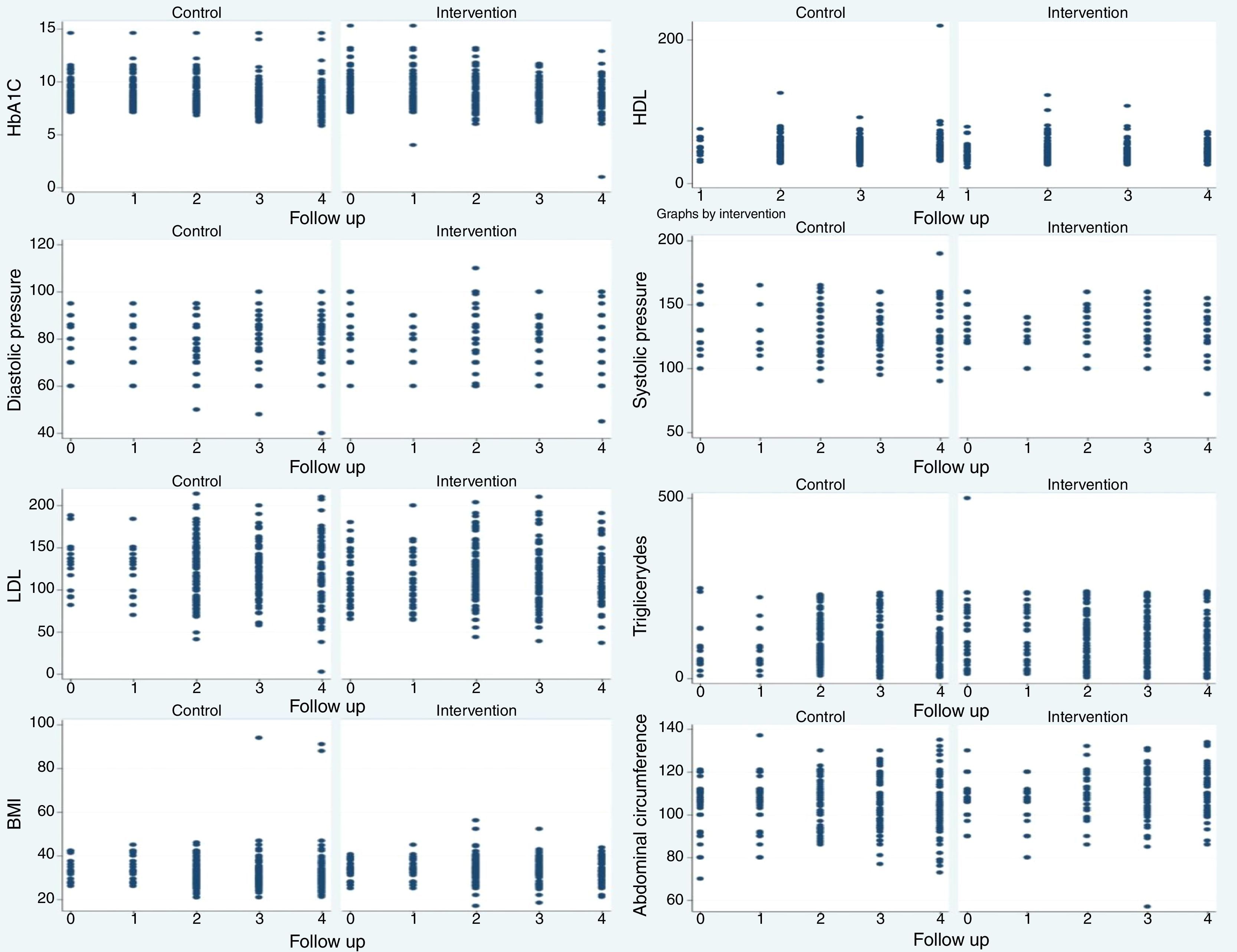
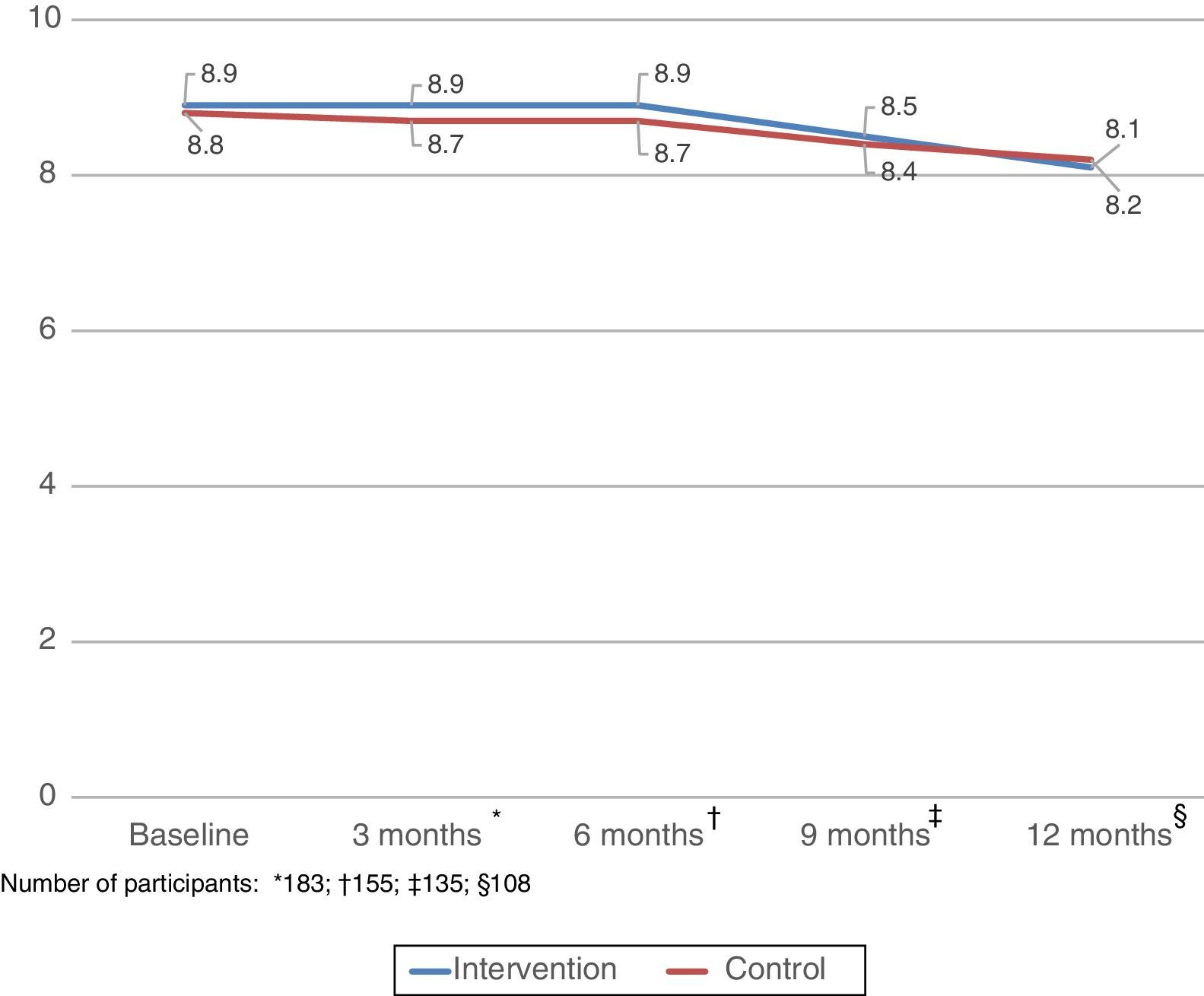
Figure 2 shows the distribution of HbA1c, blood pressure, lipidemia, BMI and abdominal circumference at 3, 6, 9 and 12 months. HbA1c decreased over the study period in both groups, especially after sixth months of follow up. Although the reduction in HbA1c levels was statistically significant (p <0.001) in both groups, differences were higher in the intervention (from 8.9% to 8.1%) than in the control group (from 8.8% to 8.2%) (Fig. 3).


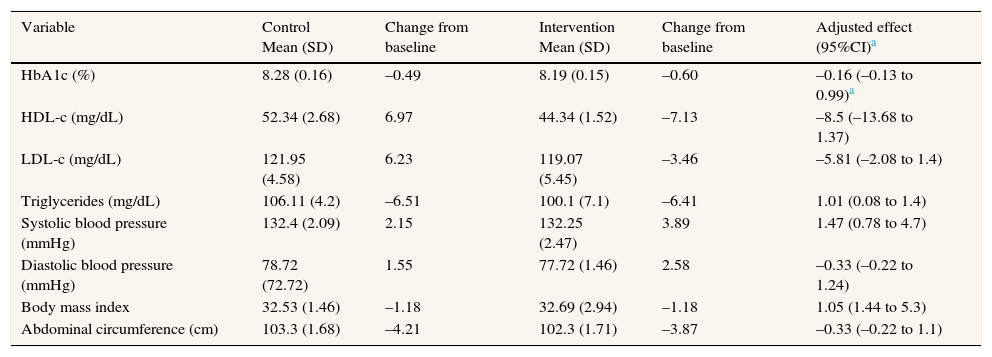
The multilevel analysis (Table 3) showed a 0.16% decrease (95%CI: 0.13-0.99) in mean HbA1c in the intervention group compared to the control group. No statistically significant differences between groups were observed for blood pressure, HDL, LDL, triglycerides, BMI and abdominal circumference. The random-effects analysis of the physicians was not significant. Attendance was a significant predictor of HbA1c (β=−0.2, p <0.001), suggesting that each additional session patients attended was associated with a 0.2% decrease in HbA1c.
Differences in outcomes before and after the intervention and between intervention and control group.
| Variable | Control Mean (SD) | Change from baseline | Intervention Mean (SD) | Change from baseline | Adjusted effect (95%CI)a |
|---|---|---|---|---|---|
| HbA1c (%) | 8.28 (0.16) | –0.49 | 8.19 (0.15) | –0.60 | –0.16 (–0.13 to 0.99)a |
| HDL-c (mg/dL) | 52.34 (2.68) | 6.97 | 44.34 (1.52) | –7.13 | –8.5 (–13.68 to 1.37) |
| LDL-c (mg/dL) | 121.95 (4.58) | 6.23 | 119.07 (5.45) | –3.46 | –5.81 (–2.08 to 1.4) |
| Triglycerides (mg/dL) | 106.11 (4.2) | –6.51 | 100.1 (7.1) | –6.41 | 1.01 (0.08 to 1.4) |
| Systolic blood pressure (mmHg) | 132.4 (2.09) | 2.15 | 132.25 (2.47) | 3.89 | 1.47 (0.78 to 4.7) |
| Diastolic blood pressure (mmHg) | 78.72 (72.72) | 1.55 | 77.72 (1.46) | 2.58 | –0.33 (–0.22 to 1.24) |
| Body mass index | 32.53 (1.46) | –1.18 | 32.69 (2.94) | –1.18 | 1.05 (1.44 to 5.3) |
| Abdominal circumference (cm) | 103.3 (1.68) | –4.21 | 102.3 (1.71) | –3.87 | –0.33 (–0.22 to 1.1) |
CI: confidence interval; HbA1c: glycated haemoglobin; HDL-c: high density lipoprotein cholesterol; LDL-c: low density lipoprotein cholesterol; SD: standard deviation.
This study examined the effectiveness of an intervention to improve diabetes self-management in patients with low educational level and inadequate glycaemic control by improving patient-provider communication. Patients both from the intervention and control group, significantly improved their glycaemic control after the study period. However, a higher reduction in HbA1c was observed in the intervention group. The intervention produced higher positive impact in those patients with higher levels of social support and without comorbidities. A dosage effect was observed, with each additional session being associated with a 0.2% decrease in HbA1c.
This the first study conducted in Spain that implemented and evaluated an intervention to improve diabetes self-management in a group of socially vulnerable patients. The study presents several methodological strengths, namely an adequate follow-up of outcome measures throughout the study period (including not only baseline and endpoint measures, but also every three months). Furthermore, randomization was conducted at the GP (and not patient) level, which prevented potential contamination bias. Furthermore, potential variability between GPs (clustering effect) was adequately controlled in our multilevel analysis. The HbA1c reductions were more notable after sixth months of follow up, these results could be justified by the need for a minimum number of session to achieve an intervention effect, although performance bias could not be excluded, because the HbA1c measures were performed every 3 months, instead each 6 months as usual care.
However, the study also has several limitations. First, although two intervention groups were initially considered (with and without telephone reinforcement),22 we experienced considerable difficulties in reaching and delivering the reinforcement to most of them. Because of that, we finally decided to analyse together the groups and therefore the specific effect of the reinforcement could not be formally evaluated. Second, although the proportion of patients in the intervention and control group was similar, the number providers in the intervention group (six GPs) was higher than in the control group (with only three GPs). However, results from the multilevel analysis suggested that the variability attributable to the provider level (cluster effect) was not significant, and therefore it is unlikely that the unbalanced number of providers per group has biased our results. Third, it was not possible to carry out a “double blind” study because the GPs themselves were the responsible for delivering the intervention. Finally, we cannot rule out the possibility that the GPs and/or patients might have modified their usual behaviour during the study period because they knew they were being studied (Hawthorn effect), which would at least partially explain the positive changes observed in the control group.
Although statistically significant, the reduction of HbA1c observed after the intervention is not clinically relevant, and it is substantially lower than the effect reported by Chapin et al.21 in their previous study. This could reflect the differences between control groups in both two studies. Thus, although mean HbA1c decreased in the control groups of both studies, the reduction was substantially higher in our study (−0.38%) than in the study by Chapin et al.21 (−0.18%). Moreover, it is worth noting that the number of sessions the participants attended was directly associated with the impact of our intervention, and therefore the modest effect might be a result of the low attendance observed in our study.
Apart from some exceptions,24 our results are consistent with other previous studies.25–28 The comparison with previous literature however is limited for two main reasons: 1) most of the previous studies were conducted in the U.S., a country with a healthcare system considerably different from the Spanish; and 2) with the exception of the study by Chapin et al.,21 the studies are significantly different to ours in terms of the type of intervention examined and population targeted.
Consistent to previous studies,24–28 most participants in this study presented multiple comorbidities and low social support. The intervention produced better results in patients with higher levels of social support. Part of the intervention consisted in encouraging patients to discuss with their relatives the results displayed in their DSMRS, which could have been a facilitating factor. In order to successfully tackle social inequalities in health however, the identification of effective strategies for patients with lower levels of social support is very much needed. Similarly, the intervention produced better results in patients without comorbidities. Adequate diabetes self-management is especially challenging in patients with multiple chronic conditions. The impact of multimorbidity on quality of care (including self-care) is an area of growing interest in primary care.29 Although there is still little scientific evidence regarding what constitutes high quality healthcare for patients with multiple conditions, our intervention is in line with available recommendations, since its main aim is to improve patient-practitioner communication.
A systematic review by members of our team30 identified a set of common characteristics of successful interventions in promoting adequate self-management, which included simple, face to face, and individually delivered; based on cognitive reframing techniques; and involving peer providers. The intervention tested in our study contained all these characteristics. Although a higher focus on cognitive techniques related to healthcare for patients with comorbidities and low social support, could have produced a greater positive impact.
Diabetes care in Spain, as in other developed countries, is increasingly expensive. It has been estimated that patients with T2DM in Spain use between 2 and 6 times more direct resources than patients with other long-term conditions.3 Differences in resources and healthcare costs between the intervention and the control group were minimal; the only additional costs in the intervention group were the take home prints offered to the patients. The average appointment duration were not different in both the intervention and control groups, and no additional testing or materials were used in the intervention group. Although we have not carried out a formal cost-effectiveness analysis, the feasibility and minimal cost of this intervention would permit its implementation as part of routine healthcare in those areas with higher proportion of patients with low educational levels.
This study is one of the first clinical trials in Spain to evaluate an intervention conducted in the primary care setting to improve health outcomes in a group of socially vulnerable patients. Despite of the high number of studies published each year highlighting the existence of important social inequalities in health in Spain, up to date there has been little interest in designing, implementing and evaluating strategies aiming to improve the health of disadvantaged groups. There is no doubt that clinical trials in primary care are complex and more susceptible to bias than clinical trials in more controlled settings. However, simple interventions in the primary care setting such as the one describe here can be widely and easily implemented, and have the potential to benefit a large proportion of the population. More research in this area is therefore essential.
This study analysed an intervention implemented in a primary care setting to improve diabetes self-management in patients with a low educational level. The results suggested that the intervention produced a modest improvement in glycaemic control, although no significant improvements were observed in the secondary outcomes examined. More research is needed to identify effective strategies that can be implemented in primary care to contribute to tackling social inequalities in health in patients with diabetes.
People diagnosed with diabetes present important clinical complications. This is especially important in people with low socioeconomic status because they have difficulties to perform a suitable diabetes self-management.
What does this study add to the literature?Although the improvement in the outcomes were not significant, taking into account the feasibility and easy to perform this intervention, more research need to be realized to identify the keys elements to better understanding of the relationship between health and diabetes self-management, in diabetes mellitus type 2 patients.
Alberto Ruano-Ravina.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsC. Bermúdez Tamayo, G. Pastor Moreno, J. Bolívar Muñoz, I. Ruiz Pérez and IRC designed the study. F. Quesada Jiménez, P. Cruz Vela, A.M. de los Ríos Álvarez, M.A. Prados Quel, E. Moratalla López, S. Domínguez Martín and J.A. Lopez de Hierro were involved in data analysis and interpretation. A. Olry de Labry Lima and M. Johrid carried out the statistical analysis. C. Bermúdez Tamayo, G. Pastor Moreno, J. Bolívar Muñoz, I. Ruiz Pérez, A. Olry de Labry Lima, M. Johrid and I. Ricci Cabello conducted the literature searches and wrote a draft of the manuscript. All results were discussed among the authors. All authors contributed to and have approved the final manuscript.
Trial registrationClinical Trials U.S. National Institutes of Health, NCT01849731.
Protocol accessiblehttps://clinicaltrials.gov/ct2/show/NCT01849731?term=NCT+01849731&rank=1
FundingRegional Health Ministry (Andalusia, Spain). The funder of this study had no role in study design, data analysis, data collection, data interpretation, or writing of the report.
Conflicts of interestOne of the authors (C. Bermúdez Tamayo) belongs to the Gaceta Sanitaria editorial committee, but was not involved in the editorial process of the manuscript.
The authors gratefully acknowledge funding of this research from the Regional Health Ministry, Andalusia (Spain).











