




To document the differences in low birthweight in different population subgroups and to analyze its possible relationship with fetal mortality rates in Spain.
MethodWe used the microdata on live births and stillbirths since 1975 to 2020 from the Spanish National Statistics Institute to examine differentials in delivering a low birthweight controlling for different sociodemographic variables and to determine the relationship between low birthweight and fetal mortality. No statistical analysis was necessary beyond the calculation of percentages and rates.
ResultsThe data at our disposal for Spain confirm the historical increase in the incidence of low birthweight and allow us to link trends in low birthweight with a decrease in the fetal mortality rate. When fetal mortality is high, the incidence of low birthweight is low, given that a natural selection effect takes place.
ConclusionsThe surprising historical increase in the incidence of low birthweight in Spain can be explained by the improvement in mortality rates. As more fetuses of lower gestational age are born alive, cases of low birthweight also increase.
Documentar las diferencias en el bajo peso al nacer en diferentes subgrupos de población y analizar su posible relación con las tasas de mortalidad fetal en España.
MétodoUtilizamos los microdatos de los nacimientos y abortos desde 1975 hasta 2020 del Instituto Nacional de Estadística de España para examinar las diferencias en los nacimientos con bajo peso controlando por distintas variables sociodemográficas y conocer su relación con las tasas de mortalidad fetal. No ha sido necesario llevar a cabo ningún tipo de análisis estadístico, más allá del cálculo de porcentajes y tasas.
ResultadosLos datos disponibles para España confirman el incremento histórico en la incidencia del bajo peso al nacer y permiten vincular las tendencias en el bajo peso con el descenso en la tasa de mortalidad. Cuando la mortalidad fetal es alta, la incidencia del bajo peso al nacer es baja, debido a que tiene lugar un proceso natural de selección.
ConclusionesEl sorprendente incremento histórico de la incidencia del bajo peso al nacer en España puede ser explicado por la mejoría de las tasas de mortalidad. Al nacer vivos más fetos de menor edad gestacional, también se incrementan los casos de bajo peso al nacer.
Birth weight is the somatometric measure that is most widely used as an indicator for the healthcare conditions of a population. The World Health Organization defines low birthweight as referring to children born alive weighing less than 2,500g (or less than 5 lb, 8 oz.), regardless of the length of gestation. There is now a large volume of evidence concerning the relationship between low birthweight (LBW) and neonatal mortality and infant morbidity.1
Although most babies born with LBW do not have a clear etiology, a series of sociodemographic factors related to the characteristics of the newborns and their mothers have been identified that could have a significant influence. In the studies carried out to date in Spain,2–7 the incidence of low birth weight is usually classified according to the nationality and marital status of the mother and the order, gestational age and sex of the newborn. Some other studies analyze both the level of education and the type of work performed by the parents.8–14 It is surprising therefore that the numerous articles published on this subject make no mention of the relationship that exists between the fetal mortality rate and the prevalence of LBW. In many developed countries, somewhere between two-thirds and three-quarters of all stillbirths are preterm and generally LBW. Both fetal growth restriction and preterm birth are important risk factors for stillbirth.15
It would seem obvious that there must be some relationship between the incidence of fetal mortality and that of LBW. It is beyond doubt that fetal mortality belongs to a process of selection through which some fetuses are born alive. Our research hypothesis, therefore, is that we have to find a negative relationship between both variables: at times when fetal mortality increases, only the strongest fetuses (and probably those that weigh most) are born alive, and so the percentage of those born with LBW is likely to be lower. In the opposite case, when improvements in obstetrics mean that even fetuses that are less developed and weigh less are born alive, we would expect the percentage of neonates with LBW to increase.
The main aims of this study are: 1) to document the differences in LBW in specific population groups, and 2) to analyze the possible relationship between fetal mortality rates and those of LBW in Spain.
MethodTo perform this research, we made use of the information in the microdata available in the Boletín estadístico de parto (Statistical Bulletin on Births) from 1975 to 2020. These databases are available on the website of the Spanish Instituto Nacional de Estadística (National Statistics Institute) (INE) (20.9 million births). INE began to collect information concerning birth weight in 1980.
In the present study, from 2007 onwards, we include in the group of “foreign mothers” those who, albeit being in possession of Spanish nationality when their child was born, had obtained this nationality by a process of naturalization. In these cases, we assigned them the nationality of their country of birth. As our aim is to identify whether the difficult socioeconomic conditions experienced by many immigrant mothers influences the incidence of LBW, it would seem reasonable not to include foreign mothers from western countries (western Europe, Canada, United States, Australia and New Zealand) in the same group as women from other regions of the world.
To calculate the fetal mortality rates, we also used the microdata from the Boletín estadístico de muertes fetales tardías (Statistical Bulletin of Late Fetal Deaths) published by INE since 1975 (99,478 fetal deaths). It is important to take in account that a not insignificant percentage of stillbirths is not registered in Spain.18
In this paper, it was not necessary to carry out any statistical analysis beyond the calculation of percentages and rates. Data on low birth weight and fetal mortality are analyzed ecologically. No personal data was used. Only the anonymized databases of the Spanish INE on births and fetal deaths were used. We downloaded the microdata available on the website: https://www.ine.es/.
As a result of the increasingly frequent use of assisted reproduction techniques, the percentage of children born in multiple births has increased continually in Spain: 1.67% (1975-1979), 2.83% (1996-2000) and 3.87% (2016-2020). The incidence of LBW among multiple births is much higher than for singleton deliveries. According to INE's microdata on births, 5.7% of the children born in singleton deliveries in the period 1996-2020 had LBW compared to 59.6% of those born in multiple deliveries. To facilitate the analysis of LBW rates, in the present study we will only take singleton births into account.
Before 1996, no information was collected about the mother's nationality. For this reason, for some indicators only the data from that year will be presented.
If our aim is to assess how improvements in medicine and healthcare have impacted on birth outcomes, we consider that the best solution is not to present a graph showing the historical trends concerning one indicator such as the percentage of LBW for the population as a whole, because as it is well known,2,7 a series of sociodemographic variables conditions the incidence of LBW. If we did this, we would not know whether the changes that we might observe were caused by possible improvements in obstetric healthcare or simply by changes in the different sociodemographic variables involved. In the present study we therefore classified the incidence of low birthweight according to the following variables: the nationality and marital status of the mother and the order, gestational age and sex of the newborn.
We determine whether any correlation is present between historical trends in the percentage of low birthweight and those for fetal mortality.
ResultsTo control as far as possible for the effect of the different sociodemographic variables on the percentage of LBW neonates, the most reasonable approach is to set out the historical development of this indicator in a disaggregated way for different population subgroups. Our results are shown in Figures 1 to 4.
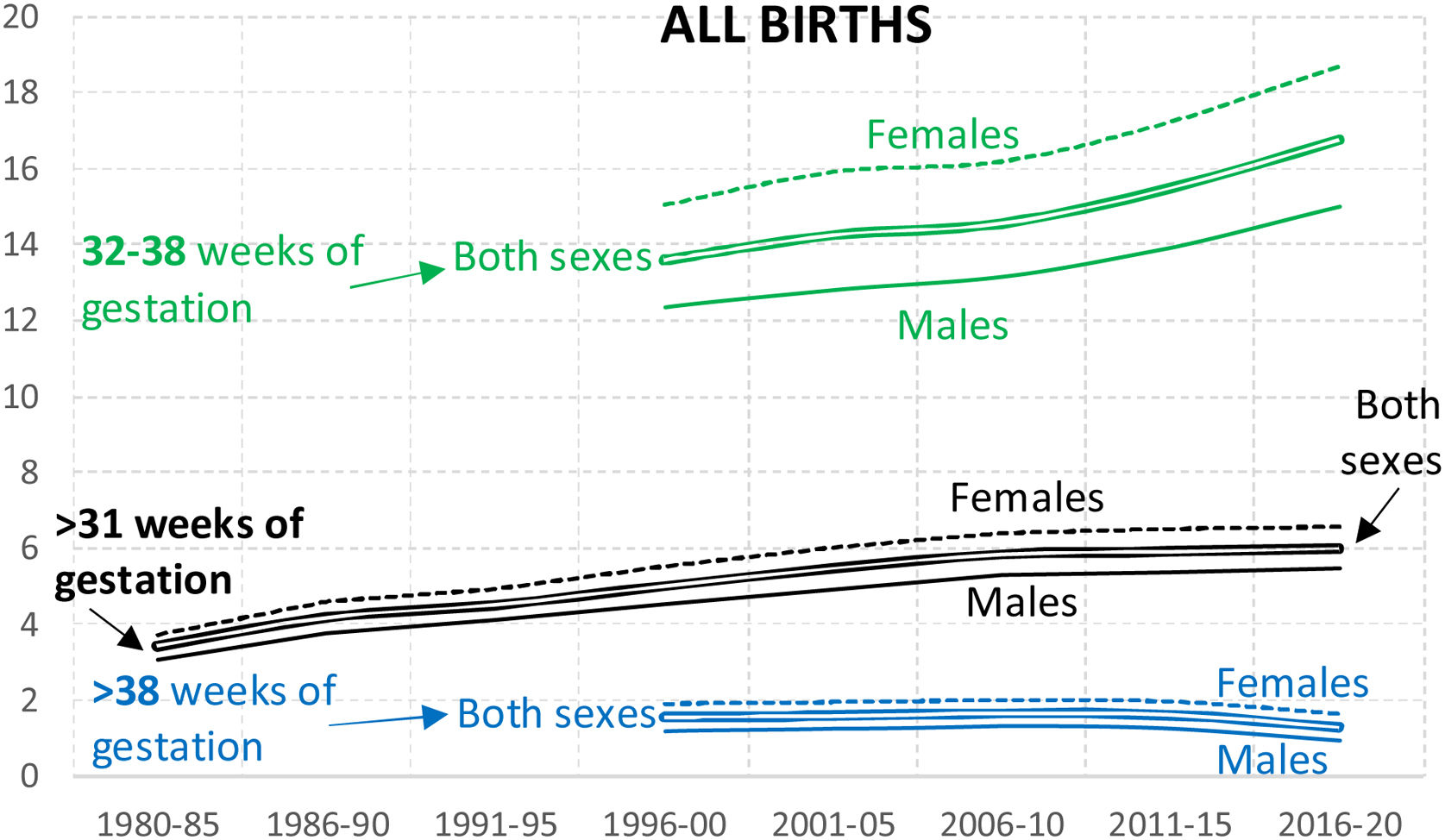
Figure 1 compares the evolution of the data between the first and last years with available information (1996-2000 and 2016-2020), and suggests that there are three major groups regarding gestational age, which have developed in very different ways. While the incidence of LBW in children born aged<32 weeks and>38 weeks has fallen in the last 25 years, that for neonates born between 32 and 38 weeks has increased sharply. Given that neonates born at <32 weeks in the period 1996-2020 scarcely represent 0.67% of all live births, we believe that the most appropriate approach is to focus on analyzing the other two gestational age groups.

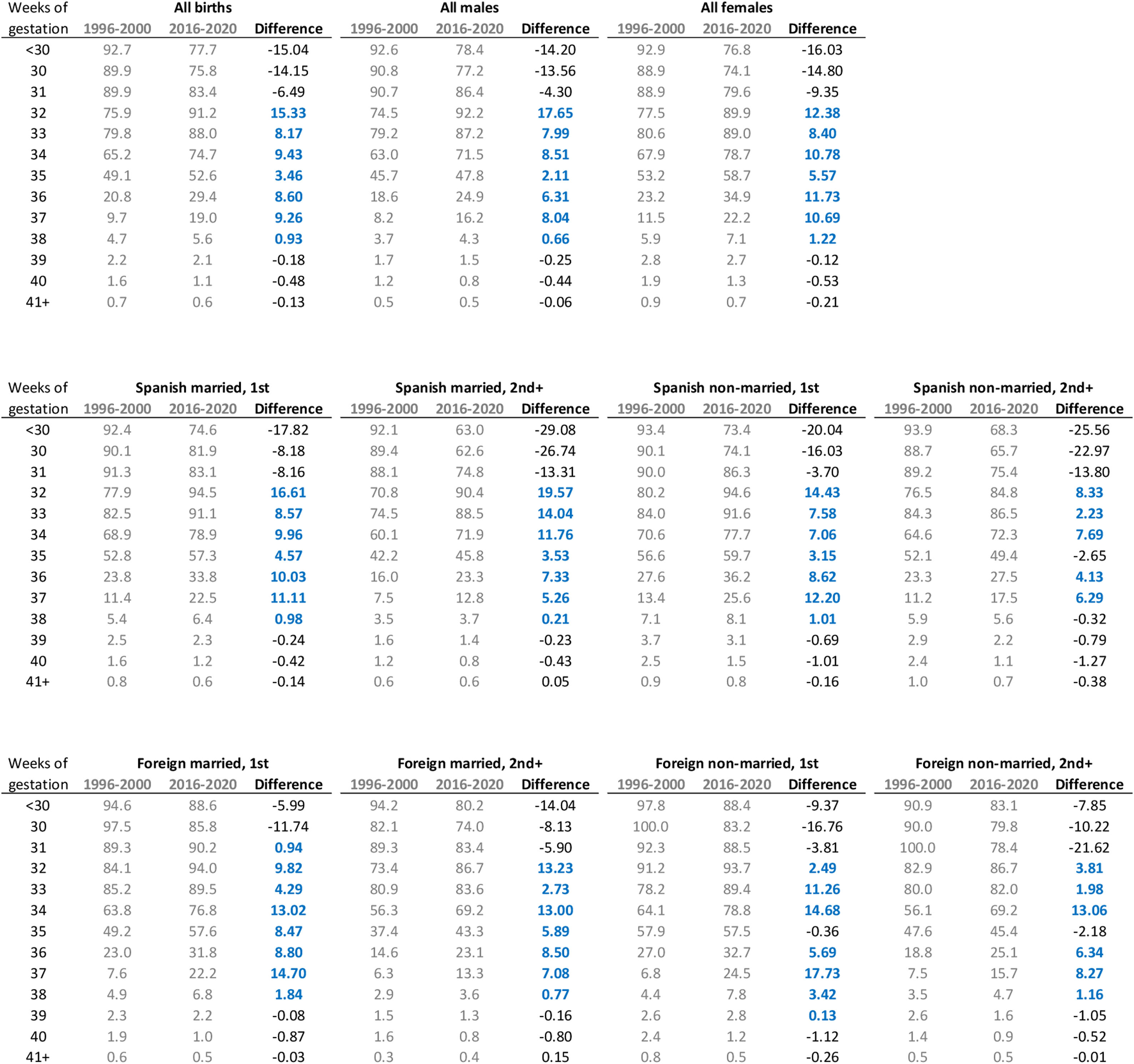
In broad terms these are the main conclusions that we can draw from Figures 2, 3 and 4:
- •
The percentage of LBW among singleton births has risen constantly in Spain since records exist. While in the early 1980s they accounted for only 3.4%, in 2006-2010 they represented 5.8%. From 2006-2010 to 2016-2020 these values clearly stabilize.
- •
The incidence of LBW is higher for females than males in all the population groups throughout the period analyzed.
- •
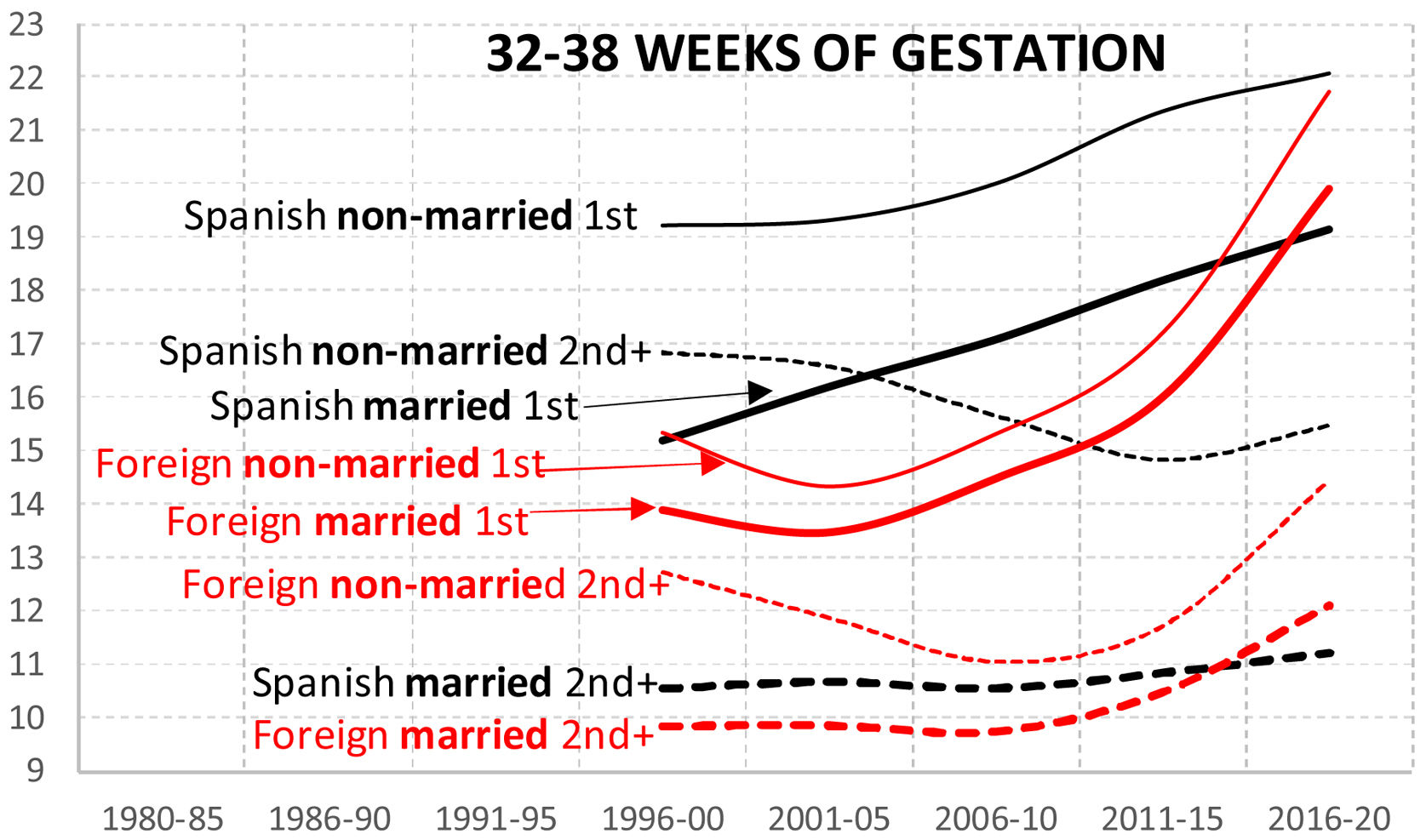
Except for the group of “Spanish non-married 2nd+”, the other groups of neonates born at 32-38 weeks have seen an increase in the incidence of LBW.
- •
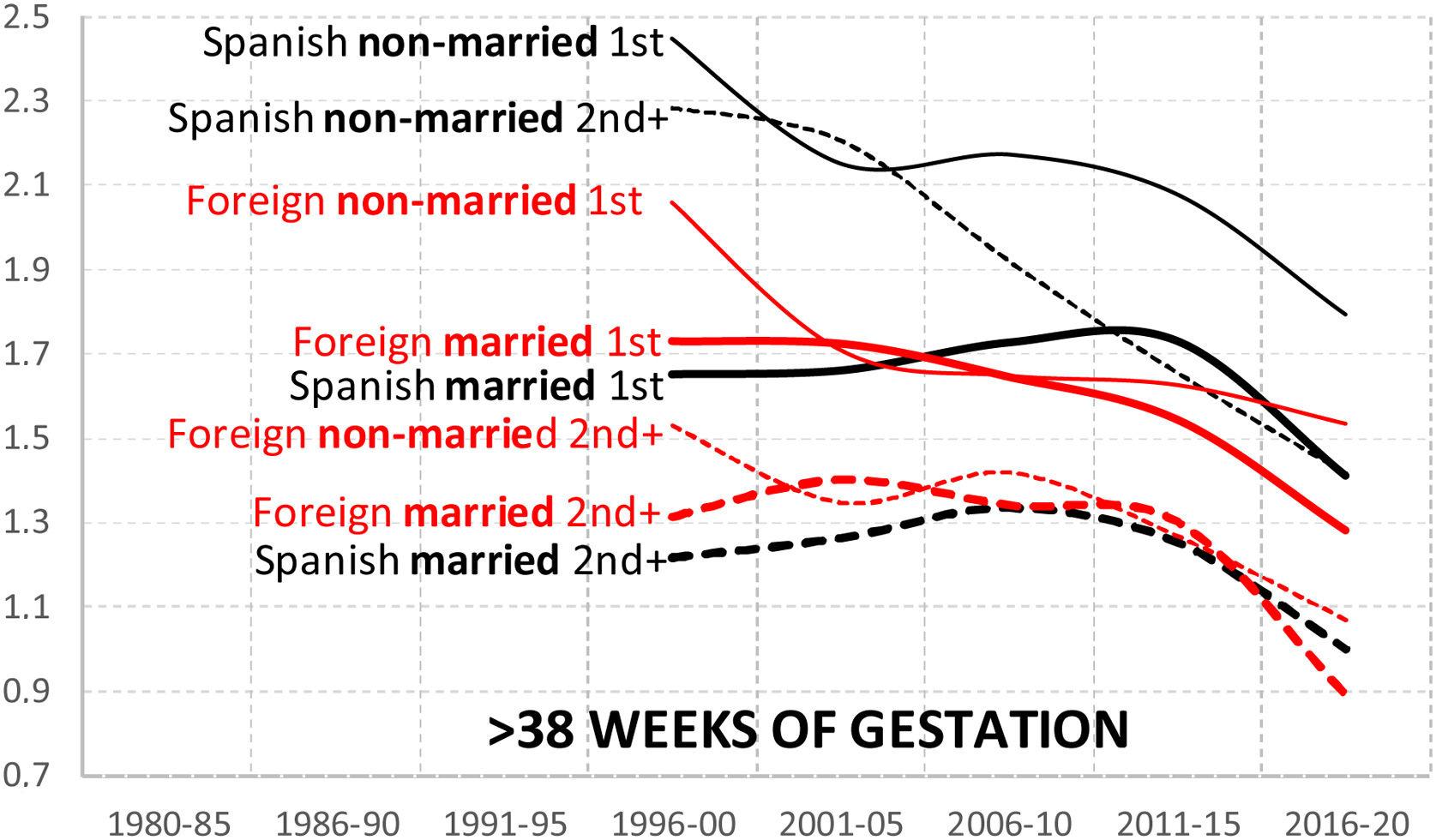
The groups of neonates born at>38 weeks of gestation saw a slight reduction in the incidence of LBW between 1996 and 2020 (somewhat less than 1%).
- •
Over time, in the two gestational subgroups (32-38 and>38 weeks) we can observe a marked process of convergence in the incidence of LBW with respect to the marital status and geographical origin of the mothers.
- •
Without doubt, the greatest differences in the prevalence of LBW among the different population groups are to be found among first order births and second and subsequent order births.
- •
Unmarried mothers have a much higher likelihood of having a child with LBW than their married counterparts.



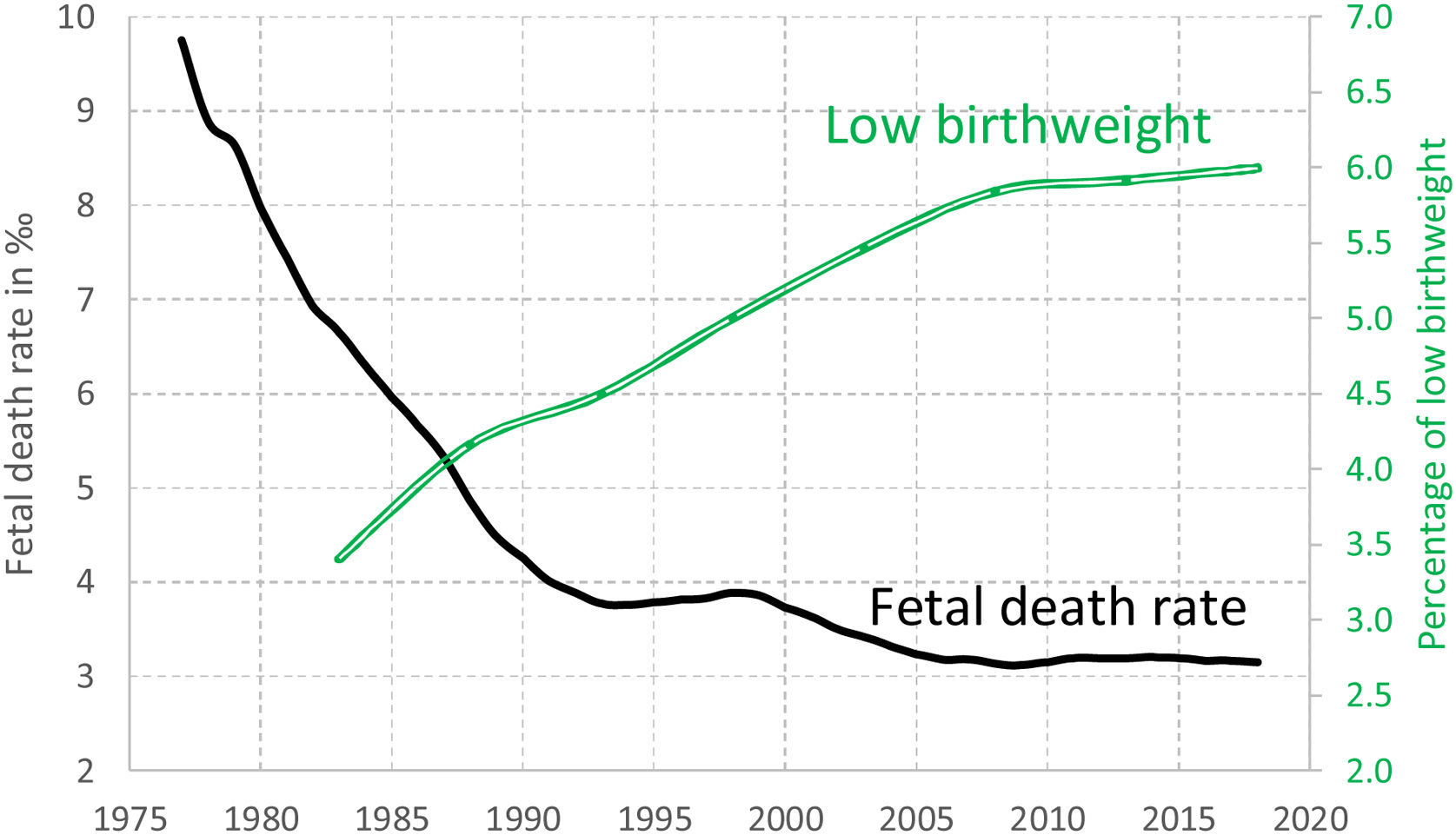
Figure 5 shows us both how the fetal mortality rate evolved and how the percentage of children born with LBW developed in Spain. The coefficient of correlation between the two variables is very high (−0.93; R2=86%), that is, the evolution of both variables over time follows a very similar pattern. The estimates made by Luque-Fernández et al.16,17 and Cassidy18 on historical developments in late fetal mortality rates are very similar to ours.

We should take in account that a not inconsiderable percentage of late fetal deaths is not registered in Spain.18 For this reason, the fetal mortality figures shown in Figures 5 and 6 should be regarded as merely indicative. Nonetheless, the aim of these figures is not to determine exactly what these rates are, but to detect differences observed between different population subgroups. If we accept that under-registration is similar in each of the subgroups, the rates can be very useful for making comparisons.

To calculate the fetal mortality rates, we included all stillbirths registered without restrictions concerning the gestational age (most of the cases older than 27 weeks of gestation). The fetal mortality rate relates the number of stillbirths with the total number of births (alive and dead) expressed in ‰.
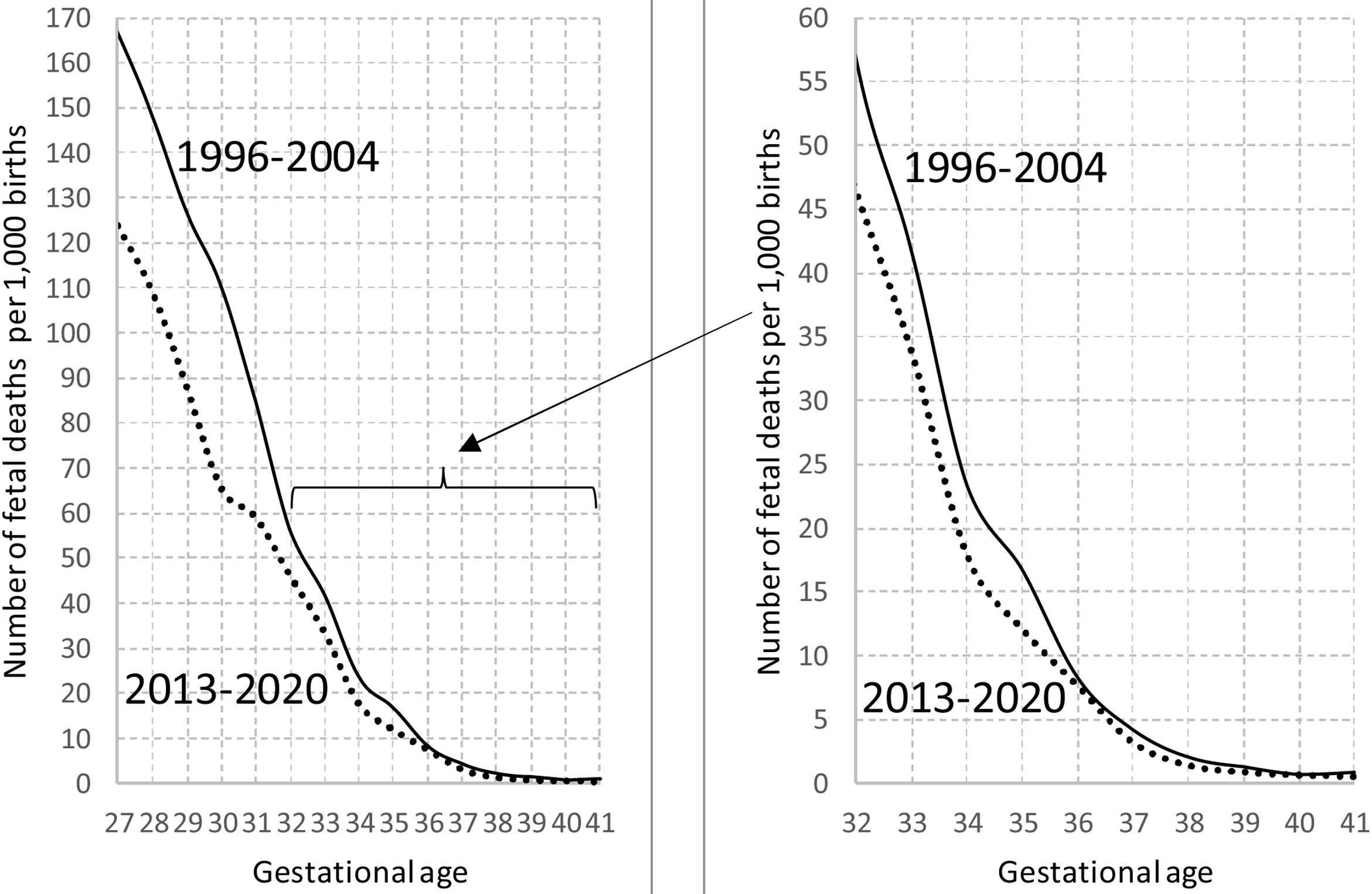
It is also possible to link the increase in the percentage of LBW among those born at 32-38 weeks of gestation (see Figures 1 to 4) to the reduction in fetal mortality. Figure 6 shows us that the gestational age-specific mortality rates (GASMR) also declined during this period.
The incidence of LBW among children born at>38 weeks has remained almost stable (it scarcely fell by 1% between 1996 and 2020). We can see that the GASMR in this gestational age group barely changed in the period 1996-2020.
DiscussionFigures 2 to 4 confirm that, as in most western countries, in Spain there has been a generalized tendency for the percentage of LBW to increase. Although the size of the increase varies according to population group, it is obvious that there is one or more other factor that may have affected all the population subgroups and that could have made the percentage of births with LBW increase, particularly between 1980 and 2006-2010.
What reasons have been put forward to explain this historical trend in the percentages of LBW?
Financial crisisEiríksdóttir et al.19 for the Icelandic population, Carolan-Olah and Barry20 for the Irish population, and Juárez and Revuelta-Eugercios21 and Terán et al.4,5 for the Spanish population associate the financial crisis with a decline in perinatal health indicators. They relate such crises to a greater prevalence of LBW. However, when we observe the evolution of this indicator over a long time period (Figures 2 to 4), it would be hard to associate the increase in the prevalence of LBW from 1980 onwards with any specific economic crisis. The real gross domestic product per capita in Spain in $2011 in 1980 was $14,008; in 2010 it was $31,786 and in 2018 it was $31,497.22 It is not appropriate to associate a decline in economic conditions with the rise in the percentage of LBW over the last few decades.
ParadoxSome researchers have expressed surprise about this apparently illogical development, and have been swift to describe it as “paradoxical”. Terán et al.3 assure us that “in Spain and other developed countries we have seen the paradox of a worsening of neonatal indices in the period of economic growth prior to 2008” (p. 65). According to Castro-Martín,2 “the recent upward trend in low birthweight goes against what we would expect to observe, given the improvement in living standards and health care, but it has also been observed in several developed countries” (p. 875). Castro-Martín2 also agrees that this situation can be described as an “apparent paradox”, and advances five possible explanations for this unexpected development:
- •
The number of multiple births has increased as a consequence of the increase in fertility treatments.
- •
As a result of the decline in fertility rates, the proportion of first order births has risen.
- •
The percentage of children born to unmarried mothers has increased.
- •
Mean age at maternity has risen.
- •
The rise in the prevalence of smoking among pregnant women might also partially account for the increase in low birthweight.23
However, these arguments find no basis in the data that are at our disposal. For example, as Figures 2 to 4 show, among children born at 32-38 weeks of gestation, the percentage of LBW has grown:
- •
Even when we only take into consideration singleton births.
- •
Even when we separate first order births from second and subsequents order births.
- •
Even when married and unmarried mothers are separated.
- •
Even when age at motherhood is neutralized by means of standardization. Table I in the on-line Appendix shows that when the mothers’ ages are standardized, the percentages of LBW vary very little (less than 3%).
The percentage of urban population in Spain exposed to concentrations of PM10 (one of the principal air contaminants) that exceed the daily limit has plummeted: 99.6% (in 2000), 75.8% (2005), 1.3% (2010), 7.04% (2015) and 1.9% (2019).24 Along similar lines, the National Health Surveys carried out by INE have detected a steady decline in the women aged over 15 who smoke on a daily basis or occasionally in Spain: 24.7% (2003), 23.9% (2006), 22.8% (2011) and 20.1% (2017).25
Numerous studies26–30 point to the positive relationship between contamination levels and the incidence of low birthweight in Spain. We do not question this relationship. However, we do question whether the historical increase in the incidence of low birthweight can be attributed, as CSIC researcher Castro-Martín2 suggests, to an increase in the percentage of women who smoke or to worsening air quality in Spain. The data available clearly indicate that fewer and fewer women smoke and that the main air pollutants have continued to decrease (substantially) in Spain.
Fetal mortalitySo what may be the reason for the increase in children born with LBW, particularly in 1980-2006, over the whole of the population in Spain? Surprisingly, in the studies that have been carried out on this subject in Spain (and elsewhere) no reference has been made to the possible impact of trends in fetal mortality rates on the incidence of LBW.31,32
It should come as no surprise that new medical technology used in pregnancy could be influencing tendencies in the incidence of LBW. The main hypothesis of the “medical technology theory” is that technological advances in obstetrics and neonatology have reduced fetal mortality.33 We might expect that when fetal mortality is high, the incidence of LBW would be low, given that a natural selection effect is taking place: the more fragile fetuses (those of lower gestational age and lower weight) would be more likely to die before birth, whereas the stronger ones (generally those of more advanced gestational age and greater weight) would represent a higher percentage of the total number of all liveborn children.
The converse of this is that when technological advances in obstetrics mean that even fetuses with greater health problems (which are also smaller and have a lower gestational age) are born alive, it would be logical to assume that the percentage of children with LBW would be higher.34
Improvements in obstetric care have succeeded in reducing the GASMR with lower gestational ages, that is, they are now saving a larger percentage of the lives of fetuses with low birthweight that might previously have been stillborn. The immediate consequence of this is that the percentage of children born with LBW has risen.
In short, the data at our disposal for Spain allow us to link the historical evolution of the incidence of LBW (both as a percentage of all births and as a percentage of those born at 32-38 weeks of gestation) with a decrease in the fetal mortality rate. This “apparent paradox”, as some researchers have called the increase in the percentage of LBW over recent decades,2,3 is therefore merely the logical consequence of the improvement in fetal mortality rates.
In addition to those inherent to the use of ecological data (ecological fallacy), the main limitations of this study are related to the reliability of the data used (especially those related to the intensity of fetal mortality). However, the similarity between our rates and those from previous studies carried out by other researchers allows us to be confident concerning their temporal trends.
ConclusionsIn this paper, we made use of the databases of the Spanish National Statistics Institute regarding births and late fetal deaths from 1975 to 2020. It was not necessary to carry out any statistical analysis beyond the calculation of percentages and rates.
Although the possible influence of fetal mortality rates on LBW has traditionally been ignored, we have shown that this variable should definitely be taken in account. By including this variable in our analysis, we have been able to explain some apparent paradoxes, such as the fact that the percentage of children with LBW increases despite the improvements in obstetric healthcare. It is beyond doubt that fetal mortality has a selective effect on the children who are born alive. If medical progress allows more fetuses with a younger gestational age to be born alive, the immediate result will be that the percentage of children born with LBW will rise. We should therefore expect to find a negative relationship between the fetal mortality rate and the incidence of LBW.
This negative relationship over time between fetal mortality and LBW does indeed come to light even when we analyze some sociodemographic variables such as the sex, birth order and gestational period of the newborn child, or the nationality and marital status of the mother.
Given the major consequences that LBW has on the future health of newborn infants, it is necessary to study this phenomenon in more depth and conduct further research that will enable us to understand better the influence of fetal mortality on determining birth weight. For example, studies using individual data could help confirm or disprove the relationship we have found with the use of ecological data.
Availability of databases and material for replicationAll the databases used to perform this research (live births and fetal deaths) are freely available at the Spanish Instituto Nacional de Estadística (National Statistics Institute) (INE): https://www.ine.es/.
Although many articles have been published that attempt to identify the variables that might account for the prevalence of low birthweight, the causes are still not well understood. Many researchers consider it paradoxical that this has increased as obstetric healthcare services have improved.
What does this study add to the literature?We find that fetal mortality is the key to understanding historical changes in the percentage of children born with low birthweight.
What are the implications of the results?Solving the apparent paradoxes about low birthweight raised by many researchers can help to better understand the etiology of this phenomenon.
Carlos Álvarez-Dardet.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsJ.J. Sánchez-Barricarte designed the study and carried it out. A. Sánchez-Arlegui provided methodological support and contributed in writing and discussing the results. All the authors have contributed corrections and improvements in the writing and final presentation of the study.
FundingThis study was supported by the Ministerio de Economía, Industria y Competitividad, CSO2017-83290-P (Spain).
Conflicts of interestNone.











