

To adapt the Primary Primary Care Assessment Tool-Adult Edition into the Moroccan Arabic dialect and to assess its reliability and validity from the perspective of Moroccan adult patients.
MethodA committee of experts carried out the cross-cultural adaptation of the Primary Care Assessment Tool. The adapted questionnaire was subject to forward and backward translation and a pilot study. Exploratory factor analysis assessed the internal consistency, reliability, and construct validity of items and scales. Finally, descriptive statistics were performed on the final factor structure.
ResultsA 43-item Moroccan Arabic dialect version of the Primary Care Assessment Tool-Adult Edition was developed. It consisted of six multi-item scales that represented the four main dimensions of primary care: first contact, continuity, comprehensiveness, and coordination. Four derived dimensions were included: cultural competence, communication, advice, and community orientation. All six scales demonstrated robust internal consistency, item-total solid correlations, and construct validity. The calculated Cronbach's alpha coefficients ranged from 0.78 to 0.90.
ConclusionsComprehensive metric analyses supported the reliability and validity of the Moroccan Arabic dialect version of the Primary Care Assessment Tool-Adult Edition in assessing core primary care domains from the patients’ experience. This tool could be used for future research on primary care in Morocco.
Adaptar la Herramienta de Evaluación de Atención Primaria para Adultos al dialecto árabe marroquí y evaluar su fiabilidad y validez desde la perspectiva de pacientes adultos marroquíes.
MétodoUn comité de expertos realizó la adaptación transcultural de la Herramienta de Evaluación de Atención Primaria. El cuestionario adaptado fue sometido a traducción directa e inversa y a un estudio piloto. El análisis factorial exploratorio evaluó la consistencia interna, la fiabilidad y la validez de constructo de los ítems y escalas. Finalmente, se realizaron estadísticas descriptivas sobre la estructura factorial final.
ResultadosSe elaboró una versión en dialecto árabe marroquí de 43 ítems de la Herramienta de Evaluación de Atención Primaria para Adultos. Consiste en seis escalas de múltiples ítems que representan las cuatro dimensiones principales de la atención primaria: primer contacto, continuidad, integralidad y coordinación. Se incluyeron cuatro dimensiones derivadas: competencia cultural, comunicación, consejo y orientación comunitaria. Las seis escalas demuestran una sólida consistencia interna, correlaciones totales sólidas de ítems y validez de constructo. Los coeficientes alfa de Cronbach calculados variaron de 0,78 a 0,90.
ConclusionesLos análisis métricos exhaustivos respaldan la confiabilidad y la validez de la versión en dialecto árabe marroquí del Instrumento de Evaluación de Atención Primaria Edición para Adultos al evaluar los dominios centrales de la atención primaria desde la experiencia de los pacientes. Esta herramienta podría ser utilizada para investigaciones futuras sobre la atención primaria en Marruecos.
Primary care (PC) is the first level of professional care where people present their health issues, and most therapeutic and preventive health needs can be met.1 It is now well established that improving PC positively impacts population health. It is associated with improved outcomes in public health promotion programs, lower costs, and higher efficiency.2–4 Furthermore, their advancement enables professionals to promote the health monitoring of the population they serve, improve health care utilization, and improve the quality of care.3,4
In Morocco, the first health reform was implemented under the 1981-1985 action plan focused on PC.5 Over a 40-year horizon, PC has been emphasized further in the Health Plan 2025, giving it priority within the framework of a service-based approach centered on the citizen.6 Furthermore, Morocco's healthcare system is divided into two sectors: the public sector, which includes health resources from the Ministry of Health, the Royal Armed Forces, local authorities, and other ministerial departments, and the private sector, which includes two subsets, one of which is non-profit and includes health resources from the National Social Security Fund, and mutual organizations. The second is for-profit and is made up of private healthcare resources organized and directed individually or collectively by healthcare professionals.7
In the Moroccan public sector, healthcare is provided at three distinct levels. Community health centers (CHC) comprise the primary level, concentrating on health promotion, preventive measures, and treatment. Provincial and regional hospitals are secondary, delivering specialized services, including emergency, oral, and mental health care. The tertiary level comprises university hospital centers, which, beyond specialized care, offer highly specialized treatments like bone marrow transplantation.8,9 Up until now, more than 20% of total health expenses have been borne by households. The ongoing challenge is to merge the various mandatory health insurance plans into a single, national, and universal basic scheme.10
Despite Morocco's long reform process in the early 1980s, the Ministry of Health intends to review the current service delivery model. It intends to make family medicine the primary mode of healthcare delivery. This approach should emphasize aspects such as continuity of care, a patient-centered approach, the provision of a package of essential services based on disease burden, the use of electronic medical records, and the use of technologies to lighten activities, particularly in PC. These factors will improve care quality by making it more integrated and patient-centered, facilitating the professional-patient relationship and reducing the current level of mistrust.9
In this regard, many countries have widely adapted and used the Primary Care Assessment Tool (PCAT) in patient surveys.11–20 The PCAT aims to provide an overall assessment of PC and its accomplishments in accessibility, continuity, comprehensiveness, and coordination. It also evaluates other aspects, such as family orientation, community orientation, and cultural competence.21
PC evaluation has not been established in Morocco due to a significant need for evaluation tools.22 Thus, it seems judicious that we consider in the current reform the evaluation of PC performance to describe, compare, and monitor services from the patients’ perspective, knowing that several instruments have been developed to structure this evaluation in a standardized manner.21,23,24
In Morocco, dialectal Arabic (dariža) is the mother tongue of Arabic speakers and is spoken by nearly 50% of the Amazighs.25 Thus, this study aimed to translate and culturally adapt the PCAT-AE to the Moroccan context. On the other hand, to assess the psychometric properties of the adapted version in PC from the perspective of Moroccan patients.
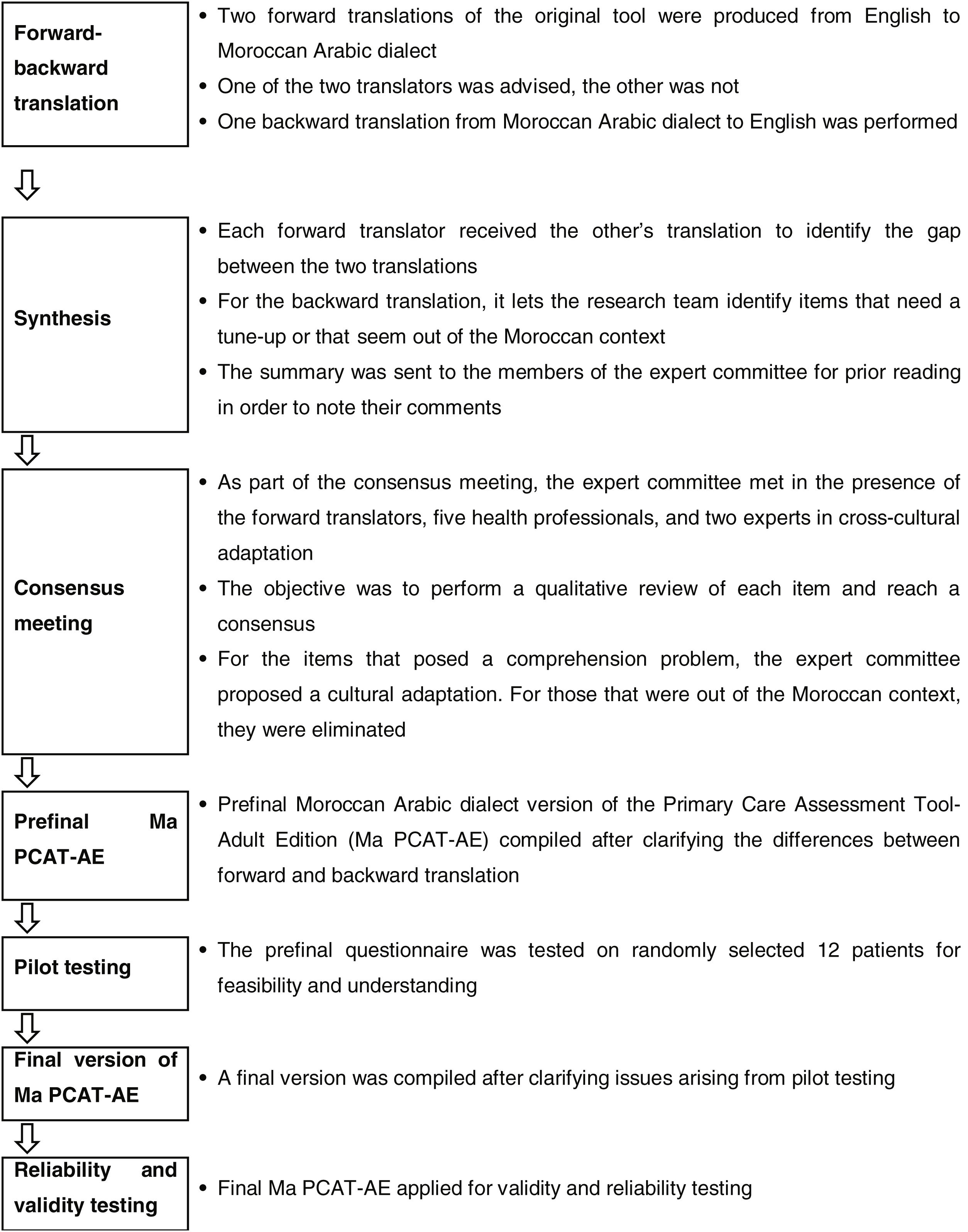
MethodTranslation and cross-cultural adaptationThe authors granted permission to adapt the instrument. The forward-backward translation method was used in the adaptation process.19 An English teacher and a healthcare professional whose mother tongue is Moroccan Arabic dialect independently performed two forward translations from English to Moroccan Arabic dialect. During a meeting with the study coordinator and the group of experts, a consensus version was reached. A bilingual healthcare professional with no knowledge of the original English version performed the back-translation (Fig. 1).

The panel of experts was made up of a general practitioner, a nurse, an English teacher, two users of PC settings, two epidemiologists and a resident doctor in public health. The committee reviewed all versions and came to an agreement on the differences. A convenience sample of 12 patients was used for the pretest. The final version was then used for validation with no changes.
Validation study- 1)
Subjects
Participants were recruited from two CHC in Marrakech, selected randomly among the 54 available; one is located in an urban area and the other in a rural setting. Eligibility criteria included being at least 18 years old, having been affiliated with the CHC for a minimum of 12 months, and willingness to volunteer. Those with cognitive impairments or insufficient proficiency in the Moroccan Arabic dialect were excluded, as it presented challenges in evaluating the adapted questionnaire. Although 75 individuals received the questionnaire, only 60 completed it and gave their consent to participate in the study.
Data collection extended to other additional data such as the level of CHC, age, gender, literacy status, marital status, employment status, and social security coverage, the reason for the visit to the CHC, the possibility of a previous referral to a specialized service or a specialist doctor, and the possibility of financial difficulty in obtaining treatment.
- 2)
Instrument
The Johns Hopkins Primary Care Policy Center developed the PCAT-AE for Underserved Populations. It was created to assess adult patients’ experience in PC.21 It has been adapted in several countries, including Spain,16,26 China,13,18 South Korea,17 and Malawi.12 The instrument has 74-items and takes about 40minutes to complete. It can be administered over the phone, in person, or by mail. The PCAT-AE includes six scales that represent the four PC domains (first contact, continuity, coordination, and comprehensiveness), namely first contact-accessibility, first contact-utilization, continuity of care, coordination of services, comprehensiveness-services available and comprehensiveness-services received, and the two sub-domains community orientation and cultural competence.21
All items are represented by a 4-point Likert scale (1=definitely not, 2=probably not, 3=probably, and 4=definitely, with the additional option «Don’t know/can’t remember» also available.21 The response «Don’t know/can’t remember» and the missing data received a neutral value of 2.5 during analyses in order to be consistent with methods used in other countries.12,13 The total score for each domain is calculated by adding the values (in reverse order, if applicable) of all domain items.21
- 3)
Statistical analysis
The statistical analyses were carried out using the SPSS software (Version 25.0). The data were described using means and standard deviation for quantitative variables and frequency distributions for qualitative variables. Before proceeding with the exploratory factor analysis, the overall Kaiser-Meyer-Olkin (KMO) statistic and Bartlett's test for sphericity were performed to assess whether the sample size was large enough to perform a satisfactory factor analysis. Otherwise, the determination of the structure of the scale and the reduction of the items was based on several steps.
First, we used factor analysis to explore the structure of the PCAT-AE items and examine its construct validity. The correct number of common factors was obtained based on the initial exploratory factor analysis. The results from this initial factor analysis were further tested using principal factor analysis and Varimax rotation. Factor loadings>0.60 were considered meaningful and used as criteria for item selection.
Secondly, the internal reliability of consistency was examined by Cronbach's alpha coefficient and item-total correlation. For a scale to be considered sufficiently reliable, an alpha value of 0.80 is recommended. All the retained items should exceed the minimum acceptable item-total correlation of 0.30.
Thirdly, the Likert scaling assumptions were tested by assessment of item-convergent validity. The item-convergent validity was tested by item-scale correlations. We defined an item-scale correlation of 0.30 as the lowest acceptable value.
Ethical considerationsThe study protocol was reviewed and approved by the University Hospital Ethics Committee of the Faculty of Medicine of Marrakech (Reference: 021/20). The participants received information about the study, and their informed consent was collected, as established by the Declaration of Helsinki.
ResultsCross-cultural adaptationIn general, the adaptation process revealed some items that could cause patients and users confusion. However, the expert committee was able to work through these issues in order to reach consensus, keeping in mind that the Ma PCAT-AE will not be self-administered due to the high proportion of illiteracy in the target population. The expert panel was required to reach two separate decisions by consensus based on the qualitative analysis. On the one hand, the items that are difficult to understand were the subject of reformulation. Items that do not correspond to the Moroccan context, on the other hand, have been completely removed (see online Appendix A).
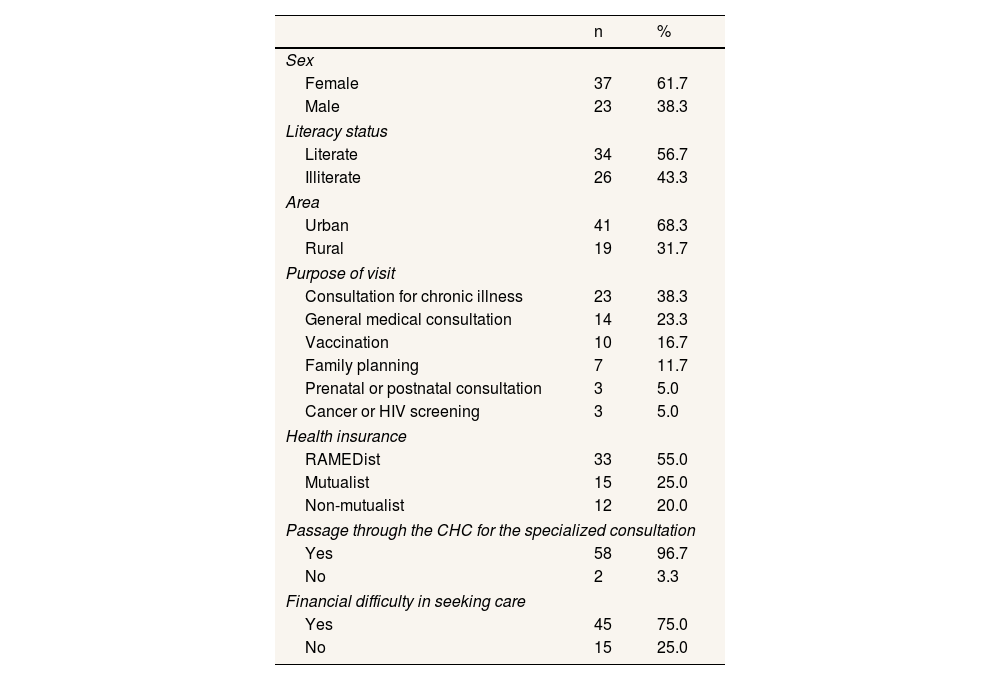
Characteristics of the sampleIn total, 75 eligible patients were invited to participate in the study, and 80% (n=60) of them completed the questionnaire. The average age was 53.7±14.45 years (range: 23-77). Table 1 shows the sociodemographic characteristics of the 60 study participants: 61.7% were female, 43.3% were illiterate, 55% were covered by the Medical Assistance Regime (RAMED), and 68.3% were from urban areas. Most study participants (38.3%) consult for a chronic illness. In addition, most respondents (96.7%) confirm going through the CHC before having a specialized consultation, and 75% confirm having financial difficulties in accessing care.
Sociodemographic characteristics of participants.
| n | % | |
|---|---|---|
| Sex | ||
| Female | 37 | 61.7 |
| Male | 23 | 38.3 |
| Literacy status | ||
| Literate | 34 | 56.7 |
| Illiterate | 26 | 43.3 |
| Area | ||
| Urban | 41 | 68.3 |
| Rural | 19 | 31.7 |
| Purpose of visit | ||
| Consultation for chronic illness | 23 | 38.3 |
| General medical consultation | 14 | 23.3 |
| Vaccination | 10 | 16.7 |
| Family planning | 7 | 11.7 |
| Prenatal or postnatal consultation | 3 | 5.0 |
| Cancer or HIV screening | 3 | 5.0 |
| Health insurance | ||
| RAMEDist | 33 | 55.0 |
| Mutualist | 15 | 25.0 |
| Non-mutualist | 12 | 20.0 |
| Passage through the CHC for the specialized consultation | ||
| Yes | 58 | 96.7 |
| No | 2 | 3.3 |
| Financial difficulty in seeking care | ||
| Yes | 45 | 75.0 |
| No | 15 | 25.0 |
CHC: community health center; HIV: human immunodeficiency virus; RAMED: Medical Assistance Regime for economically disadvantaged persons.
- 1)
Reliability tests
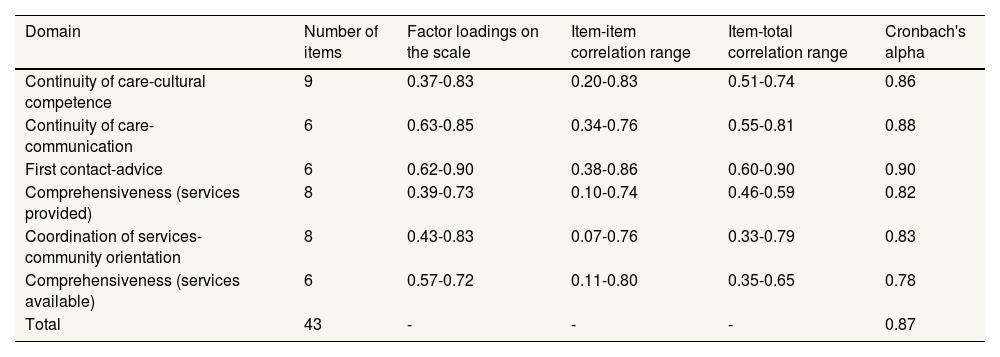
Cronbach's alpha coefficient for the 43-items is 0.87, which is higher than the reference value of 0.70 (Table 2).
- 2)
Exploratory factor analysis
Results of the exploratory factor analysisa and the internal consistency of the Ma PCAT-AE (n=43).
| Domain | Number of items | Factor loadings on the scale | Item-item correlation range | Item-total correlation range | Cronbach's alpha |
|---|---|---|---|---|---|
| Continuity of care-cultural competence | 9 | 0.37-0.83 | 0.20-0.83 | 0.51-0.74 | 0.86 |
| Continuity of care-communication | 6 | 0.63-0.85 | 0.34-0.76 | 0.55-0.81 | 0.88 |
| First contact-advice | 6 | 0.62-0.90 | 0.38-0.86 | 0.60-0.90 | 0.90 |
| Comprehensiveness (services provided) | 8 | 0.39-0.73 | 0.10-0.74 | 0.46-0.59 | 0.82 |
| Coordination of services- community orientation | 8 | 0.43-0.83 | 0.07-0.76 | 0.33-0.79 | 0.83 |
| Comprehensiveness (services available) | 6 | 0.57-0.72 | 0.11-0.80 | 0.35-0.65 | 0.78 |
| Total | 43 | - | - | - | 0.87 |
Exploratory factor analysis with Varimax rotation on data from 60 respondents was used to create and identify the PC domains of the Ma PCAT-AE. A factor loading greater than 0.35 was considered meaningful and used as a criterion for retaining items. In addition, each retained factor should have at least three items with loadings greater than 0.35.11 Thus, the exploratory factor analysis enabled the extraction of six common domains in the Ma PCAT-AE by rotating the Varimax. Furthermore, the remaining 43-items account for 65.4% of the variance in the components (see online Appendix B).
- 3)
Construct validity
The results of the rotated matrix after factoring the main axis, six common factors were extracted based on the initial exploratory factor analysis and were named “continuity of care-cultural competence”, “continuity of care-communication”, “first contact-advice”, “comprehensiveness (services provided)”, “coordination of services-community orientation” and “comprehensiveness (services available)”.
In order to ensure the ease of use of the tool, the items were reduced. To do this, we selected items with high factor loadings (>0.60) on the other factor analyses. As shown in Table 2, the inter-item correlations ranged from 0.07 to 0.86 and the factor loadings ranged from 0.37 to 0.90.
- 4)
Internal consistency
Cronbach's alpha scores ranged from 0.78 (comprehensiveness-services available) to 0.90 (first contact-advice) for all multi-item domains reviewed. Item-total correlation ranged from 0.33 to 0.90, far above the standard of 0.30 (Table 2).
- 5)
Descriptive feature of Ma PCAT-AE
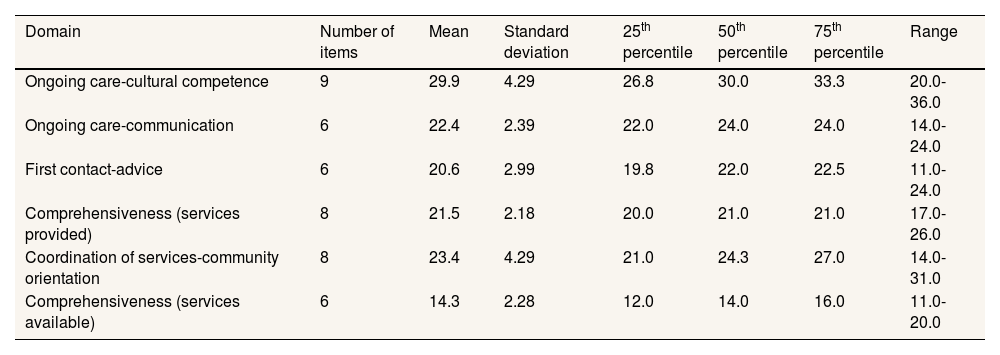
The estimates of central tendency and dispersion of score distribution for the six domains. The percentage of respondents scoring at the floor or ceiling was acceptably low for all domains (Table 3).
Descriptive characteristics of the Ma PCAT-AE.
| Domain | Number of items | Mean | Standard deviation | 25th percentile | 50th percentile | 75th percentile | Range |
|---|---|---|---|---|---|---|---|
| Ongoing care-cultural competence | 9 | 29.9 | 4.29 | 26.8 | 30.0 | 33.3 | 20.0-36.0 |
| Ongoing care-communication | 6 | 22.4 | 2.39 | 22.0 | 24.0 | 24.0 | 14.0-24.0 |
| First contact-advice | 6 | 20.6 | 2.99 | 19.8 | 22.0 | 22.5 | 11.0-24.0 |
| Comprehensiveness (services provided) | 8 | 21.5 | 2.18 | 20.0 | 21.0 | 21.0 | 17.0-26.0 |
| Coordination of services-community orientation | 8 | 23.4 | 4.29 | 21.0 | 24.3 | 27.0 | 14.0-31.0 |
| Comprehensiveness (services available) | 6 | 14.3 | 2.28 | 12.0 | 14.0 | 16.0 | 11.0-20.0 |
This study developed the Ma PCAT-AE (see online Appendix C), a 43-item instrument, to assess the performance of PC in Morocco. It consists of six scales that measure the four core PC domains and two derived domains from the original tool, “community orientation” and “cultural competence”. The tool is concise, enhancing its administrative efficiency, though there are even shorter versions internationally.12,13,16,18,19 It could serve as a PC evaluation tool, which would be fundamental for improving the health process and actions.21,27
The Ma PCAT-AE effectively assesses all essential PC domains, aligning with other studies that maintained these domains.12,19,20 However, it does not retain the “first contact-utilization” subdomain, a trend observed in other adaptations.11,12,19 Most PC users may not require facilities to be open on weekends, but such accessibility could benefit specific groups, like full-time workers.28 The integration of “cultural competence” and “community orientation” into existing domains reflects the progressive adaptation of PC in Morocco.21
The Ma PCAT-AE exhibited high internal reliability, evidenced by a Cronbach's alpha of 0.90 and an intra-class correlation of 0.90. Its item-total range of correlations, from 0.13 to 0.46, is larger than the original tool's range of 0.18 to 0.3821 and comparable to the ranges in other studies.12,29 Factor analysis of the Ma PCAT-AE identified six main factors with an eigenvalue ≥1, explaining 65.4% of the total variance, which aligns with the Chinese version.13 These findings underscore the Ma PCAT-AE's balance between universal evaluation criteria and localized healthcare dynamics.
Despite these strengths, the study faces limitations. The sample size, though validated by a KMO of 0.5 and Bartlett's test (p <0.01), included a 43.3% illiteracy rate among respondents, which could impact the interpretation of specific questions. The findings, supported by Muniz et al.,30 suggest that small samples can still yield conclusive results in cross-cultural adaptation processes even with small samples as small as 50 individuals. Analyses and tests conducted in these cases allow the identification of more than half of the test items exhibiting significant or even very significant differential item functioning.
While the four core domains of the original PCAT are generally preserved, they have experienced certain modifications. A sub-domain of the first contact was removed, and another was expanded with an additional derived domain, namely “advice”. The domain of continuity of care was divided into two distinct sub-domains, each enhanced with its own derived domain (cultural competence and communication). The coordination of services domain was combined with the derived domain “community orientation”. Notably, the two sub-domains of the comprehensiveness remained untouched. This type of structural modifications have been made in other studies.11,12,14,17,26,29,31,32 They are particularly crucial in cross-cultural adaptations, necessitate strict adherence to well-defined guidelines. This is imperative to ascertain the adapted instrument's psychometric robustness and cultural appropriateness, as cited by Beaton et al.33
In conclusion, this study is pioneering in Morocco, marking the first attempt to validate a Moroccan Arabic dialect version of the PCAT-AE. The Ma PCAT-AE emerges as an empirically validated instrument, marking a significant step towards the context-specific PC evaluation in Morocco.
Future research efforts should focus on extending the validation of the Ma PCAT-AE to a broader audience and in various contexts in Morocco. Comparative analyses involving varied populations and contexts will enrich the tool's validity, ensuring its adaptability and relevance to the country's complex and diverse healthcare landscape.
In summary, while the Ma PCAT-AE has demonstrated its initial validity and effectiveness, a comprehensive national validation is paramount to affirm its efficacy, reliability, and utility as a standard tool for assessing and enhancing PC in Morocco. Such national validation will bolster the credibility and applicability of the Ma PCAT-AE but also provide a robust foundation for data-driven, patient-centric improvements in PC tailored to the unique needs, challenges, and opportunities inherent in Morocco's healthcare system.
Availability of databases and material for replicationThe data is made available to people on request from H. El Mouaddib (h.elmouaddib.ced@uca.ac.ma) following the data policy applicable by the Ethics Committee of the University Hospital of the Faculty of Medicine of Marrakech.
Primary care's positive impact on health and efficiency is well-known. Assessing primary care is crucial to meet population needs. The Primary Care Assessment Tool is a top instrument for comprehensive primary care assessment, noted for cross-cultural adaptability and effectiveness in evaluating key domains.
What does this study add to the literature?This article covers the cross-cultural adaptation of the Primary Care Assessment Tool for Morocco, filling a gap in evaluating the first level of its healthcare system.
What are the implications of the results?The Moroccan Arabic dialect version of the Primary Care Assessment Tool-Adult Edition is a validated instrument for assessing primary care in Morocco, benefiting local and regional researchers with a rigorously developed, adaptable resource.
Carlos Álvarez-Dardet.
Transparency declarationThe corresponding author on behalf of the other authors guarantee the accuracy, transparency and honesty of the data and information contained in the study, that no relevant information has been omitted and that all discrepancies between authors have been adequately resolved and described.
Authorship contributionsAll authors contributed to the conception, design, and writing of this article. Specifically, H. El Mouaddib coordinated the project and wrote the first version of the manuscript with M. Sebbani and M. Amine. H. El Mouaddib collected the data. M. Sebbani and A. Mansouri conducted the statistical analysis with the technical support of L. Adarmouch and M. Amine. All authors were involved in the interpretation of the data as well as the revision process of the article. All authors have read and approved the final version of the manuscript.
AcknowledgementsThe authors thank the survey participants and the expert panel for their enormous contribution to this study. A special mention goes to Dr. Leiyu Shi and his team for agreeing to use their tool.
FundingNone.
Conflicts of interestNone.









