

To analyse doctors’ opinions on clinical coordination between primary and secondary care in different healthcare networks and on the factors influencing it.
MethodsA qualitative descriptive-interpretative study was conducted, based on semi-structured interviews. A two-stage theoretical sample was designed: 1) healthcare networks with different management models; 2) primary care and secondary care doctors in each network. Final sample size (n = 50) was reached by saturation. A thematic content analysis was conducted.
ResultsIn all networks doctors perceived that primary and secondary care given to patients was coordinated in terms of information transfer, consistency and accessibility to SC following a referral. However, some problems emerged, related to difficulties in acceding non-urgent secondary care changes in prescriptions and the inadequacy of some referrals across care levels. Doctors identified the following factors: 1) organizational influencing factors: coordination is facilitated by mechanisms that facilitate information transfer, communication, rapid access and physical proximity that fosters positive attitudes towards collaboration; coordination is hindered by the insufficient time to use mechanisms, unshared incentives in prescription and, in two networks, the change in the organizational model; 2) professional factors: clinical skills and attitudes towards coordination.
ConclusionsAlthough doctors perceive that primary and secondary care is coordinated, they also highlighted problems. Identified factors offer valuable insights on where to direct organizational efforts to improve coordination.
Analizar la opinión de los médicos sobre la coordinación entre la atención primaria (AP) y la atención especializada (AE) en diferentes redes de servicios de salud, e identificar los factores relacionados.
MétodoEstudio cualitativo descriptivo-interpretativo basado en entrevistas semiestructuradas. Se diseñó una muestra teórica en dos etapas: 1) redes de servicios de salud con diferentes modelos de gestión; 2) en cada red, médicos de AP y AE. El tamaño muestral se alcanzó por saturación (n = 50). Se realizó un análisis temático de contenido.
ResultadosEn las tres redes, los médicos expresaron que la atención está coordinada en términos de intercambio de información, consistencia y accesibilidad de AE tras derivación urgente. Sin embargo, emergieron problemas relacionados con el acceso no urgente y cambios en prescripciones, y en dos redes la inadecuación clínica de las derivaciones entre ambos niveles. Se identificaron los siguientes factores relacionados: 1) organizativos: facilitan la coordinación, la existencia de mecanismos de transferencia de información, de comunicación y de acceso rápido, y la proximidad física que promueve actitudes positivas a la colaboración; la obstaculizan el tiempo insuficiente para el uso de mecanismos, incentivos no compartidos en la prescripción y, en dos redes, un cambio del modelo organizativo; 2) relacionados con los profesionales: habilidades clínicas y actitudes frente a la coordinación.
ConclusionesAunque los médicos perciben que la atención entre niveles está coordinada, también señalan problemas. Los factores identificados muestran hacia dónde dirigir los esfuerzos organizativos para su mejora.
Care fragmentation is considered one of the main obstacles health services have to face in the current context of rapid medical and technological breakthroughs and increasing specialization. The provision of suboptimal care in terms of quality and efficiency is associated with care fragmentation,1,2 thus clinical coordination across care levels is becoming a priority issue in health services around the world.3
This study is oriented by the conceptual framework of Vazquez et al.4,5, which considers clinical coordination an intermediate objective of healthcare networks as a means by which to reach the ultimate objectives of quality of care, efficiency and equity of access. To analyse the achievement of these objectives, both external and internal processes and contextual factors are taken into account, as well as the different perspectives (services, users).4–6 Clinical coordination is defined as the harmonious connection of the different health services needed to provide care to a patient throughout the care continuum in order to achieve a common objective without conflicts.5 Two types of clinical coordination are distinguished:7 clinical information coordination, which refers to the use of patients’ clinical information in order to harmonize activities between providers; and clinical management coordination, which refers to the provision of care in a sequential and complementary way by the different services and healthcare levels involved.
Despite the numerous interventions introduced to improve care coordination between the primary care (PC) and secondary care (SC), few evaluations are available and generally based on the analysis of indicators.6,8 Studies which focus on the opinion of health professionals usually explore their experiences in the use of coordination mechanisms. Some studies explore professionals’ perception using a qualitative approach, which tend to focus on patients with a specific condition, such as those with cancer,9,10 or mental health problems11,12 or only a specific type of transition, such as hospital discharges.13,14 These studies identify diverse organizational factors which affect clinical coordination, such as economic incentives to collaborate;11,15 as well as factors related to professionals, such as attitudes towards coordinating care and mutual knowledge.9,11,12 Little research has been conducted in the context of national health systems,16,17 which may present particular opportunities and challenges in clinical coordination.
In Catalonia (Spain), the healthcare system is characterized by a split of the financing and provision functions. The provision is the responsibility of a number of contracted providers: a public company, the Catalan Health Institute, and public consortia, municipal foundations and private (mostly non-profit) foundations.18 This diversity has originated, on the one hand, a risk of fragmentation and, on the other, different management models, including the joint management of both PC and SC.19
Previous research have approached the analysis of clinical coordination in health care networks with different management models, exploring the patients’ perceptions of continuity across care levels and quantifying the degree of clinical coordination based on the application of clinical coordination indicators.20,21 These studies pointed to high levels of continuity and coordination across care levels in Catalonia, although they also indicated room for improvement, including insufficient information transfer and long waiting times for secondary care after referral. These studies did not explore the factors influencing clinical coordination or include the perception of doctors, both scarcely analysed in the Catalan health care context.17 The aim of this article, which forms part of a wider project,6,22 is to analyse the opinions of doctors on clinical coordination between PC and SC and on the factors influencing it in different healthcare networks of the Catalan National Health System.
MethodsA qualitative and descriptive-interpretative qualitative study was conducted with PC and SC doctors.
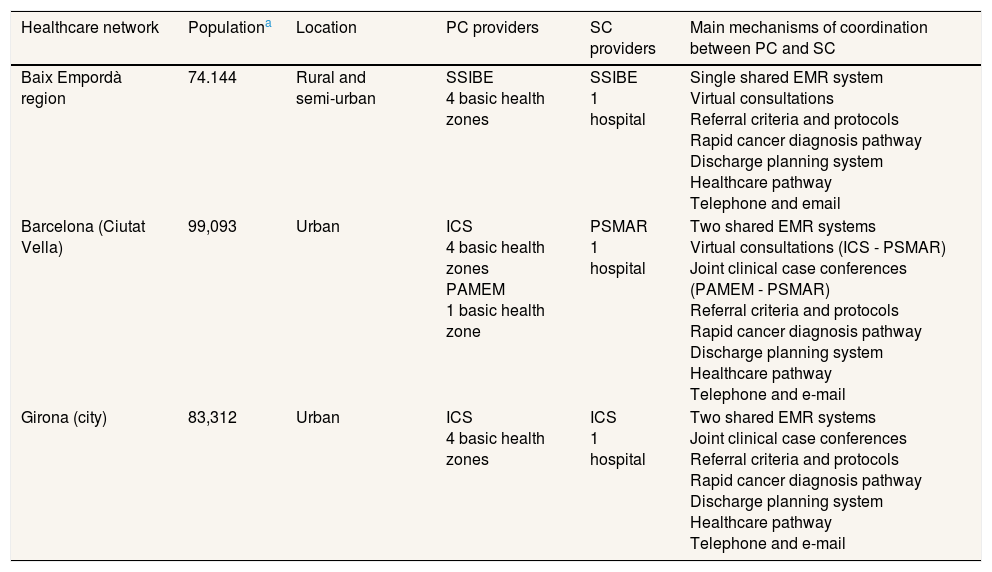
Study sampleA theoretical sample,23 i.e. criteria was defined to ensure that contexts and profiles that could provide information which is different and relevant to the study's objectives are included, was selected through a two-stage process. In the first stage, the contexts healthcare networks were selected to represent the diversity of management models in Catalonia: Baix Empordà, the city of Girona and the Ciutat Vella district of Barcelona (Table 1). A single entity manages both PC and SC in Baix Empordà and in Girona. In Ciutat Vella, two public entities manage PC and a different public entity manages SC.
Description of the healthcare networks of study.
| Healthcare network | Populationa | Location | PC providers | SC providers | Main mechanisms of coordination between PC and SC |
|---|---|---|---|---|---|
| Baix Empordà region | 74.144 | Rural and semi-urban | SSIBE 4 basic health zones | SSIBE 1 hospital | Single shared EMR system Virtual consultations Referral criteria and protocols Rapid cancer diagnosis pathway Discharge planning system Healthcare pathway Telephone and email |
| Barcelona (Ciutat Vella) | 99,093 | Urban | ICS 4 basic health zones PAMEM 1 basic health zone | PSMAR 1 hospital | Two shared EMR systems Virtual consultations (ICS - PSMAR) Joint clinical case conferences (PAMEM - PSMAR) Referral criteria and protocols Rapid cancer diagnosis pathway Discharge planning system Healthcare pathway Telephone and e-mail |
| Girona (city) | 83,312 | Urban | ICS 4 basic health zones | ICS 1 hospital | Two shared EMR systems Joint clinical case conferences Referral criteria and protocols Rapid cancer diagnosis pathway Discharge planning system Healthcare pathway Telephone and e-mail |
Population ≥18 years.
EMR: Electronic Medical Record; ICS: Institut Català de la Salut; PAMEM: Institut de Prestacions d’Assistència Mèdica al Personal Municipal; PC: Primary Care; PSMAR: Parc de Salut Mar; SC: Secondary Care; SSIBE: Serveis de Salut Integrats Baix Empordà.
Source: Registre Central d’Assegurats, 2010.
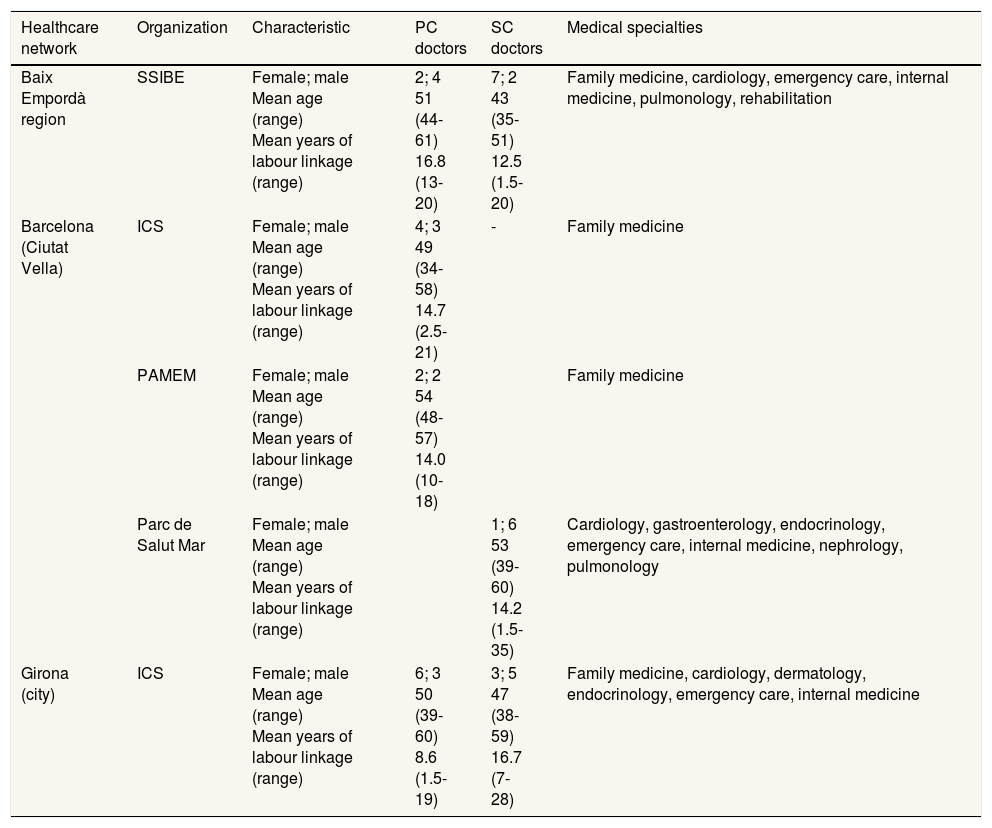
In the second stage, in each network PC and SC doctors who perform clinical activities and with a minimum labour linkage to the organization of a year and a half were selected. Maximum variation with regard to age and sex was sought, and for SC doctors also to speciality. The sample was selected in a sequential way, so profiles that emerged as relevant in initial interviews were also included in the study. No contacted doctor declined or showed reluctance to participate in the study. The final sample size was between 15 and 18 doctors per network (Table 2).
Final composition of the sample of informants.
| Healthcare network | Organization | Characteristic | PC doctors | SC doctors | Medical specialties |
|---|---|---|---|---|---|
| Baix Empordà region | SSIBE | Female; male Mean age (range) Mean years of labour linkage (range) | 2; 4 51 (44-61) 16.8 (13-20) | 7; 2 43 (35-51) 12.5 (1.5-20) | Family medicine, cardiology, emergency care, internal medicine, pulmonology, rehabilitation |
| Barcelona (Ciutat Vella) | ICS | Female; male Mean age (range) Mean years of labour linkage (range) | 4; 3 49 (34-58) 14.7 (2.5-21) | - | Family medicine |
| PAMEM | Female; male Mean age (range) Mean years of labour linkage (range) | 2; 2 54 (48-57) 14.0 (10-18) | Family medicine | ||
| Parc de Salut Mar | Female; male Mean age (range) Mean years of labour linkage (range) | 1; 6 53 (39-60) 14.2 (1.5-35) | Cardiology, gastroenterology, endocrinology, emergency care, internal medicine, nephrology, pulmonology | ||
| Girona (city) | ICS | Female; male Mean age (range) Mean years of labour linkage (range) | 6; 3 50 (39-60) 8.6 (1.5-19) | 3; 5 47 (38-59) 16.7 (7-28) | Family medicine, cardiology, dermatology, endocrinology, emergency care, internal medicine |
ICS: Institut Català de la Salut; PAMEM: Institut de Prestacions d’Assistència Mèdica al Personal Municipal; PC: Primary Care; PSMAR: Parc de Salut Mar; SC: Secondary Care; SSIBE: Serveis de Salut Integrats Baix Empordà.
Individual, semi-structured interviews were carried out using a topic guide adapted from previous studies.17,24 The topic guide addressed doctors’ opinions on clinical coordination between PC and SC and factors influencing it through open questions. Interviews were conducted by the first author, an anthropologist/pharmacist with a good knowledge of qualitative methods, the research topic and the context, who worked in close collaboration with the second and last authors. The interviews lasted between 45 and 80minutes and were recorded and transcribed.
Doctors were contacted by telephone or email either by a contact in the health organization or by the researcher. Interviews were performed in the healthcare facilities. Data collection stopped when saturation was reached in each study network. Fieldwork took place between July and September 2012 (Baix Empordà) and between December 2013 and May 2014 (Ciutat Vella and Girona).
Data analysis and quality of informationA thematic content analysis25 was conducted with the support of the Atlas-ti software. Data were segmented by healthcare network and level of care. The process of category generation was mainly inductive, i.e. it was oriented towards the identification of emergent patterns in the data.23 Themes were identified, coded, re-coded and classified, identifying common patterns by looking at regularities, convergences and divergences in data, through a process of constant comparisons, going back and forth between data. Data quality was ensured through triangulation, by comparing different networks, groups of informants, and sources (literature).
The first author was responsible for the analysis, and worked in close collaboration with the second (a health economist) and last authors (public health doctor). Differences were discussed and resolved by going back to the data. The rest of the authors contributed to the interpretation of data.
Ethical considerationsThis study was approved by the ethics committee of Parc de Salut Mar (2010/412/1). Written consent was obtained from every participant prior to interview. Confidentiality and anonymity were guaranteed.
ResultsDue to similarities in the discourse, results are presented jointly for the three healthcare networks. When existing, differences between networks are outlined.
Doctors’ experiences of clinical coordination between PC and SCIn all three healthcare networks, doctors considered that care provided to patients was generally coordinated across that levels, and described it in terms of the availability and uptake of clinical information generated at the other care level through the shared EMR, the resolution of doubts regarding diagnosis and treatment through direct communication, and rapid access to SC following a referral in urgent cases. However, certain limits to clinical coordination emerged, which varied depending on the network and care level.
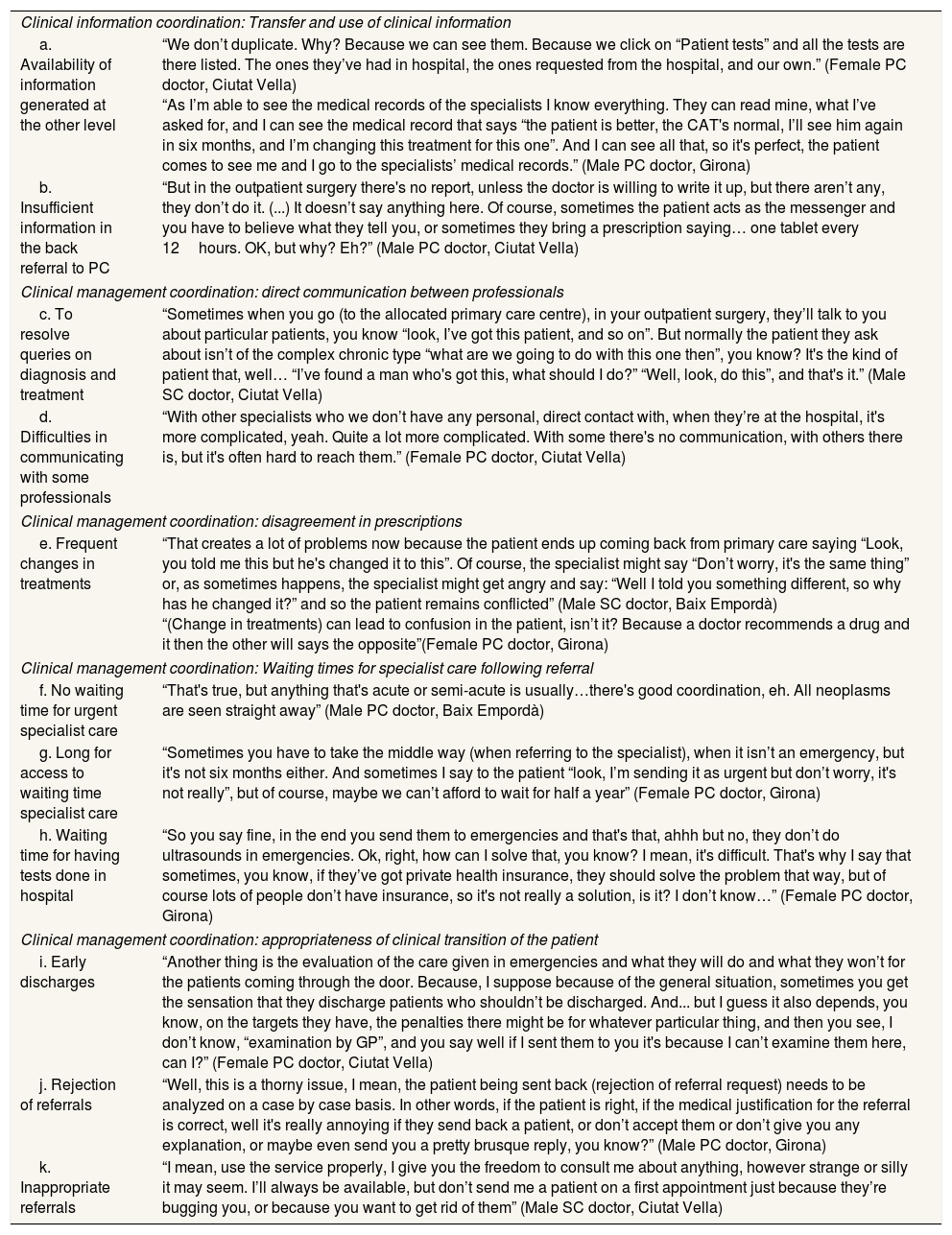
According to the informants, the availability and uptake of clinical data generated at the other level on the EMR meant that tests and treatments are not duplicated or contraindicated (Table 3 a). This information also facilitated an adequate follow up of the patient when they pass from one level to another, for example following a referral. However, doctors pointed out that some doctors from the other care level failed to transfer all the information needed in patient referral (reason for referral) and reply letters to PC (diagnoses or recommendations for follow-up) (Table 3 b).
Examples for categories of opinions on clinical coordination between primary and secondary care.
| Clinical information coordination: Transfer and use of clinical information | |
| a. Availability of information generated at the other level | “We don’t duplicate. Why? Because we can see them. Because we click on “Patient tests” and all the tests are there listed. The ones they’ve had in hospital, the ones requested from the hospital, and our own.” (Female PC doctor, Ciutat Vella) “As I’m able to see the medical records of the specialists I know everything. They can read mine, what I’ve asked for, and I can see the medical record that says “the patient is better, the CAT's normal, I’ll see him again in six months, and I’m changing this treatment for this one”. And I can see all that, so it's perfect, the patient comes to see me and I go to the specialists’ medical records.” (Male PC doctor, Girona) |
| b. Insufficient information in the back referral to PC | “But in the outpatient surgery there's no report, unless the doctor is willing to write it up, but there aren’t any, they don’t do it. (...) It doesn’t say anything here. Of course, sometimes the patient acts as the messenger and you have to believe what they tell you, or sometimes they bring a prescription saying… one tablet every 12hours. OK, but why? Eh?” (Male PC doctor, Ciutat Vella) |
| Clinical management coordination: direct communication between professionals | |
| c. To resolve queries on diagnosis and treatment | “Sometimes when you go (to the allocated primary care centre), in your outpatient surgery, they’ll talk to you about particular patients, you know “look, I’ve got this patient, and so on”. But normally the patient they ask about isn’t of the complex chronic type “what are we going to do with this one then”, you know? It's the kind of patient that, well… “I’ve found a man who's got this, what should I do?” “Well, look, do this”, and that's it.” (Male SC doctor, Ciutat Vella) |
| d. Difficulties in communicating with some professionals | “With other specialists who we don’t have any personal, direct contact with, when they’re at the hospital, it's more complicated, yeah. Quite a lot more complicated. With some there's no communication, with others there is, but it's often hard to reach them.” (Female PC doctor, Ciutat Vella) |
| Clinical management coordination: disagreement in prescriptions | |
| e. Frequent changes in treatments | “That creates a lot of problems now because the patient ends up coming back from primary care saying “Look, you told me this but he's changed it to this”. Of course, the specialist might say “Don’t worry, it's the same thing” or, as sometimes happens, the specialist might get angry and say: “Well I told you something different, so why has he changed it?” and so the patient remains conflicted” (Male SC doctor, Baix Empordà) “(Change in treatments) can lead to confusion in the patient, isn’t it? Because a doctor recommends a drug and it then the other will says the opposite”(Female PC doctor, Girona) |
| Clinical management coordination: Waiting times for specialist care following referral | |
| f. No waiting time for urgent specialist care | “That's true, but anything that's acute or semi-acute is usually…there's good coordination, eh. All neoplasms are seen straight away” (Male PC doctor, Baix Empordà) |
| g. Long for access to waiting time specialist care | “Sometimes you have to take the middle way (when referring to the specialist), when it isn’t an emergency, but it's not six months either. And sometimes I say to the patient “look, I’m sending it as urgent but don’t worry, it's not really”, but of course, maybe we can’t afford to wait for half a year” (Female PC doctor, Girona) |
| h. Waiting time for having tests done in hospital | “So you say fine, in the end you send them to emergencies and that's that, ahhh but no, they don’t do ultrasounds in emergencies. Ok, right, how can I solve that, you know? I mean, it's difficult. That's why I say that sometimes, you know, if they’ve got private health insurance, they should solve the problem that way, but of course lots of people don’t have insurance, so it's not really a solution, is it? I don’t know…” (Female PC doctor, Girona) |
| Clinical management coordination: appropriateness of clinical transition of the patient | |
| i. Early discharges | “Another thing is the evaluation of the care given in emergencies and what they will do and what they won’t for the patients coming through the door. Because, I suppose because of the general situation, sometimes you get the sensation that they discharge patients who shouldn’t be discharged. And... but I guess it also depends, you know, on the targets they have, the penalties there might be for whatever particular thing, and then you see, I don’t know, “examination by GP”, and you say well if I sent them to you it's because I can’t examine them here, can I?” (Female PC doctor, Ciutat Vella) |
| j. Rejection of referrals | “Well, this is a thorny issue, I mean, the patient being sent back (rejection of referral request) needs to be analyzed on a case by case basis. In other words, if the patient is right, if the medical justification for the referral is correct, well it's really annoying if they send back a patient, or don’t accept them or don’t give you any explanation, or maybe even send you a pretty brusque reply, you know?” (Male PC doctor, Girona) |
| k. Inappropriate referrals | “I mean, use the service properly, I give you the freedom to consult me about anything, however strange or silly it may seem. I’ll always be available, but don’t send me a patient on a first appointment just because they’re bugging you, or because you want to get rid of them” (Male SC doctor, Ciutat Vella) |
PC: primary care doctor; SC: secondary care doctor.
Doctors considered that direct communication, through virtual consultations via EMR or email, telephone, and joint clinical case conferences encouraged greater consistency in medical instructions, prevented unnecessary patient referrals and helped to speed up the diagnostic process and treatment (Table 3 c). Likewise, difficulties in communicating with certain SC doctors, translated into delays in diagnosis and treatment (Table 3 d). Disagreements regarding prescriptions also emerged, which were described as frequent changes in prescriptions from the other care level, creating confusion in patients and conflict between doctors of the two levels (Table 3 e).
The rapidity of access to SC when the reason for referral was urgent, was considered to contributes to a timely diagnosis and treatment (Table 3 f). However, PC doctors and some SC doctors considered that the waiting times for non-urgent SC and, in Girona, for hospital tests, were long, which caused delays in diagnosis and treatment and sometimes forced the patients to seek help for their problems in inappropriate places, such as hospital emergency services or PC (Table 3 g-h). In this sense, in Girona and Ciutat Vella, PC doctors considered that the patient did not always receive care in the most appropriate place due to being prematurely discharged from hospital or emergency services (Table 3 i) and, in Girona, due to the rejection of certain referrals, a factor which they also associated with delays in diagnosis and treatment (Table 3 j). However, SC doctors considered referral rejections a consequence of unnecessary referrals (Table 3 k).
Factors influencing clinical coordination across care levelsIn the informants’ discourse, various types of factors related to the organization and professionals emerged that influenced clinical coordination across care levels. The majority of these factors emerged in all networks, although with some differences in organizational factors. Differences were also observed depending on the care level, mainly in factors related to professionals.
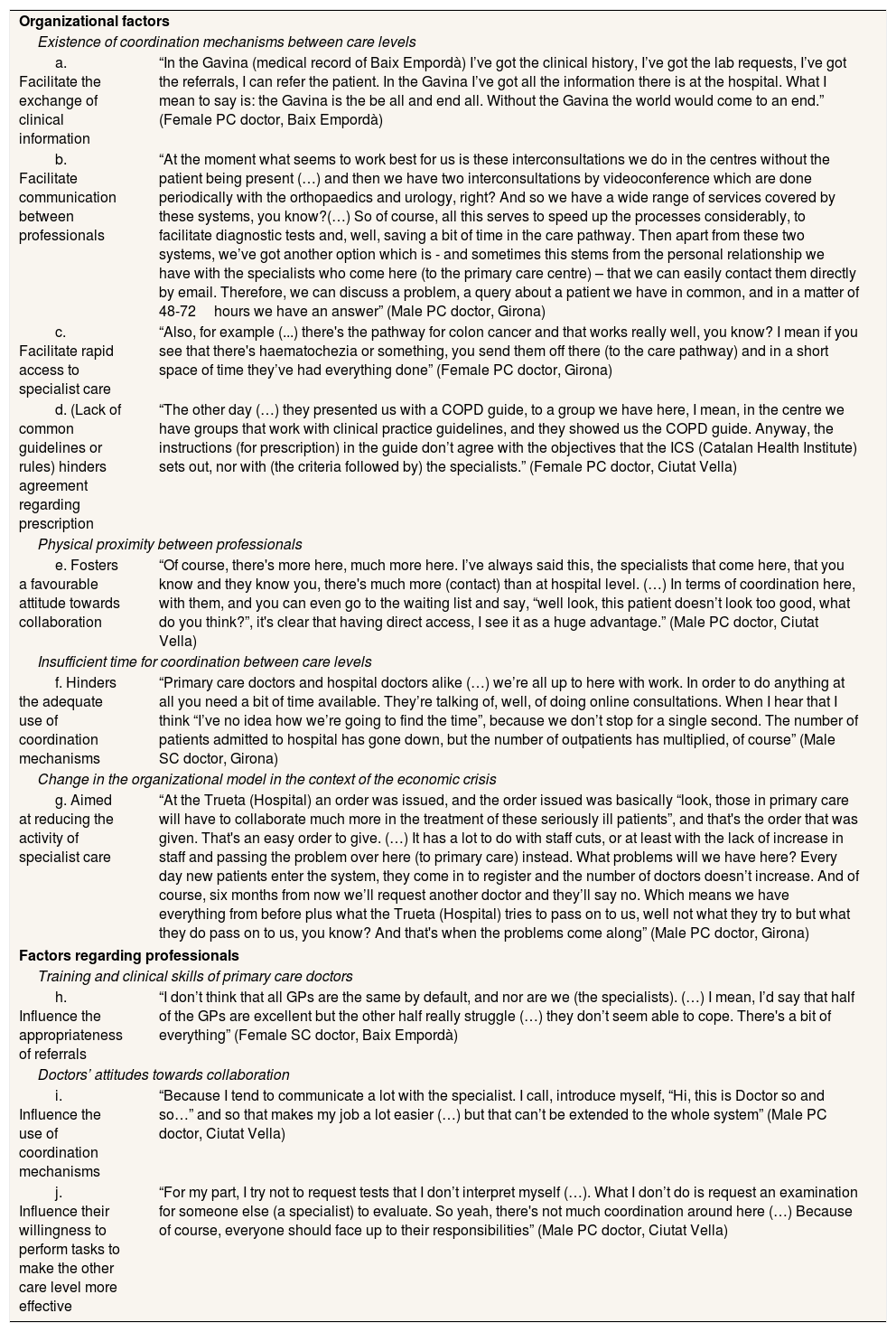
Organizational factorsThe existence of coordination mechanisms between care levels emerged as one of the main facilitators of clinical coordination between levels. They identified mechanisms that facilitate access to the information generated at the other level (shared EMR) or enable problem-solving communication and agreement on clinical approaches (clinical case conferences between PC and SC doctors [Girona], virtual consultations via EMR [Ciutat Vella and Baix Empordà] or email, and telephone [Table 4 a-b]). Joint clinical case conferences also contribute to improve mutual knowledge, both in terms of the skills and roles of the other level, fostering a more positive attitude towards collaboration. In addition, they identified the rapid diagnosis pathway for suspected cancer to guarantee rapid access to urgent SC (Table 4 c).
Examples for categories of factors that influence clinical coordination between primary and secondary care.
| Organizational factors | |
| Existence of coordination mechanisms between care levels | |
| a. Facilitate the exchange of clinical information | “In the Gavina (medical record of Baix Empordà) I’ve got the clinical history, I’ve got the lab requests, I’ve got the referrals, I can refer the patient. In the Gavina I’ve got all the information there is at the hospital. What I mean to say is: the Gavina is the be all and end all. Without the Gavina the world would come to an end.” (Female PC doctor, Baix Empordà) |
| b. Facilitate communication between professionals | “At the moment what seems to work best for us is these interconsultations we do in the centres without the patient being present (…) and then we have two interconsultations by videoconference which are done periodically with the orthopaedics and urology, right? And so we have a wide range of services covered by these systems, you know?(…) So of course, all this serves to speed up the processes considerably, to facilitate diagnostic tests and, well, saving a bit of time in the care pathway. Then apart from these two systems, we’ve got another option which is - and sometimes this stems from the personal relationship we have with the specialists who come here (to the primary care centre) – that we can easily contact them directly by email. Therefore, we can discuss a problem, a query about a patient we have in common, and in a matter of 48-72hours we have an answer” (Male PC doctor, Girona) |
| c. Facilitate rapid access to specialist care | “Also, for example (...) there's the pathway for colon cancer and that works really well, you know? I mean if you see that there's haematochezia or something, you send them off there (to the care pathway) and in a short space of time they’ve had everything done” (Female PC doctor, Girona) |
| d. (Lack of common guidelines or rules) hinders agreement regarding prescription | “The other day (…) they presented us with a COPD guide, to a group we have here, I mean, in the centre we have groups that work with clinical practice guidelines, and they showed us the COPD guide. Anyway, the instructions (for prescription) in the guide don’t agree with the objectives that the ICS (Catalan Health Institute) sets out, nor with (the criteria followed by) the specialists.” (Female PC doctor, Ciutat Vella) |
| Physical proximity between professionals | |
| e. Fosters a favourable attitude towards collaboration | “Of course, there's more here, much more here. I’ve always said this, the specialists that come here, that you know and they know you, there's much more (contact) than at hospital level. (…) In terms of coordination here, with them, and you can even go to the waiting list and say, “well look, this patient doesn’t look too good, what do you think?”, it's clear that having direct access, I see it as a huge advantage.” (Male PC doctor, Ciutat Vella) |
| Insufficient time for coordination between care levels | |
| f. Hinders the adequate use of coordination mechanisms | “Primary care doctors and hospital doctors alike (…) we’re all up to here with work. In order to do anything at all you need a bit of time available. They’re talking of, well, of doing online consultations. When I hear that I think “I’ve no idea how we’re going to find the time”, because we don’t stop for a single second. The number of patients admitted to hospital has gone down, but the number of outpatients has multiplied, of course” (Male SC doctor, Girona) |
| Change in the organizational model in the context of the economic crisis | |
| g. Aimed at reducing the activity of specialist care | “At the Trueta (Hospital) an order was issued, and the order issued was basically “look, those in primary care will have to collaborate much more in the treatment of these seriously ill patients”, and that's the order that was given. That's an easy order to give. (…) It has a lot to do with staff cuts, or at least with the lack of increase in staff and passing the problem over here (to primary care) instead. What problems will we have here? Every day new patients enter the system, they come in to register and the number of doctors doesn’t increase. And of course, six months from now we’ll request another doctor and they’ll say no. Which means we have everything from before plus what the Trueta (Hospital) tries to pass on to us, well not what they try to but what they do pass on to us, you know? And that's when the problems come along” (Male PC doctor, Girona) |
| Factors regarding professionals | |
| Training and clinical skills of primary care doctors | |
| h. Influence the appropriateness of referrals | “I don’t think that all GPs are the same by default, and nor are we (the specialists). (…) I mean, I’d say that half of the GPs are excellent but the other half really struggle (…) they don’t seem able to cope. There's a bit of everything” (Female SC doctor, Baix Empordà) |
| Doctors’ attitudes towards collaboration | |
| i. Influence the use of coordination mechanisms | “Because I tend to communicate a lot with the specialist. I call, introduce myself, “Hi, this is Doctor so and so…” and so that makes my job a lot easier (…) but that can’t be extended to the whole system” (Male PC doctor, Ciutat Vella) |
| j. Influence their willingness to perform tasks to make the other care level more effective | “For my part, I try not to request tests that I don’t interpret myself (…). What I don’t do is request an examination for someone else (a specialist) to evaluate. So yeah, there's not much coordination around here (…) Because of course, everyone should face up to their responsibilities” (Male PC doctor, Ciutat Vella) |
PC: primary care doctor; SC: secondary care doctor.
Lastly, the lack of shared clinical criteria for prescription and incentives only for PC doctors emerged as a barrier, as it makes it difficult to reach an agreement on a treatment plan for the patient (Table 4 d).
Physical proximity to each other was highlighted by doctors from both care levels as a factor that facilitates clinical coordination. Various organizational elements, which differed according to the network, ensured proximity: the co-location of SC doctors in PC centres in Ciutat Vella, working in a small organization in Baix Empordà and in centres that are close to each other in Baix Empordà and Girona. Physical proximity increases contact and mutual knowledge, fostering a more favourable attitude towards collaboration. It also facilitates informal communication and a greater use of coordination mechanisms (Table 4 e).
Insufficient time for coordination due to work overload was mentioned as the main barrier to clinical coordination by doctors from all networks. Doctors highlighted having insufficient time to use coordination mechanisms to communicate and to participate in joint meetings (Table 4 f). Furthermore, PC doctors pointed out that inappropriate referrals were a result of the insufficient consultation time per patient.
Changes in the organizational model in the context of the economic crisis emerged from the discourse of PC doctors and, with less intensity, in that of the SC doctors, in Ciutat Vella and Girona. They attributed these changes to cuts in the healthcare budget, which translated into a cut in resources (reducing the number of hospital beds). They considered that coordination mechanisms which present an alternative to conventional referrals, such as virtual consultations, were implemented with the purpose to reducing the number of patients who access SC. In addition, PC doctors perceived that hospital stays and emergency admissions have been curtailed (early discharges) and the volume and complexity of patients treated in PC had increased. Moreover, sometimes the patient was referred back to PC without the problem having been resolved (Table 4 g).
Professional factorsInsufficient training and clinical skills of PC doctors was related to clinically inappropriate referrals by some SC doctors, especially those who are not in regular contact with PC doctors (Table 4 h). However, according to PC doctors and other SC doctors, this perception is built on SC doctors prejudices and their scant knowledge of the function and the resources available at PC.
Attitudes of doctors towards coordination emerged as a factor which influences the use of coordination mechanisms: specifically, telephone and email to communicate, the EMR to share medical data and their participation in joint meetings (Table 4 i). It also influences their willingness to perform tasks aimed at making the other care level more effective, such as requesting tests so that the SC doctor can see the results on the patient's first visit (Table 4 j). The informants considered that these values are conditioned by mutual knowledge and contact between professionals, which foster a more positive attitude towards coordination.
DiscussionFew differences between networks in doctors’ perceptions of clinical coordination across care levelsIn general, doctors considered that care provided to patients is coordinated across PC and SC in all three networks, with some limitations and their perception of clinical coordination was similar across networks, although some differences were identified between networks and professionals. In two networks, Ciutat Vella and Girona, problems in the adequacy of patient care transitions in terms of early discharges and the rejection of referrals were described, mainly by PC doctors. However, these problems were attributed to changes introduced in the context of the economic crisis, thus, this difference could be due to the fact that the field work was carried out at different times: at the start of the economic crisis in Baix Empordà and over a year later in the other two networks, when the main reductions in public health spending budget took place.
Similar factors influencing clinical coordination between PC and SC in all three networksDoctors of all three networks also identify similar organizational factors; most importantly, physical proximity between doctors and the implementation of similar coordination mechanisms.
Among organizational factors highlighted by informants were the implementation of coordination mechanisms to foster information transfer and problem-solving communication. In addition, it became evident that physical proximity was important, since it promotes mutual knowledge and trust among doctors that encourage direct communication and foster a better attitude towards coordination. A positive attitude towards coordination emerges in this and other studies12,26 as one of the most relevant factors influencing collaboration among professionals, as it contributes to the better use of coordination mechanisms and makes them more willing to perform tasks destined to make care more effective at the other level.
On the other hand, the results reveal various factors, which hinder coordination across care levels. Most importantly, lack of time for coordination activities emerges as the main organizational obstacle to clinical coordination, also pointed out in the scientific literature.10,27,28. This problem seems to have become more severe as a result of the change in the organizational model, aimed at reducing the activity of SC, and change that has gone hand in hand with a higher level of referral rejections and early discharges.
The discourse highlights incentives in drug prescription, which are heavily weighted towards the PC. These incentives, along with a lack of shared prescription guidelines or a lack of awareness, lead to frequent changes in treatments. This problem points to the need to implement a more global focus involving both care levels by making doctors of both levels equally responsible for prescribing drugs to the population they serve.29,30
Finally, the three networks form part of a national health system, and thus share many of the contextual factors that can influence coordination, such as the same healthcare model; almost universal coverage and the same type of financing and incentive systems. This might be explaining the coincidence in discourses.
LimitationsDespite the heterogeneity of the population interviewed in terms of certain characteristics, such as medical speciality and type of centre, we cannot rule out the possibility that information saturation was not fully reached, although the main arguments are represented in the results. Furthermore, a contact in the organizations participated in the selection process, so they could have introduced a bias towards a more positive discourse. However, the research team also participated in the selection process, discussing the profiles of the informants, and some informants were identified in a sequential way as part of the sampling strategy. Finally, the fact that the field work in one network was performed at a different time to the other two may be the reason for the differences observed between study areas, especially those related to changes in the socioeconomic context seen in recent years.
ConclusionsThis study shows that doctors perceived that care provided to patients is generally coordinated, with similarities in the networks analysed, although it also highlights several areas for improvement. In addition, the study has allowed us to identify the factors that doctors relate to clinical coordination between care levels, with differences depending on care level and, to a lesser degree, network. The most important enablers are organizational, and among them, the implementation of coordination mechanisms that facilitate information exchange (EMR) and problem-solving communication, and those that guarantee rapid access to SC, as well as doctors’ physical proximity. Main barriers are a lack of time for coordination, the change in the organizational model in the context of the economic crisis and the existence of unshared incentives in drug prescription. Future interventions strategies for improvement in coordination across care levels should take these factors into consideration in order to guarantee a suitable and effective response to the problems encountered in clinical coordination across care levels.
Poor clinical coordination is considered to be one of the main obstacles to attaining effective healthcare outcomes in many healthcare systems. There are few evaluations that explore clinical coordination between PC and SC from the doctors’ perspective, one of the main actors in this process. Studies in the context of national health systems are even scarcer.
What does this study add to the literature?This study contributes to current knowledge by analysing coordination between PC and SC and factors influencing it from the doctors’ perspective in three healthcare networks within the context of a national health system. Future interventions addressing clinical coordination across care levels should take identified factors into consideration in order to guarantee a suitable and effective response to the encountered problems.
María del Mar García-Calvente.
Authorship contributionsM.B. Aller, M.L. Vázquez Navarrete and I. Vargas were responsible for the design of the study. M.B. Aller carried out the data collection, its analysis and interpretation, and also wrote the first draft of the manuscript. M.L. Vázquez Navarrete and I. Vargas provide support to the data collection and made substantial contributions to the analysis and manuscript. All authors participated in the interpretation of data, reviewed draft versions of the paper, and checked and approved the final manuscript.
FundingThis study forms part of the projects “Relationship between continuity and coordination of care across care levels in different healthcare environments” and “Coordination across care levels and its relationship with quality of care in different healthcare environments of the public healthcare system”, which were partly financed by the Instituto de Salud Carlos III and the European Regional Development Fund (PI10/00348 and PI15/00021). The funding source had no involvement in the study design, nor in the collection, analysis and interpretations of data, or in the writing of the article and the decision to submit it for publication.
Conflicts of interestsNone.
The authors wish to thank all informants for their thoughtful and open participation in the study. We thank Nuria Martinez and Isabel Serra for their administrative support and Kate Bartlett for her help in correcting the English version of this article.









